
Abstract
Study design:
Prospective cross-sectional study.
Objective:
To study epidemiology, complication, neurological and functional outcome in non-traumatic spinal cord lesions (NTSCL) after inpatient rehabilitation.
Setting:
Neurological rehabilitation unit of a tertiary research hospital.
Methods:
Sixty-four patients (M/F=28:36) with NTSCL admitted from June 2005 to January 2008 for multidisciplinary rehabilitation. Epidemiology, medical complications during stay in rehabilitation, admission and discharge—Barthel Index (BI) and American Spinal Injury Association (ASIA) impairment scale for functional and neurological recovery, respectively, were recorded and analyzed.
Results:
NTSCL constituted 60% (64 of 106) of the total SCL patients admitted for rehabilitation during the same period. Female patients outnumbered males (56.25%) in the study. Mean age, duration of illness and duration of stay in rehabilitation were 30.64±13.67 years (6–57), 7.09±9.15 months (1–48) and 55.75±40.91 days (14–193), respectively. The ratio of paraplegia and quadriplegia was 2:1. Forty-four patients (68.75%) had incomplete cord lesion according to the ASIA impairment scale. Spinal tumors (26.6%) were found to be the most common etiology, followed by Pott's spine (25%) and transverse myelitis (22%). Urinary tract infection was found to be the most common complication (50%), followed by spasticity (35.93%) and urinary incontinence (31.25%). The mean BI scores showed significant (P=0.000) functional recovery during rehabilitation using paired Student's t-test. The ASIA impairment scale showed significant neurological recovery (P=0.001) using the Wilcoxon non-parametric test.
Conclusions:
NTSCL constitute a significant proportion of overall SCL. Female population, paraplegia and incomplete cord lesions are more common among NTSCL in this study. Patients with NTSCL recover significantly both neurologically and functionally with rehabilitation intervention.
Similar content being viewed by others


Introduction
Non-traumatic spinal cord lesions (NTSCL) represent a significant proportion of individuals with SCL admitted in rehabilitation settings, and it is important to further evaluate their demographics, neurological presentation and functional outcome.1 A plethora of literature is available on the medical complications as well as on the neurological and functional outcome of traumatic SCL, but very few studies have focused on medical complications,2, 3 etiology4, 5, 6, 7 and neurological8, 9 and functional1 outcomes after NTSCL.
The incidence of NTSCL is difficult to determine because of the infrequent reporting, but it is estimated to be approximately equal to that of traumatic SCI.10 Spinal tumors7 and Pott's spine5, 6 have been reported as the most common etiology of NTSCL in different studies.
Although most of the studies have reported more men suffering from NTSCL compared with women, a reverse trend has also been noticed.3
Urinary tract infection (UTI), pain (naturopathic as well as musculoskeletal), pressure ulcers, spasticity, depression, heterotrophic ossification and deep vein thrombosis are among the more common complications noticed in patients suffering from NTSCL during rehabilitation. There are few studies1, 2 that suggest UTI as the most common complication faced during in-patient rehabilitation.
Irrespective of the etiology, severity and extent of insult to the cord, patients with spinal cord lesions perform better in activities of daily living, including self-care, personal toilet, transfer and locomotion by whatever means, in a much better way after rehabilitation intervention and show significant neurological recovery.8, 9 Mckinley et al.1 have reported significant functional recovery in patients with NTSCL after rehabilitation intervention.
This prospective study was conducted to observe the etiology, medical complications, neurological and functional recovery in patients with NTSCL admitted in our rehabilitation setup.
Patients and methods
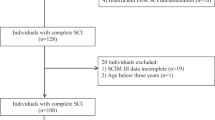
This prospective study consisted of 64 patients with NTSCL admitted in neurological rehabilition unit over a period of 32 months (June 2005–January 2008). During this period, overall 106 patients with spinal cord lesions (both traumatic and non-traumatic) were admitted for in-patient rehabilitation. Patients who were medically stable and able to participate actively for at least 2 hrs per day in the rehabilitation were included in the study. Patients with cardiorespiratory co-morbidities, requiring ventilator for assisted respiration, and with unstable vertebral injuries were excluded.
The demographic profile of the patients included age, gender, family size and age at the onset of lesion. Duration of illness (in months), duration of stay in the rehabilitation unit, and level and completeness of lesion were recorded. Etiology of NTSCL, requirement of assistive devices/orthoses for mobility and locomotion, and medical complications during in-patient rehabilitation were also recorded.
