
Key Points
-
Highlights that maintaining denture hygiene can be difficult for infirm individuals and is often regarded as an unpleasant chore by nurses and carers.
-
Suggests that for susceptible patients infections associated with the denture biofilm can result in morbidity.
-
Shows that the denture box facilitates denture hygiene, reduces the chance of accidental damage and acts as a means of identification.
Abstract
This paper re-visits the need for patients or their carers to maintain as low a level of denture biofilm as possible. It notes that the handling of dentures is unpleasant to carers and suggests a method of reducing this contact to a minimum but yet allow efficient cleaning by means of brushing. It also highlights the potential damage that can occur due to mishandling or accident. The denture box acts as a safe storage unit and finally, it suggests that its 'footprint' allows accurate recovery in an institution where dentures can be inadvertently mingled.
Similar content being viewed by others


Introduction
The programme for the 2013 British Dental Association conference contained some 60 lectures, none of which dealt with the treatment of edentulous patients. This reflects the subject's relative absence from the literature and reinforces the perception that the need for complete dentures is waning. Nonetheless, as recently as 2009, 6% of the combined population of England, Wales and Northern Ireland were edentate and in need of prostheses.1 Most of them are 'elderly', that is 75+, and in consequence a proportion are likely to be in care homes or incapacitated to a greater or lesser degree.
The York consensus2 declared that for the edentulous mandible the minimal standard of care is the provision of an overdenture supported by two implants. However, in the recent update on guidelines for the provision of such treatment under the NHS,3 the authors note '...funding for implants on the NHS is likely to be a precious resource.' They suggest, 'the decision to provide implants needs to be balanced against alternative modes of restoration, their ease of provision, longevity and outcome rates'.
An alternative mode of restoration is the provision of optimal dentures, if necessary, at the hands of an experienced dentist. This might preclude the need for surgical intervention and is especially relevant for patients who are not amenable to surgery.4 An added benefit is that if correctly designed, the denture(s) can act as a stent for implants if they are subsequently required.
A well-made but retentively compromised complete upper denture can be stabilised with the judicious use of a dental fixative5 and severe bone resorption of either jaw too, is not necessarily a barrier to a successful outcome. The effect of a resorbed, mobile maxillary ridge can be ameliorated by a careful impression technique.6 Similarly, in the mandible a skilful technique can provide a stable denture that can be soft-lined if discomfort cannot be eliminated. The updated report3 makes provision under the NHS for patients who are intolerant to such treatment and where the implant retained or supported overdenture2 would then be treatment of choice.
The edentate state is most often the result of a lack of awareness of the importance of oral hygiene. It is therefore unlikely that attention to this will be radically altered when the teeth are replaced by dentures. Even if this is not always the case, patients may not be aware of the potential harm of the denture biofilm.
Denture plaque (DP) differs in its constituents from the normal dental biofilm.7 In the physically healthy individual it can be aesthetically objectionable with a build-up of materials found in the mouth that can produce an unpleasant odour.8 They can also induce mucosal inflammation that is, denture stomatitis, and a potentially disfiguring angular cheilitis (AC).9,10
Denture stomatitis (DS) can appear in different forms. Found typically under a maxillary denture it produces a bright red imprint of the outline of the denture on the underlying mucosa (Fig. 1). Due to a lack of symptoms, its presence is frequently unnoticed by the patient and by the dental professional.

Denture induced stomatitis under an acrylic partial denture
Not infrequently, DS is associated with AC described as a usually bilateral erythematous fissuring of the corners of the mouth (Fig. 2). The poor appearance that this produces is exacerbated by deep labial folds that encourage maceration of the corners of the mouth with saliva. These folds are often present when the vertical dimension is significantly reduced but is not a cause of the chielitis.11 AC can sometimes be a result of vitamin and iron deficiency anaemias.12

Angular cheilitis associated with the stomatitis in Figure 1
Removal of denture plaque is therefore important. The film may not be visible but its presence can be demonstrated to the patient by the use of a plaque disclosing agent (Fig. 3). The two main denture cleaning methods of brushing with a non-abrasive paste or soaking in chemicals have been reviewed.13 The authors found that there was a lack of evidence to suggest that one method was superior to the other. In the writer's opinion the demonstration of the removal of disclosed plaque by brushing is preferred to simply advising chemical soaking. However without assistance brushing becomes a problem when the patient is unable to use one hand, for example due to injury or a stroke. A possible solution is suggested below.

