
Key Points
-
Dental practices not currently using encapsulated amalgam systems may achieve a small reduction in mercury exposure by upgrading to them.
-
A further reduction of exposure to mercury may be achieved by upgrading the fabric of the workplace.
-
Systemic mercury poisoning is now very rare and so the continued routine monitoring of dentists and their staff is difficult to justify.
Abstract
Aims and objectives To review a long-standing mercury monitoring service offered to staff in dental practices in Scotland.
Methods During the first 20 years of the service, dentists and their staff were contacted by letter and invited to participate. Respondents were asked to collect samples of head hair, pubic hair, fingernail and toenail for analysis of mercury. After 1995, head hair samples were collected initially and further samples were only measured if head hair mercury was elevated.
Results At the start of this scheme many staff, including administrative staff, had systemic exposure to mercury (defined as increased mercury in all four samples). Incidents of exposure have decreased over the 35 years and are now very rare. Male staff were found to have higher mercury concentrations than female staff and dentists tended to have higher concentrations than other staff. Staff working in dental practices more than five years old had small but discernable increases in head hair mercury concentration. In recent years the use of reusable capsules such as Dentomats has been associated with a slight but statistically significant increase in head hair mercury concentrations when compared to the use of encapsulated amalgam systems. Staff wearing open-toed footwear had significantly higher toenail mercury concentrations compared to those who wore shoes.
Conclusions Exposure of staff to mercury in Scottish dental practices is currently now very low. This is probably as a result of increased awareness to the toxicity of mercury and improved methods of preparing amalgam. It may be possible to reduce exposure further, although probably only slightly, by upgrading practices and using encapsulated mercury amalgam.
Similar content being viewed by others


Introduction
Dentists and their staff work with significant quantities of mercury, the main constituent of amalgam, on a daily basis and cases of mercury poisoning in dentists have been reported.1,2 Mercury is lipid soluble and can enter the brain, from which it is only slowly eliminated. The symptoms of low level mercury poisoning are subtle such as headaches, fatigue, nausea, tremor, memory impairment and personality changes and so may be difficult to distinguish from other causes. A 1973 survey of dental staff in Scotland identified significant degrees of exposure to mercury3 and so a mercury monitoring service was introduced for staff in Scottish dental practices in order to identify those who may be at risk of exposure. Mercury was measured in samples of head hair, pubic hair, toenail and fingernail. These samples were used rather than urine and blood for reasons of analytical sensitivity, convenience, acceptability to staff, and the ability to assess an integrated exposure over a realistic time interval which in turn enabled sampling to be carried out infrequently. The aim was to inform dental staff of the extent of their exposure to mercury and, when it was considered excessive, to give support in achieving a reduction in exposure. Since 1975 this service has been available on a three- to six-year rolling basis. The accumulated data offers a unique opportunity to review a dental mercury monitoring scheme based on analysis of hair and nail. The preliminary findings from interrogating this database are presented.
Methods
Dentists were invited to participate by letter and if interested they and their staff sent samples for mercury analysis. Before 1995, samples of head hair, pubic hair, fingernail and toenail were collected. Mercury avidly binds to hair and nails as a result of systemic incorporation as well as direct surface contamination. Systemic mercury exposure was defined as mercury levels above 2 μg/g in all four samples (concentrations are normally less than 0.5 μg/g). External contamination was considered to be the likely cause when mercury concentrations were raised in hair and/or fingernails alone. After 1995 head hair mercury was measured and if results were above 2 μg/g then further samples of pubic hair, fingernail and toenail were requested and staff were asked about their consumption of predatory fish.
In the 1970s and 1980s invitation to participate was limited to a small, but now unknown, number of practices. Since the early 1990s, all dental practices throughout Scotland were invited to participate. Participation is voluntary, however, since 2005 dental staff have been strongly encouraged to participate to ensure compliance with COSHH (Control of Substances Hazardous to Health) regulations. This has resulted in a substantial increase in response rate with replies being received from 681 practices of a total of 886 (75%) and the percentage of staff returning samples around 75%.
The category of staff (dentist, dental nurse, receptionist, manager, hygienist, technician or cleaner) was recorded; insufficient information was available on therapists. Additional information was obtained at different times: use of open-toed footwear from 1977 to 1987; system used for preparation of amalgam from 1977 to 1982, 1985 to 1987, 2004 to 2007; age of dental practice from 2004 to 2009.
Mercury was measured by neutron activation analysis until 1982 and after this time by cold vapour atomic absorption spectrometry. Certified reference materials were used to confirm analytical concordance between the two methods. Participation in the 'Mercury in Hair' Interlaboratory Comparison Program external quality assurance scheme4 was satisfactory. No attempt was made to cleanse surface mercury from hair or nails, partly because its avid binding to sulphur bonds make cleaning procedures ineffective5 and partly because information on contamination of samples was considered to be useful.
Mercury concentrations were positively skewed and so medians and 75th and 95th percentiles are reported. Statistical analysis is by the Mann-Whitney test.
Results
Changes of mercury concentrations with time
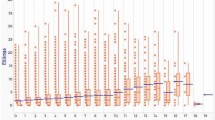
The change of head hair, pubic hair, fingernail and toenail mercury concentrations with time is shown in Figures 1a to 1d. In the early years of the service mercury concentrations were high, often considerably so, in all four samples. Mercury concentrations in all four sample types have substantially decreased over 35 years. Head hair mercury is now close to concentrations found in the general population.