Neurological recovery of all patients was recorded at-admission using the American Spinal Injury Association (ASIA) impairment scale.11 It was compared with at-discharge ASIA impairment scale to assess neurological recovery during the stay in rehabilitation. Functional recovery in all the patients was measured using the Barthel Index (BI) score.12 Admission and discharge scores were compared to assess functional recovery during rehabilitation.
Data analysis
SPSS 15.0 was used for the analysis of the data. Descriptive statistics included frequency, means and standard deviation for quantitative variables such as age, duration of illness, family size, duration of stay and requirement of assistive devices and orthoses. Paired Student's t-test was used for the assessment of functional recovery using mean BI scores at admission and at discharge. The Wilcoxon non-parametric test was used for the assessment of neurological recovery by comparing admission and discharge ASIA scale scores.
Results
Sixty-four patients with NTSCL who underwent in-patient rehabilitation were included in the study. During the same period, a total of 106 patients with SCL were admitted in the unit for in-patient rehabilitation, and so the incidence of NTSCL was more (60%) than the traumatic spinal cord lesions (TSCL). Of 64 patients, 28 were men and 36 women. The age of the patients varied from 6 to 57 years (30.64±13.67). Duration of stay in the rehabilitation unit ranged between 14 and 193 days (55.75±40.91) and the duration of neurological illness varied between 1 and 48 months (7.09±9.15). Maximum number of patients was from the second and fifth decades of life (16 each), but there was no specific age group suggestive of a high incidence of NTSCL.
The etiology of NTSCL is given in Table 1. Twenty-one patients (32.8%) had cervical lesion with a clinical picture of quadriplegia and 43 patients (67.2%) had dorsal or lumbar lesion with paraplegia. The ratio of paraplegia and quadriplegia was 2:1. Among the paraplegia patients, 95.34% (41 of 43) had dorsal lesion (6 patients had the highest level of lesion between D1 and D6 and 35 patients had the highest level of lesion between D7 and D12) and only 2 patients (4.66%) had lumbar lesions.
Fourteen patients (21.9%) needed lower limb orthoses for locomotion, 9 patients (14.1%) required wheelchairs for mobility and locomotion, 6 patients (9.4%) used walkers for locomotion, 2 patients (3.1%) needed auxiliary crutches, 5 patients (7.8%) needed tripod canes and 10 patients (15.6%) required both orthoses and walkers for locomotion in the study.
Fifty-eight patients (90%) reported at least one complication during their stay the in rehabilitation unit. The frequency of common medical complications is shown in Table 2.
Neurological recovery was assessed using the ASIA impairment scale. Assessment was done both at admission and at discharge. At admission, 31.25% patients (20 of 64) had complete cord lesion (ASIA-A) according to the scale, 20.31% patients (13 of 64) had complete motor cord lesion (ASIA-B) and 48.43% patients (31 of 48) had incomplete cord lesion (ASIA-C and D). At discharge, only 18.75% patients (12 of 64) had complete cord lesion (ASIA-A), 7.81% patients (5 of 64) had complete motor lesion (ASIA-B) and 73.43% patients (47/64) had incomplete cord lesion (ASIA-C and D). Significant neurological recovery was noted during the period of rehabilitation (P=0.001).
Functional recovery was assessed using the BI scores. At discharge, mean BI scores were compared with mean admission scores and analyzed. At admission, BI scores varied from 0 to 75 with a mean of 31.25±18.55, and at discharge, BI scores varied from 0 to 100 with a mean of 55.46±23.71. Significant functional recovery was observed (P=0.000) in patients during in-patient rehabilitation.
Discussion
The demographic characteristics of this study were in accordance with the earlier studies performed on NTSCL.1, 3, 7 In this study, patients with NTSCL had a more even gender distribution with women outnumbered men (36 of 64) as compared to the results with TSCL where almost all studies13, 14 have found male preponderance with most common age group ranging between 16 and 30 years.14 Similar findings with male predominance among TSCL were also found in our earlier study.15 However, in contrast with these studies,1, 3 no age-related trend was found in the present study, and the patients were distributed equally in all age groups. This could be attributed to the fact that in these studies most of the patients with spinal tumors, which was the most common etiology, had secondary tumors, which is a late decade phenomenon. In our study, all patients barring none had primary spinal tumors, which may occur at very early age.
