
Abstract
To examine the association between stage 1 hypertension (at baseline and longitudinal change) defined by the 2017 ACC/AHA hypertension guidelines and risk of cardiovascular events in a Chinese Kailuan Cohort. A total of 97,126 active and retired workers aged 18 to 98 years free of cardiovascular disease at baseline were followed for up to 10 years in the Chinese Kailuan Cohort Study. Adjusted Cox proportional hazard models were used to estimate hazard ratios and 95% confidence intervals of cardiovascular events among different blood pressure categories. Participants with stage 1 hypertension at baseline accounted for 31.1% of the cohort. Compared with normal blood pressure (<120/80 mmHg), stage 1 hypertension had a significantly higher risk of cardiovascular events, cerebral infarction and cerebral hemorrhage, and the hazard ratios (95% confidence intervals) were 1.25 (1.11–1.40), 1.31 (1.13–1.52), and 1.45 (1.07–1.97), respectively. Over a four-year period, 43.1% of participants maintained stage 1 hypertension. Compared with the decreased blood pressure from stage 1 hypertension to normal blood pressure, the maintained stage 1 hypertension had a significantly higher risk of cardiovascular events and cerebral infarction, and the hazard ratios (95% confidence intervals) were 1.78 (1.16–2.72) and 1.94 (1.14–3.30), respectively. People with stage 1 hypertension defined by the 2017 ACC/AHA hypertension guidelines have a relatively high risk for cardiovascular events in northern China; they should be given appropriate antihypertensive interventions.
Similar content being viewed by others

Introduction
In 2015, the results from systolic blood pressure intervention trial (SPRINT) demonstrated that lowering systolic blood pressure (SBP) to less than 120 mmHg, compared with less than 140 mmHg, resulted in significantly lower rates of cardiovascular events and all-cause death [1]. Mainly based on such studies, the 2017 ACC/AHA hypertension guidelines lowered the diagnostic criteria for hypertension from 140/90 mmHg to 130/80 mmHg and defined 130–139/80–89 mmHg as stage 1 hypertension [2]. People with that blood pressure (BP) range are recommended to take drugs or undergo lifestyle interventions based on their 10-year atherosclerotic cardiovascular disease risk.
Although the new American hypertension guidelines have conveyed an important idea about early prevention, their impact on health economics should not be ignored. Taking China as an example, if the new American hypertension guidelines are adopted, the prevalence of hypertension will double among adults [3]. As a result, a heavy economic burden caused by increased spending on BP lowering will be placed on the Chinese government. Therefore, it is necessary to study the association between stage 1 hypertension and long-term cardiovascular risk in China.
Recently, the results from a Chinese multicenter cohort study showed that the risk of cardiovascular events in patients with stage 1 hypertension was 1.78 times higher than those with normal BP (<120/80 mmHg). Compared with those who maintained their BP < 130/80 mmHg for 15 years, the risk of cardiovascular events in those who maintained stage 1 hypertension was also significantly higher [4]. Another cohort study also found that among Chinese Singaporeans aged 46–65 without cardiovascular history, the risk of cardiovascular death was significantly higher in those with stage 1 hypertension than those with normal BP [5]. Both studies suggest that stage 1 hypertension is a relatively high-risk group for cardiovascular disease. The new American hypertension guidelines seem to be applicable to the Chinese population, but more relevant studies are needed to support this suggestion. Therefore, we reassessed the association between stage 1 hypertension (at baseline and longitudinal change) and the risk of cardiovascular events in the Kailuan cohort from northern China.
Methods
Study design and population
Detailed information on the Kailuan Study has been described previously [6]. In brief, the Kailuan Study of 101,510 Chinese adults (81,110 men and 20,400 women) aged 18–98 years was established when detailed information on health status and lifestyle was collected in 2006–2007. Participants are seen every two years to update information on potential risk factors and ascertain newly diagnosed disease.
In the first analysis, we enrolled 100,831 active and retired workers who participated in the 2006–2007 health examination and had complete BP data. Then, we excluded participants with a history of myocardial infarction (n = 1361), stroke (n = 2016), and cancer (n = 328). A total of 97 126 individuals (77,329 men and 19,797 women) were included in the statistical analysis for the association between baseline BP and cardiovascular events (Fig. 1).