Head hair mercury concentrations during thirty-five years expressed as medians, 75th & 95th percentiles

Pubic hair mercury concentrations during thirty-five years expressed as medians, 75th & 95th percentiles

Fingernail mercury concentrations during thirty-five years expressed as medians, 75th & 95th percentiles

Toenail mercury concentrations during thirty-five years expressed as medians, 75th & 95th percentiles
Incidence of mercury exposure and contamination
Tables 1 and 2 show the incidence of systemic exposure and contamination in five-year blocks of time. Table 1 records this data up to and including 1994 when mercury screening of head hair, pubic hair, toenail and fingernail was routinely performed, while Table 2 shows the data after this time when an initial head hair screen was performed and samples for further analyses were only requested when head hair mercury was ≥2.0 μg/g. The staff who were exposed to mercury were mainly dentists and dental nurses (89% and 5% respectively) although exposure has also occurred in staff members who would not be expected to work directly with mercury: receptionist, hygienist, manager and cleaner (3%, 0.7%, 0.4% and 0.4% respectively). The frequency of exposure incidents has progressively reduced over the thirty-five years with no incidents over the last five years. Similarly, the frequency of head hair and fingernail contamination incidents has fallen. On occasions raised pubic hair and/or toenail concentrations were found without increases in head hair and/or fingernail concentrations. This explanation of these results is less obvious and so they are recorded separately in the last three columns of Table 1 and the last two columns of Table 2.
The relationship of gender with mercury concentrations
With the exception of dentists, most of the staff employed in dental surgeries are female and so this was the only occupational group in which there were sufficient numbers to make reliable gender comparisons. The results in Table 3 and Figures 2a to 2d show that male dentists consistently have higher mercury concentrations.