More than two-third of the patients in the study (68.75%—44 of 64) had incomplete cord lesion, and this trend was noticed both in quadriplegia (62%—13 of 21) and in paraplegia (72%—31 of 43). The injuries were found to be less severe (incomplete). The ratio of paraplegia and quadriplegia was found to be 2:1. The severity and completeness of the injury, as well as the clinical pattern of cord lesions observed in the study, were similar to some earlier studies.1, 3 This may be due to a combination of factors, such as the region of the spinal cord involved in NTSCL and the often insidious nature of the lesion. The specific pattern of the lesions seen at individual centers could influence the severity of the NTSCL seen.3 Considering the etiology of the spinal cord lesions, most of NTSCL have the propensity to develop in the dorsal or dorsolumbar region, except the ossification/fluorosis of the posterior longitudinal ligament which is reported to be more common in the cervical region.
The most common etiology in this study was spinal tumors. Some earlier studies have also reported tumors as the most common etiology in their series.1, 3 But as compared to these studies, the present study has all primary tumors. All spinal tumors were already operated and then taken over by the rehabilitation unit for further rehabilitation. These cases showed both neurological and functional recovery during their stay in rehabilitation. However, as this is a cross-sectional study, conclusions cannot be drawn on the long-term outcome in these cases. Some studies performed in the same region5, 6 have reported Pott's spine as the most common etiology of NTSCL in their series. In our study also it was the second most common cause of NTSCL.
More than 76% of patients (16/21) with quadriplegia required assistive devices, orthoses or both as a means of mobility, transfers and locomotion. Among paraplegics, 53.48% of patients (23/43) needed them for mobility, transfers and locomotion. Fourteen patients (21.9%) required lower limb orthoses for locomotion, 6 patients (9.4%) required walkers and an additional 10 patients (15.6%) used both for locomotion. Nine patients (14.1%) used wheelchairs for transportation and mobility. In an earlier study, wheelchairs were rated significantly higher than long leg braces on value, potency and activity and transportation. It was also observed that wheelchair users had complete cord lesions and were older, whereas orthoses users had incomplete injury and were younger.16 As the present study is not a follow-up study, it is impossible to comment on the future use of orthoses or wheelchairs after discharge from the rehabilitation unit.
Mortality and morbidity after TSCL are higher in people with higher age at injury.17 But Nair et al.2 in their study on NTSCL, did not observe significant correlation between age and frequency of medical complications during the rehabilitation phase. In the present study, 90.62% of patients (58/64) had at least one medical complication during in-patient rehabilitation. Similar frequency was noted by Nair et al.2 in their series with NTSCL patients. However, New et al. observed a lower incidence (63.2%) of medical complications in their series.3 UTI was found in 50% of patients (32/64) and was the most common medical complication in the present study. All NTSCL patients are taken on clean intermittent catheterization/self-catheterization soon after admission in the rehabilitation unit after getting a urine culture sample. Prophylactic antibiotic was not given routinely to the patients and only symptomatic UTIs (with fever) were treated with antibiotics. Abdominal ultrasound were urodynamic studies performed in all patients with spinal cord lesion admitted in the rehabilitation unit. Despite all these protocols, the reasons for this high UTI could be poor compliance in relation to timed voiding, poor hygiene with CIC, indwelling catheter for prolonged period (before coming to the rehabilitation ward) and neurogenic bladder with irritative or obstructive urinary symptoms.