Flow chart for the analysis of the association between baseline blood pressure and cardiovascular events. A total of 101,510 active and retired workers participated in the 2006–2007 health examination is a flow chart for the analysis of the association between baseline blood pressure and cardiovascular events. A total of 101,510 active and retired workers participated in the 2006–2007 health examination. Excluding those with incomplete blood pressure, history of myocardial infarction, stroke and cancer, 97,126 participants were included in the statistical analysis. The participants were followed until December 31, 2016. A total of 1318 myocardial infarction events, 3546 cerebral infarction events, and 950 cerebral hemorrhage events occurred
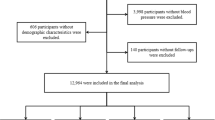
In the second analysis, we enrolled 21,428 active and retired workers who had a baseline BP of 130–139/80–89 mmHg and obtained another BP measurement from the 97,126 participants above at the 2010–2011 health examination. Then, we further excluded participants with a history of myocardial infarction (n = 160), stroke (n = 300) and cancer (n = 46) before the 2010–2011 health examination. A total of 20,922 individuals (16,480 men and 4442 women) were included in the statistical analysis for the association between longitudinal change in BP and risk of cardiovascular events among patients with stage 1 hypertension at baseline (Fig. 2).

Flow chart for the analysis of the association between changes of blood pressure and cardiovascular events. 97,126 participants with complete baseline blood pressure and without history of myocardial infarction, stroke, and cancer is a flow chart for the analysis of the association between longitudinal changes in blood pressure and cardiovascular events in people with stage 1 hypertension. Among 30,198 participants with stage 1 hypertension at baseline, we excluded those who did not participate in the 2010–2011 health examination, those without complete blood pressure data at the 2010–2011 examination, and those who had myocardial infarction, stroke or cancer between the two examinations. A total of 20,922 participants were included in the statistical analysis. The participants were followed from the time of the 2010–2011 examination until December 31, 2016. A total of 117 myocardial infarction events, 332 cerebral infarction events, and 60 cerebral hemorrhage events occurred
The study was performed according to the guidelines of the Helsinki Declaration and was approved jointly by the Ethics Committee of the Kailuan General Hospital and Hebei Medical University. Written informed consent was obtained from all participants.
Assessment of BP
BP was measured by trained research staff in the morning between 7:00 and 9:00 in the physical examination center of the Kailuan General Hospital. Smoking or drinking tea or coffee was not allowed within 30 min before the measurement of BP. Participants were asked to rest for 15 min in a seated position. Then, a calibrated mercury sphygmomanometer was used to measure the BP of the left arm with a cuff of appropriate size following the standard recommended procedures. The reading was accurate to 2 mm Hg. BP was measured twice with a 5-minute interval. The mean value of two readings was taken. If the difference between the two readings exceeded 5 mm Hg, a third measurement was required, and the mean of the three measurements was taken as the final BP value.
Assessment of covariates
Height and weight were measured by a corrected body mass scale (RGZ-120). The readings were accurate to 0.1 cm and 0.1 kg, respectively. Body mass index (BMI) was calculated as weight (kg)/height (m) [2].
Questionnaires were used to collect information about demographic, socioeconomic, and medical data, including age, sex, smoking status (“never and past”, “current, ≥1 cigarette/d”), alcohol drinking status (“never and past”, “current, ≥ 1 time/d”), education level (“elementary school”, “high school or above”), physical exercise (“none”, “occasionally and frequently, ≥1 time/wk”), income level (“ <1000 yuan/month” or “ ≥1000 yuan/month”) and use of antihypertensive drugs (“yes” or “no”).
Blood samples were collected in EDTA tubes in the morning between 7:00 and 9:00 after an overnight fasting period. Then, the blood samples were centrifuged for 10 min at 3000 r/min at 25 °C within 30 min after collection. All biochemical variables, such as fasting blood glucose, total cholesterol, high-sensitivity C-reactive protein and uric acid, were measured by an autoanalyzer (Hitachi 747; Hitachi, Tokyo, Japan) at the central laboratory of the Kailuan General Hospital. The specific methods of measurement refer to the published literature of our research group [7].