Head hair mercury concentrations

Pubic hair mercury concentrations

Fingernail mercury concentrations

Toenail mercury concentrations
The relationship of occupation with mercury concentrations
The mercury concentrations in different occupational categories are recorded in Table 4. Data were taken only from female staff because of the observed difference of mercury concentrations between male and female dentists and because of the low number of results from male staff other than dentists. Similarly there were no significant differences in results from hygienists and administrative staff (receptionists, managers and secretaries) and so these groups, in which no direct exposure to mercury was expected, were also combined. Results are shown in Table 4 and Figures 2a to 2d.
In the first decade of the new millennium, head hair samples were collected from 209 female cleaners who were employed by dental practices. None had high head hair concentrations and so no pubic hair, fingernail or toenail samples were collected. The median head hair mercury concentration was 0.3 μg/g (inter-quartile range = 0.1 to 0.5 μg/g) which was significantly lower compared to dentists, dental nurses and hygienists / administrative staff (p <0.001 for all three groups).
The effect of age of dental practices on mercury concentrations
From 2005 until 2009 the concentrations of head hair mercury in staff working in dental practices were initially grouped into five-year blocks of time. The mean head hair mercury concentrations in staff who worked in dental practices which were five years old or less were lower than all other groups. For this reason five years was used as an appropriate cut-off point at which more detailed statistical analyses were carried out. Four occupational categories were studied and the results in Table 5 show that dentists (both male and female) and dental nurses working in dental practices more than five years old had significantly higher head hair mercury concentrations than those working in practices up to five years old. Hygienists and administrative staff working in practices more than ten years old also had higher head hair mercury concentrations but this did not reach statistical significance (p = 0.06).
The effect of wearing open-toed shoes on mercury concentrations
The effect of wearing open-toed footwear on mercury concentrations was studied in two groups: male dentists and female dentists and female dental nurses combined; the latter occupations were merged into a single group since there was no significant difference in their mercury concentrations in each of the sample types. In both groups, there was no difference in mercury concentrations in head hair, pubic hair or fingernail samples, however, toenail concentrations were significantly raised in those staff who wore open-toed footwear (Table 6).
The effect of preparation of amalgam on mercury concentrations
From 2004 to 2009, staff were asked to indicate whether reusable capsules (eg Dentomat) or an encapsulated system was used when preparing amalgam. The effect of the instrument used on head hair mercury concentrations is recorded in Table 7. Lower head hair mercury concentrations were found in groups using encapsulated mercury preparation systems. Encapsulated systems are used more commonly than reusable capsules and in the course of the five-year period studied the use of encapsulated systems has increased from 77% to 90%.
Discussion
Elemental mercury is a powerful toxin and inhalation of sufficient mercury vapour can be fatal.6,7 Chronic exposure to lower concentrations of mercury can result in milder symptoms as well as detectable effects on motor function and behaviour, and previous studies have shown that relatively low levels of mercury exposure may be detrimental to health.8,9 However, it is difficult to designate a threshold of exposure below which can be considered to be safe. For this reason and because local cases of symptomatic mercury poisoning of dentists had been detected, an occupational mercury monitoring programme was introduced in 1975 for dental practices in Scotland.
During the 1970s median mercury concentrations in all samples collected (head hair, pubic hair, fingernail and toenail) were markedly higher than in recent years. In a significant minority of staff, concentrations were markedly high; for example, the 95th percentiles for dental staff were head hair mercury 21.3 μg/g, pubic hair 8.5 μg/g, fingernail 242 μg/g and toenail 16.3 μg/g (cf <0.5 μg/g concentrations in unexposed individuals). Over the 35 years of the service head hair mercury concentrations have fallen substantially from a median in all staff of 8.6 μg/g and 90th percentile value of 11.6 μg/g in the first five years to a median of 0.5 μg/g and 90th percentile value of 1.2 μg/g in the final five years. This is close to reference values of 0.3 μg/g and 90th percentile value of 1.4 μg/g quoted by the US Environmental Protection Agency.10