Spasticity was the second most common complication with 35.93% (23 of 64), urinary incontinence in 31.25% (20 of 64) and pressure ulcers in 25% of patients (16/64). Nair et al. reported genitor-urinary complications in 70% of the participants in their series, with 60% of patients having at least one episode of UTI. Present study showed similar frequency of UTI (64–80%) among patients with SCL. Similar frequency of UTI has been noted in different rehabilitation settings within the National Health Service in United Kingdom.18 Some other studies3, 19 on NTSCL have reported lower frequency of UTI. The reason behind this low frequency could be; because of different etiology of the cord lesion, bladder management technique, usage of antibiotics and infection control protocols.2 In NTSCL, the frequency of spasticity ranged from 14.9 to 56%.2, 3, 19 In the present study, spasticity was found to be present in 35.93% of patients. Maynard et al.20 reported 32.2% of patients with TSCL developed spasticity before discharge from hospital. So our study showed a similar trend, although with NTSCL. In this study, the frequency of pressure ulcers was 25% (16 of 64), which is similar to earlier studies2, 3, 19 with NTSCL. As ulcers take long time to heal, strategies of prevention and treatment should be an integral part of the protocol for rehabilitation of subjects with NTSCL. Fifteen patients in the study had constipation during rehabilitation. It could be because of immobility, changes in colonic compliance, prolonged transit time, fecal impaction, poor fluid intake and low fiber content in the diet. A regular bowel program with adequate fluid and fiber intake may help in preventing constipation.2
Neurological recovery is an important aspect of rehabilitation of patients with NTSCL. Significant neurological recovery was noted in this study during the period of rehabilitation (P=0.001), as most of the patients improved by at least one grade according to the ASIA impairment scale at the time of discharge. Eight patients, who were ASIA-A at admission, showed recovery by at least one grade by the time of discharge. The reason could be that the patients were in spinal shock at admission or that their infection (in cases of Pott's spine and transverse myelitis) subsided with treatment during stay in rehabilitation and they showed neurological recovery. Catz et al. in their study,8 observed complete or substantial neurological recovery (Frankel Grade D or E) in patients with NTSCL in rehabilitation with 51% of patients with Grade A, B or C on admission were improved to Grade D by the time of discharge. According to the authors, neurological recovery in NTSCL during rehabilitation was significantly affected by initial Frankel grade and etiology, and recovery is usually better in NTSCLs than in TSCLs. Ronen et al.9 in their study with spinal stenosis patients, reported significant neurological recovery in 58% of cases after inpatient rehabilitation. Providing an optimum environment for spontaneous recovery, preventing/managing secondary complications as well as medication or other treatment modality as per the etiology of the lesion and proper physiotherapy are some of the contributory factors in the neurological recovery of patients with NTSCL.
Functional recovery was assessed by comparing the mean BI score at-admission with at-discharge scores. Significant functional recovery was observed in the study (P=0.000) during the period of rehabilitation. Several studies1, 3, 15, 19 have shown similar significant functional recovery among patients with NTSCL, underlying the important role of rehabilitation in making these patients independent for their activities of daily living, mobility and locomotion.
Conclusion
This study gives further information about change in the demographic profile in NTSCL patients compared with TSCL patients in the form of less gender difference in the former. No trend toward any specific age group was noted in the study in contrast to some earlier studies. The study is suggestive of the fact that patients with NTSCL tend to have less-severe, incomplete injury and more paraplegics when compared with TSCL. Adequate provision of assistive devices/orthoses contributes favorably in making these patients independent/less dependent for transportation and locomotion. Further, rehabilitation has an indispensable role to play in favorable functional outcome and prevention/management of medical complication after NTSCL.
Limitations of the study
There are limitations of this study, the foremost being the small sample size, although with the same it is corroborating the findings of the earlier studies performed in this center as well as across the world. There is a selection bias in the study, as only the patients who were medically stable and in a position to participate in the rehabilitation program were admitted in the unit/included in the study. The higher percentage of NTSCL cases could also be attributed to the fact that some operated/conservatively managed TSCL cases were directly discharged from the neurosurgery unit because of the non-availability of beds in the rehabilitation unit.
References
McKinley WO, Seel RT, Hardman JT . Nontraumatic spinal cord Injury: incidence, epidemiology and functional outcome. Arch Phys Med Rehabil 1999; 80: 619–623.
Nair KPS, Taly AB, Maheshwarappa BM, Kumar J, Murali T, Rao S . Nontraumatic spinal cord lesions: a prospective study of medical complications during in-patient rehabilitation. Spinal Cord 2005; 43: 558–564.
New PW, Rawicki HB, Bailey MJ . Nontraumatic spinal cord injury: demographic characteristics and complications. Arch Phys Med Rehabil 2002; 83: 996–1001.
Akyuz M, Dalyan M, Keykubatli AO, Kaya A, Cakci A . A retrospective study of non-traumatic spinal cord injury. Eur J Phys Med Rehabil 1999; 8: 163–165.