Follow-up and identification of events
Cardiovascular events included fatal or nonfatal myocardial infarction, cerebral infarction and cerebral hemorrhage. If two or more events occurred, the first event was regarded as the end point of observation. The first occurrence of myocardial infarction, cerebral infarction or cerebral hemorrhage was defined as a cardiovascular event. All participants were followed every 2 years. The time of 2006–2007 or 2010–2011 health examination was regarded as the beginning of follow-up for the first or the second analysis. The follow-up continued through December 31, 2016 or until the occurrence of cardiovascular events or the date of death. Outcome events were ascertained by the government health care system. Then, the trained researchers further identified outcome events by checking medical records from hospitals every 6 months.
Diagnostic criteria
The 2007 ESC/ACCF/AHA/WHF universal definition of myocardial infarction was adopted for the diagnosis of myocardial infarction, including dynamic changes in myocardial injury markers and the presence of any one of the following three factors: (1) ischemic chest pain symptoms; (2) new ischemic electrocardiogram changes (ST-T changes or new left bundle branch block) or new pathologic Q wave formation; or (3) imaging evidence [8]. The diagnosis of cerebral infarction and cerebral hemorrhage was mainly based on symptoms, signs and CT or MRI. The specific diagnostic criteria refer to the 1989 WHO recommendations on stroke prevention, diagnosis and therapy [9].
Statistical analyses
SAS software (Version 9.2, SAS Institute, Cary, NC) was used for statistical analyses. All statistical tests were two-sided, and P < 0.05 was considered statistically significant. Continuous variables with a normal distribution were expressed as the mean plus or minus standard deviation and compared using one-way ANOVA. Due to the skewed distribution of high-sensitivity C-reactive protein in our study, logarithmic transformation was followed by ANOVA. Categorical variables were described as percentages and compared by the Chi-square test.
To evaluate the association between baseline BP and risk of cardiovascular events, the 97,126 participants were divided into four groups according to baseline BP: the normal BP group included participants with SBP < 120 mm Hg and diastolic blood pressure (DBP) < 80 mm Hg; the elevated BP group included participants with SBP 120–129 mm Hg and DBP < 80 mm Hg; the stage 1 hypertension group included participants with SBP 130–139 mmHg or DBP 80–89 mmHg; and the stage 2 hypertension group included participants with SBP ≥ 140 mm Hg or DBP ≥ 90 mm Hg or those taking antihypertensive medication. The normal BP group was regarded as a reference. The hazard ratios (HRs) and 95% confidence intervals (CIs) of cardiovascular events, myocardial infarction, cerebral infarction and cerebral hemorrhage associated with different baseline BP groups were calculated using the Cox proportional hazard model after adjustment for age, sex, smoking, alcohol drinking, body mass index, exercise, education level, income level, fasting blood glucose, total cholesterol, uric acid, and high-sensitivity C-reactive protein.
The association between longitudinal changes in BP over four years and risk of cardiovascular events was further evaluated among patients with stage 1 hypertension at baseline. The 20,922 participants were divided into four groups according to the changes in BP from the 2006 to 2010 examination: BP-lowering group 1 (SBP/DBP: 130–139/80–89 mmHg in 2006 and <120/80 mmHg in 2010), BP-lowering group 2 (SBP/DBP: 130–139/80–89 mmHg in 2006 and 120–129/ <80 mmHg in 2010), invariant BP group (SBP/DBP: 130–139/80–89 mmHg in 2006 and 2010), and BP elevating group (SBP/DBP: 130–139/80–89 mmHg in 2006 and ≥140/90 mmHg, or antihypertensive medication use in 2010). The HRs and 95% CIs of cardiovascular events, myocardial infarction, cerebral infarction and cerebral hemorrhage associated with the different BP change groups were calculated using the Cox proportional hazard model after adjustment for the above confounders, with BP-lowering group 1 as a reference. The HRs and 95% CIs of cardiovascular events per 10/5 mmHg increase in SBP/DBP from stage 1 hypertension during the first 4 years of follow-up were also calculated using Cox regression.
Sensitivity analyses were further performed by excluding participants taking antihypertensive drugs.
Results
Baseline characteristics of different BP groups
Of the 97,126 participants, the mean age was 51, more than three quarters were men (79.6%), and 31.1% had a BP of 130–139/80–89 mmHg, which was defined as stage 1 hypertension by the new American hypertension guidelines. Table 1 shows the baseline characteristics of the participants according to BP groups. Participants in the higher BP groups were older and were more likely to be men, to exercise and have higher BMI, total cholesterol, fasting blood glucose, C-reactive protein and uric acid levels (P < 0.001 for all).