There has also been a substantial fall in both the incidence and severity of mercury exposure. This was defined as elevated mercury concentrations in head hair, fingernail, toenail and pubic hair mercury samples to 2 μg/g or more. Until the 1990s the frequency of mercury exposure was 15% to 20% with the vast majority of cases affecting dentists. However, exposure also occurred occasionally in hygienists, cleaners and administrative staff. Mercury exposure is now very unusual with only one case having been detected in the last decade. The increases in hair and nail mercury concentrations in this case were minor compared to typical cases of exposure found in the 1970s and 1980s.
The finding of high head hair and/or fingernail concentrations with normal concentrations of pubic hair and toenail mercury, were considered to be due to external contamination. The finding of isolated high fingernail mercury concentrations was postulated to be due to manual handling of liquid mercury during the preparation of amalgam and the very high mercury concentrations often found in fingernail samples supports this notion. The sharp drop of fingernail mercury concentrations from the 1980s to the 1990s may be the result of the widespread use of gloves. It was thought that isolated contamination of head hair was probably caused by spray during drilling of amalgams. Transfer of mercury to hair from contaminated fingers was thought to be an additional explanation when hair head and fingernail mercury concentrations were both increased. This form of contamination has reduced around 30-fold during the existence of this service. On occasions high results of unexpected sample combinations were found, eg head hair/pubic hair, or fingernail/pubic hair/head hair, or isolated high pubic hair or toenail results. It is difficult to explain all permutations but it is possible that direct transfer from finger to pubic hair, head hair and/or toenail may occur, for example, during a bathroom visit or in the process of collecting samples.
The main reason for the decrease of mercury concentrations, exposure and contamination over the 35 years is likely to be an increased awareness of the dangers of mercury and the consequent introduction of safer ways of preparing amalgam. There has also probably been increasing awareness that mercury is toxic and that its toxicity is as a result of inhalation of mercury vapour.
Male dentists were found to have higher concentrations of mercury throughout the 35 years compared to female dentists. This was found in all sample types studied and in all time periods studied up until the 2000s during which time a significant difference was only found for head hair samples. This difference was slight, by 0.1 μg/g, and was probably detected because of the large head hair sample studied (over 3,000). Failure to detect statistical significance for pubic hair, fingernail, and toenail mercury concentrations may be related to the relatively low numbers of samples collected (100 to 200). This gender difference has been documented in previous surveys,11,12 in which urine samples were predominantly monitored. A gender-based variation in the renal handling of mercury was proposed as a possible explanation, however, the samples collected in the present survey were of hair and nail making this explanation unlikely.
Four groups of female staff working in different professions within dental practices were compared in more detail and certain trends and associations were found. In the 1970s, hygienists and administrative staff had similar hair and nail concentrations to dentists and dental nurses suggesting that there may have been less stringent delineations of working responsibilities, for example reception staff covering dental nurse duties. In the 1990s and 2000s female dentists had higher head hair, pubic hair and toenail mercury concentrations than dental nurses. Fingernail concentrations, however, were similar in both groups.
From 2005, practices were actively encouraged to include cleaners in the mercury monitoring scheme because of a concern that in the process of sweeping or particularly of vacuum cleaning, they may disturb any mercury at floor level and then breathe in mercury vapour. Since cleaners often work after the other staff have left the practice, it was thought that this particular exposure would only affect them. Their mercury values were, however, found to be significantly lower when compared to other staff groups, suggesting that this concern was unfounded. However, it is of note that cleaners had significantly lower mercury concentrations than hygienists and administrative staff who, in recent years, are unlikely to work directly with mercury. This affected all sample types signifying a small but discernible mercury exposure of staff who do not work directly with it and which is presumably related to the total time spent in dental practices.