Using a plaque disclosing liquid and the result of simple cleaning with a brush and detergent
The healthy individual can be expected to respond to oral hygiene advice but this may not be the case with patients who are seriously infirm and/or residents in care establishments, and this can pose a serious problem. It is now recognised that dental and denture plaque allow the colonisation of respiratory pathogens.14 'Dentures should be considered an important reservoir of organisms which could colonise the pharynx, and the importance of controlling denture plaque for the prevention of aspiration pneumonia cannot be overemphasised.'15 Where rigorous oral hygiene procedures have been instituted a reduction in the rate of pneumonia and deaths has resulted.16
A Swedish study17 compared the differences in attitude to the maintenance of oral health in dependant elderly and severely disabled patients in a group of 398 health workers. They were asked regarding a) personal oral healthcare habits b) experience and attitudes in assisting oral care and c) willingness to assist patients/residents with their daily oral hygiene. This study revealed that oral care assistance is viewed as more disagreeable than other nursing activities.
Another study18 found that nursing staff considered oral care the most distasteful aspect of their work (Fig. 4). They said they would 'rather clean up after bowel movements or attend to urinary incontinence accidents than brush a resident's teeth'.

Probable cause for a carer's reluctance to handle a denture
The denture biofilm attached to removable partial dentures (Fig. 12) will place teeth at risk, in particular the abutment teeth.19 Acrylic resin partial dentures, as with complete dentures, are prone to fracture if dropped onto a hard surface whereas metal-based dentures are more resistant to this danger, but nonetheless can distort after being dropped or by mishandling during cleaning. This is most likely to occur with a mandibular denture20 with a lingual or cingulum bar major connector.21 As with complete dentures, cleaning partial dentures may be left to a carer with the possibility of neglect or damage.
As has been stated, for most individuals the simplest way to remove the denture biofilm is by mechanical cleaning with a toothbrush and a non-abrasive paste, at least once a day. As an adjunct to this, the denture can be soaked twice a week in 0.1% hypochlorite solution or chlorhexidine solution for 15–30 minutes.22 Long-term nocturnal use should be discouraged.23 According to Manfredi et al.22 leaving dentures to soak overnight is counter to 'hygienic logic' because organisms that inhabit the biofilm do not survive prolonged drying out. There is no evidence to support the view that leaving them to dry overnight will cause warpage of the acrylic.22
To summarise, both complete and partial dentures require careful removal of the denture biofilm. However this may not be carried out because:
-
The patient is unaware of the need to do this
-
The patient is unable to physically carry out the cleaning
-
The carer finds the process unpleasant and may do this perfunctorily or even avoid it
-
In the process of cleaning, the denture may be prone to fracture or distortion if mishandled.
The denture box
This is a simple device to hold the denture in place during cleaning (Fig. 5). It reduces the risk of fracture and distortion of a prosthesis. It will also allow a carer minimal handling of the denture and allow its storage with reduced risk of 'getting lost'. In an institution its 'footprint' will make positive discovery of the owner certain.

A denture box
One half of an orthodontic retainer or denture box (or a soap box) is filled with activated laboratory putty (Fig. 6). The occlusal surface of the denture is pressed into the putty sufficiently deeply to produce firm retention. The denture can be replaced in the negative impression and the surface rigorously cleaned with a brush. Where the patient has the loss of the use of a hand, the box can be steadied while brushing or it can be secured on its base with a suction pad or a fabric fastener.

Denture lightly impressed into the laboratory putty
The occlusal surface of the denture can be similarly displayed, following an imprint of the intaglio surface in the lid of the box if it has sufficient depth (Fig. 7).

Impression left by the denture
Case history 1
An 80+ male patient in indifferent health had suffered a recent stroke that prevented the normal use of his left hand. He was provided with an acrylic partial overlay denture, primarily to replace his upper front teeth. The denture was embedded in the silicone putty and he was able to steady the box with the left hand allowing the right hand to brush (Fig. 8).

The patient is able to steady the box with his left hand
Case History 2
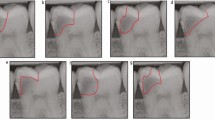
The patient has been provided with a resin-bonded bridge to replace the lower incisor teeth with wings on the canines (Fig. 9). Cingulum rests have been added to the canine wings to receive the cingulum bar major connector of the Kennedy Class 1 denture (Figs 10 and 11).

Resin bonded bridge with cingulum rests

Kennedy Class 1 denture with a cingulum bar major connector

Kennedy Class 1 denture replaced into the silicone impression to avoid accidental damage when cleaning
Case history 3
The cingulum bar connector does not impinge on the gingival margins but the abutment teeth, in the presence of plaque, are still prone to damage (Figs 12 and 13).