Incidence and HRs of cardiovascular events in different baseline BP groups
A total of 5550, 1318, 3546 and 950 participants developed cardiovascular events, myocardial infarction, cerebral infarction and cerebral hemorrhage, respectively, after a follow-up of 9.5 years from 2006–2007. The incidence of all cardiovascular events increased with baseline BP. Table 2 shows the HRs and 95% CIs for the association between baseline BP and risk of cardiovascular events, myocardial infarction, cerebral infarction and cerebral hemorrhage. Compared with the normal BP group, the stage 1 hypertension group had a higher risk of cardiovascular events, cerebral infarction and cerebral hemorrhage, and the HRs (95% CIs) were 1.25 (1.11–1.40), 1.31 (1.13–1.52), and 1.45 (1.07–1.97), respectively, after adjustment for age, sex and other relative confounders. Regarding the risk of myocardial infarction, there were no significant differences between the stage 1 hypertension and normal BP groups. The stage 2 hypertension group had a greater risk of cardiovascular events, myocardial infarction, cerebral infarction and cerebral hemorrhage than the normal BP group, and the HRs (95% CIs) were 2.30 (2.07–2.56), 1.66 (1.35–2.03), 2.44 (2.12–2.79) and 3.26 (2.47–4.31), respectively. After further exclusion of 9598 participants who were taking antihypertensive drugs, Cox regression analysis was performed again. The results showed no obvious changes.
Baseline characteristics of different groups of BP change
Of the 20,922 participants with stage 1 hypertension at baseline, the mean age was 48, and more than three quarters were men (78.8%). Over a four-year period, 15.1% of patients experienced a decrease in BP from stage 1 hypertension to normal BP (BP-lowering group 1), 5.5% experienced a decrease in BP from stage 1 hypertension to elevated BP (BP-lowering group 2), 43.1% maintained stage 1 hypertension (invariant BP group), and 36.3% experienced an increase in BP from stage 1 hypertension to stage 2 hypertension (BP elevating group). Supplementary table 1 shows the baseline characteristics in different groups of BP change. Participants in the BP-elevating group were older, more likely to be men, to smoke, to drink alcohol and have higher BMI, total cholesterol, fasting blood glucose, C-reactive protein and uric acid levels (P < 0.001 for all).
Incidence and HRs (95% CIs) of cardiovascular events in different groups of BP changes
A total of 493, 117, 332 and 60 participants with stage 1 hypertension at baseline developed cardiovascular events, myocardial infarction, cerebral infarction and cerebral hemorrhage, respectively, after a follow-up of 5.9 years from 2010. The incidence of all cardiovascular events gradually increased from the BP-lowering group to the BP-elevating group. Table 3 shows the HRs and 95% CIs for the association between BP changes from 2006 to 2010 and the risk of cardiovascular events among patients with stage 1 hypertension at baseline. Compared with BP-lowering group 1, the invariant BP group had a higher risk of cardiovascular events and cerebral infarction, with HRs (95% CIs) of 1.78 (1.16–2.72) and 1.94 (1.14–3.30). Regarding the risk of myocardial infarction and cerebral hemorrhage, there were no significant differences between the BP-lowering group 1 and the invariant BP group. However, the risk of cardiovascular events, cerebral infarction and cerebral hemorrhage in the BP-elevating group was significantly higher than in the BP-lowering group 1, and the HRs (95% CIs) were 3.19 (2.11–4.82), 3.29 (1.96–5.51), and 15.7 (2.13–116), respectively. After further exclusion of 935 participants who were taking antihypertensive drugs, the results did not change.
Each 10/5 mmHg increase in SBP/DBP from stage 1 hypertension during the first 4 years of follow-up was associated with a higher risk of cardiovascular events
Table 4 shows that each 10 mmHg increase in SBP from 2006 to 2010 was associated with a higher risk of cardiovascular events (HR: 1.17, 95% CI: 1.12–1.22), cerebral infarction (HR: 1.17, 95% CI: 1.10–1.24) and cerebral hemorrhage (HR: 1.27, 95% CI: 1.15–1.39) among participants with stage 1 hypertension at baseline. At the same time, it also showed that each 5 mmHg increase in DBP from 2006 to 2010 was associated with a higher risk of cardiovascular events (HR: 1.20, 95% CI: 1.14–1.26), myocardial infarction (HR: 1.15, 95% CI: 1.03–1.27), cerebral infarction (HR: 1.20, 95% CI: 1.13–1.27) and cerebral hemorrhage (HR: 1.38, 95% CI: 1.22–1.56) among participants with stage 1 hypertension. After further exclusion of 935 participants taking antihypertensive drugs, each 10 mmHg increase in SBP was associated with a higher risk of myocardial infarction (HR: 1.13, 95% CI: 1.01–1.27), while the other results did not change obviously.