It is reasonable to speculate that current mercury exposure may be greater in older dental practices which are likely to have suffered more spillages and processed larger volumes of liquid mercury over the years. To investigate this possibility further, the age of dental practices was requested during the second half of the 2000s and head hair mercury concentrations in new practices were compared to those in older ones. For male and female dentists and dental nurses higher mercury concentrations were found in those staff working in practices more than five years old. The differences in median head hair mercury concentrations found, although statistically significant, were relatively small (0.1 to 0.2 μg/g). However, this may well be an underestimate since many older practices may have been renovated thus reducing potential exposure to mercury. Wooden flooring, for example, tends to harbour more spilled mercury than smooth flooring, which is easier to clean. This association was less obvious in staff who do not work directly with mercury (hygienists and administrative staff). These staff would be expected to spend most of their time in offices away from clinics where amalgam is prepared and so be less exposed to mercury.
In the early years of this survey relatively primitive systems such as mortar and pestle, de Trey vibrators, and squeezing of excess mercury through cloth were commonly used in the preparation of amalgam. The Dentomat, an electrical mixing device, was initially introduced in the 1970s and was in widespread use. However, this and similar mixers still involve the use of liquid mercury and its potential volatilisation into the atmosphere. It is likely that such mercury losses may have increased during the lifetime of the instrument because of infrequent or non-existent servicing as is recommended by the manufacturers. Encapsulated systems began to replace Dentomats in the 1980s and have slowly been superseding them since then. From 2005 until 2009 dental staff were asked which type of system for producing amalgam was used. In all three groups of staff investigated (male dentists, female dentists and female nurses) those who used encapsulated systems had slightly but significantly lower head hair concentrations. The use of Dentomats is being slowly phased out with their use decreasing from 23% to 10% from 2004 to 2009.
During the 1980s and 1990s the effect of wearing open-toed footwear on mercury concentrations was investigated. Those staff who wore open-toed footwear had higher toenail mercury concentrations than those whose footwear covered the toes. Mercury concentrations in head hair, pubic hair and fingernails did not differ between the two groups. This finding suggests direct contamination of toenails from air mercury, which is more concentrated at floor level.
The results of this review give an interesting account of mercury exposure in Scottish dental practices over the past 35 years. With improved methods of amalgam preparation and as a probable result of increased awareness of the dangers of mercury, exposure has declined dramatically. There is evidence that by replacing Dentomats still in current use with encapsulated systems and by upgrading or renewing of dental practices, exposure to mercury may be further decreased albeit marginally. It is hoped that further useful information may be obtained by a retrospective survey of appropriate clinical and physiological markers of mercury toxicity in selected high- and low-risk dentists identified in the early years of this service.
References
Ship I I, Shapiro I M . Mercury poisoning in dental practice. Compend Contin Educ Dent 1983; 4: 107–110.
Symington I S, Cross J D, Dale I M, Lenihan J M . Mercury poisoning in dentists. J Soc Occup Med 1980; 30: 37–39.
Lenihan J M, Smith H, Harvey W . Mercury hazards in dental practice. Assessment and control by activation analysis. Br Dent J 1973; 135: 365–369.
The 'Mercury in Hair' Interlaboratory Comparison Program, Environmental Health Research Division, Health Canada, Ontario K1A 0K9.
Suzuki T. Preparation of samples for mercury analysis. In Clarkson T W, Friburg L, Nordberg G F, Sager P R (eds) Biological monitoring of toxic metals. pp 623–640. New York: Plenum Press, 1998.
Rowens B, Guerro-Betancourt D, Gottlieb C A, Boyes R J, Eichenhorn S . Respiratory failure and death following acute inhalation of mercury vapor. Chest 1991; 99: 185–190.
Emsley J. The elements of murder. Oxford: Oxford University Press, 2005.
Ritchie K A, Gilmour W H, Macdonald E B et al. Health and neuropsychological functioning of dentists exposed to mercury. Occup Environment Med 2002; 59: 287–293.
Echeverria D, Aposhian H V, Woods J S et al. Neurobehavioral effects from exposure to dental amalgam Hg(o): new distinctions between recent exposure and Hg body burden. FASEB J 1998; 12: 971–980.
Anon. Blood and hair mercury levels in young children and women of child-bearing age – US 1999. Morbidity and Mortality Weekly Report 2001; 50: 140–143. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5008a2.htm.
Jokstad A. Mercury excretion and occupational exposure of dental personnel. Comm Dent Oral Epidemiol 1990; 18: 143–148.
Martin M D, Naleway C, Chou H N . Factors contributing to mercury exposure in dentists. J Am Dent Assoc 1995; 126: 1502–1511.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Duncan, A., O'Reilly, D., McDonald, E. et al. Thirty-five year review of a mercury monitoring service for Scottish dental practices. Br Dent J 210, E2 (2011). https://doi.org/10.1038/sj.bdj.2011.49
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.2011.49