The disposition of plaque on the denture is shown with a disclosing solution

The fitting surface is impressed in the lid
Storage
The denture box provides a secure method of storage particularly in an institutional environment where it is not unusual for dentures to be wrapped in tissue and inadvertently discarded. In addition, where the denture is not marked for identification it possible for the ownership of a denture to be confused with others. The imprint of the denture being unique to the individual can be used to reclaim it to its owner. The imprint can be kept clean by washing under a tap and, if required, a small amount of chlorhexidine gluconate can be left in situ when stored.
References
NHS Information Centre. Adult dental health survey – first release. 2009, ammended 2010. Online information available at http://www.hscic.gov.uk/pubs/dentalsurveyfirstrelease09 (accessed November 2014).
Thomason J M J, Feine J, Exley C et al. Mandibular two implant-supported overdentures as the first choice standard of care for edentulous patients – the York Consensus Statement. Br Dent J. 2009; 207: 185–186.
Alani A, Bishop K, Renton T, Djemal S Update on guidelines for selecting appropriate patients to receive treatment with dental implants: priorities for the NHS – the position after 15 years. Br Dent J 2014; 217: 189–190.
Ellis J S, Levine A, Bedos C, Mojon P, Rosberger Z, Thomason J M . Refusal of implant supported mandibular overdentures by elderly patient. Gerodontology 2011; 28: 62–68.
Felton D, Cooper L, Duqum I et al. Evidence-based guidelines for the care and maintenance of complete dentures: a publication of the American College of Prosthodontists. J Prosthodont 2011; 20 (Suppl 1): S1–S12.
Watt D M, MacGregor A R . Designing complete dentures. 2nd ed. Bristol: Wright, 1986.
Coulthwaite L, Verran J . Potential pathogenic aspects of denture plaque. Br J Biomed Sci 2007; 64: 180–189.
Verran J . Malodour in denture wearers: an ill-defined problem. Oral Dis 2005; 11 (Suppl 1): 24–28.
Scully C, EI-Kabir M, Samaranayake LP . Candida and oral candidosis: a review. Crit Rev Oral Biol Med 1994; 5: 125–157.
Gendreau L, Loewy Z G Epidemiology and etiology of denture stomatitis. J Prosthodont 2011; 20: 251–260.
Chernosky M E . Collagen implant in management of perléche (angular cheilosis). J Am Acad Dermatol 1985; 12: 493–496.
Basker R M, Davenport J C . Prosthetic treatment of the edentulous patient. 4th ed. Oxford: Munksgaard, 2002.
de Souza R F, de Freitas O, Paranhos H, Lovato da Silva C H, Abu-Naba'a L, Gurgan C A . Interventions for cleaning dentures in adults. Cochrane Database Syst Rev 2009; 4: CD007395.
Azarpazhooh A, Leake J L . Systematic review of the association between respiratory diseases and oral health. J Periodontol 2006; 77: 1465–1482.
Sumi Y, Kagami H, Ohtsuka Y, Kakinoki Y, Haruguchi Y, Miyamoto H . High correlation between the bacterial species in denture plaque and pharyngeal microflora. Gerodontology 2003; 20: 84–87.
El-Solh A A . Association between pneumonia and oral care in nursing home residents. Lung 2011; 189: 173–180.
Wårdh I, Andersson L, Sörensen S . Staff attitudes to oral health care. A comparative study of registered nurses, nursing assistants and home care aides Gerodontology 1997; 14: 28–32.
Dharamsi S, Jivani K, Dean C, Wyatt C . Oral care for frail elders: knowledge attitudes, and practices of long term care staff. J Dent Educ 2009; 73: 581–588.
do Amaral B A, Barreto A O, Gomes Seabra E, Roncalli AG, da Fonte Porto Carreiro A, de Almeida EO . A clinical follow-up study of the periodontal conditions of RPD abutment and non-abutment teeth. J Oral Rehabil. 2010; 37: 545–552.
Pienkos T E, Morris W J, Gronet P M, Cameron S M, Looney S W . The strength of multiple major connector designs under simulated functional loading. J Pros Dent 2007; 97: 299–304.
Meeuwissen R, Keltjens H M, Battistuzzi P G . Cingulum bar as a major connector for mandibular removable partial dentures. J Pros Dent 1991; 66: 221–223.
Manfredi M, Polonelli L, Aguirre-Urizar J M, Carrozzo M, McCullough MJ . Urban legends series: oral candidosis. Oral Dis 2013; 19: 245–261.
Compagnoni M A, Souza R F, Marra J, Pero A C, Barbosa D B . Relationship between Candida and nocturnal denture wear: quantitative study. J Oral Rehab 2007; 34: 600–660.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article

Cite this article
Faigenblum, M. The denture box. An aid to denture hygiene. Br Dent J 218, 9–12 (2015). https://doi.org/10.1038/sj.bdj.2014.1139
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2014.1139
This article is cited by
-
An investigation into denture loss in hospitals in Kent, Surrey and Sussex
British Dental Journal (2017)