Discussion
In this study, we found that the incidence of all cardiovascular events presented an increasing trend with baseline BP. After adjustment for related confounders, the risk of cardiovascular events, cerebral infarction and cerebral hemorrhage among participants with stage 1 hypertension was significantly higher than among those with normal BP.
In the second analysis, we found that 36.3% of participants experienced an increase in BP from stage 1 hypertension to stage 2 hypertension over a four-year period, and 43.1% maintained stage 1 hypertension, while only 15.1% experienced a decrease in BP from stage 1 hypertension to normal BP. The incidence of all cardiovascular events gradually increased from the BP-lowering group to the BP-elevating group. After adjustment for related confounders, the risk of cardiovascular events and cerebral infarction in the invariant BP group (maintained stage 1 hypertension) was significantly higher than in the BP-lowering group 1. Furthermore, we also found that each 10/5 mmHg increase in SBP/DBP from stage 1 hypertension was associated with a higher risk of all cardiovascular events during the first 4 years of follow-up.
Similar to our study, the Linxian Cohort Study showed that compared with stable BP of normotension ( < 120/80 mmHg), maintained prehypertension (120–139/80–89 mmHg) and having an increase in BP from normotension to prehypertension both conferred a higher risk of cardiovascular mortality among rural Chinese adults aged 40–69. It also suggested that current BP targets could be revised [10]. The multicenter cohort study, as mentioned before, showed that the HR comparing stage 1 hypertension to normal BP for cardiovascular incidence was 1.78 (95% CI 1.50–2.11). Among patients with stage 1 hypertension at baseline, 21.5% of patients maintained stage 1 hypertension over a 15-year period, and they had a 2.28-fold higher risk for cardiovascular disease (95% CI 1.28–4.06) compared with those who maintained their BP < 130/80 mmHg [4]. The above results are consistent with ours. However, the age of the study population was limited to 35–64 years, which could not represent the whole population. Moreover, subgroup analysis showed that stage 1 hypertension was not associated with a higher risk of cardiovascular events among the population aged > 60 years. This finding may be because the number of people aged > 60 years was small (only 10%), resulting in insufficient power. Our study also faced a similar problem. The number of participants aged > 60 years accounted for only 14% (the first analysis) and 8% (the second analysis) of the total population, so we did not perform age-subgroup analysis. However, further validation using a larger sample size of older people is still needed.
A large sample cohort study from Singapore found that stage 1 hypertension was associated with a higher risk of cardiovascular mortality among those aged 46–65 years and without a history of cardiovascular disease compared with normal BP (HR 1.40, 95% CI 1.01–1.94) [5]. However, the study subjects were limited to the middle-aged and elderly population, and the outcome events were only cardiovascular deaths, so the significance of the results was limited. Recently, a cohort study from America [11] and another from Korea [12] also confirmed that young adults aged < 40 years with elevated BP, stage 1 hypertension and stage 2 hypertension, defined by the 2017 American hypertension guidelines, had a significantly higher risk of cardiovascular events compared with those with normal BP. The above three studies had larger sample sizes and longer follow-up times. However, they did not analyze the association between longitudinal changes in BP and cardiovascular events. Therefore, they could explain only why higher baseline BP is associated with greater cardiovascular risk, a conclusion that has been confirmed by previous studies. However, together with our study, these studies could suggest that stage 1 hypertension has a relatively high cardiovascular risk.
In this study, we also found that, for the risk of myocardial infarction, there were no significant differences between stage 1 hypertension and normal BP. There were also no significant differences between the invariant BP group and BP-lowering group 1. In the Shanghai Women’s Health Study, high normal BP (130–139/85–89 mmHg) was also not associated with CHD mortality (HR 0.82, 95% CI 0.33–1.99). In contrast, it was associated with a 2.34 (95% CI 1.32–4.12) times higher risk of stroke mortality compared with normal BP (<120/80 mmHg) [13]. The results from the Action to Control Cardiovascular Risk in Diabetes (ACCORD) showed that targeting SBP < 120 mmHg, compared with <140 mmHg, did not reduce the risk of myocardial infarction but could significantly reduce the risk of stroke in patients with type 2 diabetes [14]. Therefore, it can be inferred that compared with people at high risk of myocardial infarction, lowering BP to < 120/80 mmHg among those with stage 1 hypertension may confer a greater benefit to those at high risk of stroke. However, we could not ignore the fact that stroke is more common than coronary heart disease in East Asia (including China).