Chaurasia RN, Verma A, Joshi D, Mishra S . Etiological spectrum on non-traumatic myelopathies: Experience from a tertiary care centre. J Assoc Physicians India 2006; 54: 445–448.
Srivastava S, Sanghavi NG . Non traumatic paraparesis: etiological, clinical and radiological profile. J Assoc Physicians India 2000; 48: 988–990.
Moore AP, Blumhardt LD . A prospective survey of the causes of non-traumatic spastic paraparesis and tetraparesis in 585 patients. Spinal Cord 1997; 35: 361–367.
Catz A, Goldin D, Fishel B, Ronen J, Bluvshtein V, Gelernter I . Recovery of neurologic function following nontraumatic spinal cord lesions in Israel. Spine 2004; 29: 2278–2282.
Ronen J, Golden D, Itzkovich M, Bluvshtein V, Gelernter I, Livshitz A et al. Outcomes in patients admitted for rehabilitation with spinal cord or cauda equine lesions following degenerative spinal stenosis. Disabil Rehabil 2005; 27: 884–889.
Parsons KC, Lammertse D . Rehabilitation in spinal cord disorders: epidemiology, prevention and system of care of spinal disorders. Arch Phys Med Rehabil 1991; 72 (Suppl 1): S293–S294.
Ditunno Jr JF, Young W, Donovan WH, Creasey G . The international standards booklet for neurological and functional classification of spinal cord injury. Paraplegia 1994; 32: 70–80.
Mahoney FI, Barthel D . Functional evaluation: the Barthel Index. MD State Med J 1965; 14: 56–61.
McKinley WO, Huang M, Tewksbury MA . Neoplastic vs traumatic spinal cord lesion: an inpatient rehabilitation comparison. Am J Phys Med Rehabil 2000; 79: 138–144.
Go BK, DeVivo MJ, Rechards JS . The epidemiology of spinal cord lesion. In: Stover SL, Delisa JA, Whiteneck GG (eds). Spinal Cord Lesion. Aspen: Gaithersburg, MD, 1995, pp 21–25.
Gupta A, Taly AB, Srivastava A, Vishal S, Murali T . Traumatic vs non-traumatic spinal cord lesion: comparison of neurological and functional outcome after inpatient rehabilitation. Spinal Cord 2008; 7: 482–487.
Heinemann AW, Magiera-Planey R, Schiro-Geist C, Gimines G . Mobility for person with spinal cord injury: an evaluation of two systems. Arch Phys Med Rehabil 1987; 68: 90–93.
Whiteneck GG, Charlifue SW, Frankel HL, Fraser MH, Gardner BP, Gerhart KA et al. Mortality, morbidity and psychosocial outcomes of persons spinal cord injured more than 20 years ago. Paraplegia 1992; 30: 617–630.
Smith M . Efficacy of specialist versus non-specialist management of spinal cord injury within the UK. Spinal Cord 2002; 40: 11–16.
McKinley WO, Tewksbury MA, Godbout CJ . Comparison of medical complications following nontraumatic and traumatic spinal cord injury. J Spinal Cord Med 2002; 25: 88–93.
Maynard FM, Karunas RS, Adkins RH, Richards JS, Waring III WP . Management of neuromusculoskeletal systems. In: Stover SL, DeLisa JA. Whiteneck GG (eds). Spinal Cord Injury: Clinical Outcomes from the Model Systems. Aspen Publishers: MD, 1995, pp 145–169.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gupta, A., Taly, A., Srivastava, A. et al. Non-traumatic spinal cord lesions: epidemiology, complications, neurological and functional outcome of rehabilitation. Spinal Cord 47, 307–311 (2009). https://doi.org/10.1038/sc.2008.123
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2008.123
Keywords
This article is cited by
-
Reliability and validity of the international standards for neurological classification of spinal cord injury in patients with non-traumatic spinal cord lesions
Spinal Cord (2022)
-
Impact of complications at admission to rehabilitation on the functional status of patients with spinal cord lesion
Spinal Cord (2020)
-
Clinical features and inpatient rehabilitation outcomes of infection-related myelopathy
Spinal Cord (2017)
-
Factors predictive of survival and estimated years of life lost in the decade following nontraumatic and traumatic spinal cord injury
Spinal Cord (2017)
-
Neurological and functional recovery in acute transverse myelitis patients with inpatient rehabilitation and magnetic resonance imaging correlates
Spinal Cord (2016)