However, compared with standard antihypertensive therapy (targeting BP < 140/90 mmHg), intensive antihypertensive therapy (targeting BP < 120/80 mmHg) may lead to adverse events such as postural hypotension, syncope, electrolyte disturbances, and acute kidney injury. SPRINT and ACCORD found that the incidence of these adverse events related to BP-lowering in the intensive antihypertensive group was significantly higher than that in the standard antihypertensive group [1, 14]; however, the follow-up time of both studies was not long, and the results still need to be further observed. As clinicians, it is important to balance the relationship between cardiovascular benefits and adverse events caused by BP-lowering.
Furthermore, our results showed that 36.3% of participants with stage 1 hypertension at baseline progressed to stage 2 hypertension over a four-year period, and this percentage may increase over time. Compared with the BP-lowering group, they are more likely to be overweight or obese, alcohol drinkers, and smokers and to have higher blood lipid, glucose, uric acid, and C-reactive protein levels. These characteristics have already been proven to be important risk factors for developing hypertension [15,16,17,18,19,20,21,22,23,24]. Therefore, to a certain extent, the improvement of lifestyle, such as limiting alcohol intake, stopping smoking, engaging in moderate exercise, losing weight and consuming a low-salt diet, may prevent BP from elevating and further reduce cardiovascular risk. Additionally, it should become the main target of intervention for patients with stage 1 hypertension because only 2.0% of the general Chinese population with stage 1 hypertension is recommended to take antihypertensive drugs according to the estimated 10-year atherosclerotic cardiovascular disease risk [25].
Limitations
Our study has some limitations. First, the BP of participants was measured by mercury sphygmomanometers rather than 24-hour ambulatory BP meters, which can provide more accurate BP values. However, 24-hour ambulatory BP measurement is not realistic in a large epidemiological study because it is time-consuming and expensive. Second, the participants were limited to active and retired workers of the Kailuan group, of which male workers account for more than three-quarters. This fact limits the extension of our results. Third, in addition to BP, other factors such as antihypertensive drugs (e.g., beta blockers, angiotensin converting enzyme inhibitors) may also have an impact on cardiovascular incidence, but the results did not change obviously after an exclusion for those taking antihypertensive drugs. Fourth, the follow-up time of this study is not long, and the number of cases of myocardial infarction and cerebral hemorrhage, as well as the number of participants in BP-lowering group 2, was not large enough, which may cause the analysis to be underpowered. Fifth, according to the 2017 ACC/AHA hypertension guidelines, BP readings should be obtained on at least two occasions to determine a person’s BP classification. However, we obtained only the BP at one occasion, which may lead to a misclassification bias.
Conclusions and Perspectives
Our study mainly found that stage 1 hypertension or maintained stage 1 hypertension had a higher risk for cardiovascular events than normal BP or decreased BP from stage 1 hypertension to normal BP. Moreover, a 10/5 mmHg increase in SBP/DBP was associated with a higher risk of all cardiovascular events among participants with stage 1 hypertension at baseline. This finding suggests that stage 1 hypertension has a relatively high cardiovascular risk among the northern Chinese population. Such patients should be paid attention to and appropriately treated. Instead of a BP intervention trial, our study is only a single-center cohort study mainly based on natural changes in BP. Therefore, more multicenter and large-sample prospective cohort studies and BP intervention trials targeting the Chinese population are needed to compensate for the deficiencies of our study.
References
SPRINT Research Group, Wright JT Jr, Williamson JD, Whelton PK, Snyder JK, Sink KM, Rocco MV, et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control. N Engl J Med. 2015;373:2103–16.
Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: a report of the american college of cardiology/american heart association task force on clinical practice guidelines. Hypertension. 2018;71:e13–e115.
Wang Z, Chen Z, Zhang L, Wang X, Hao G, Zhang Z, et al. China hypertension survey investigators. status of hypertension in china: results from the China Hypertension Survey, 2012–5. Circulation. 2018;137:2344–56.
Qi Y, Han X, Zhao D, Wang W, Wang M, Sun J, et al. Long-term cardiovascular risk associated with stage 1 hypertension defined by the 2017 ACC/AHA Hypertension Guideline. J Am Coll Cardiol. 2018;72:1201–10.
Talaei M, Hosseini N, Koh AS, Yuan JM, Koh WP. Association of “elevated blood pressure” and “stage 1 hypertension” with cardiovascular mortality among an Asian population. J Am Heart Assoc. 2018;7:e008911.
Miao C, Bao M, Xing A, Chen S, Wu Y, Cai J, et al. Cardiovascular health score and the risk of cardiovascular diseases. PLoS ONE. 2015;10:e0131537.
Jia Z, Zhou Y, Liu X, Wang Y, Zhao X, Wang Y, et al. Comparison of different anthropometric measures as predictors of diabetes incidence in a Chinese population[J]. Diabetes Res Clin Pr. 2011;92:265–71.
Thygesen K, Alpert JS, White HD. Joint ESC/ACCF/AHA/WHF Task Force for the redefinition of myocardial infarction. Universal definition of myocardial infarction. J Am Coll Cardiol. 2007;50:2173–95.
WHO Task Force on Stroke and other Cerebrovascular Disorders. Recommendations on stroke prevention, diagnosis, and therapy. Stroke. 1989;20:1407–31.
Fan JH, Wang JB, Wang SM, Abnet CC, Qiao YL, Taylor PR. Longitudinal change in blood pressure is associated with cardiovascular disease mortality in a Chinese cohort. Heart. 2018;104:1764–71.
Yano Y, Reis JP, Colangelo LA, Shimbo D, Viera AJ, Allen NB, et al. Association of blood pressure classification in young adults using the 2017 american college of cardiology/american heart association blood pressure guideline with cardiovascular events later in life. JAMA. 2018;320:1774–82.
Son JS, Choi S, Kim K, Kim SM, Choi D, Lee G, et al. Association of blood pressure classification in korean young adults according to the 2017 american college of cardiology/american heart association guidelines with subsequent cardiovascular disease events. JAMA. 2018;320:1783–92.
Dorjgochoo T, Shu XO, Zhang X, Li H, Yang G, Gao L, et al. Relation of blood pressure components and categories and all-cause, stroke and coronary heart disease mortality in urban Chinese women: a population based prospective study. J Hypertens. 2009;27:468–75.
ACCORD Study Group, Cushman WC, Evans GW, Byington RP, Goff DC Jr, Grimm RH Jr, Cutler JA, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus. N Engl J Med. 2010;362:1575–85.
Huang Y, Deng Z, Se Z, Bai Y, Yan C, Zhan Q, et al. Combined impact of risk factors on the subsequent development of hypertension. J Hypertens. 2018. https://doi.org/10.1097/HJH.0000000000001956.
Lee JH, Yang DH, Park HS, Cho Y, Lee WK, Chun BY, et al. Hypertension-diabetes daegu initiative study investigators. incremental predictive value of high-sensitivity c-reactive protein for incident hypertension: the hypertension-diabetes daegu initiative study. Clin Exp Hypertens. 2014;36:302–8.
Stranges S, Wu T, Dorn JM, Freudenheim JL, Muti P, Farinaro E, et al. Relationship of alcohol drinking pattern to risk of hypertension: a population-based study. Hypertension. 2004;44:813–9.
Cornelissen VA, Smart NA. Exercise training for blood pressure: a systematic review and meta-analysis. J Am Heart Assoc. 2013;2:e004473.
Harsha DW, Bray GA. Weight loss and blood pressure control. Hypertension. 2008;51:1420–5.
Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an independent risk factor for cardiovascular disease: a 26-year follow-up of participants in the Framingham Heart Study. Circulation. 1983;67:968–77.
Lesniak KT, Dubbert PM. Exercise and hypertension. Curr Opin Cardiol. 2001;16:356–9.
Hayashi T, Tsumura K, Suematsu C, Okada K, Fujii S, Endo G. Walking to work and the risk for hypertension in men: the Osaka Health Survey. Ann Intern Med. 1999;131:21–26.
Klatsky AL. Alcohol and cardiovascular mortality: common sense and scientific truth. J Am Coll Cardiol. 2010;55:1336–8.
Shankar A, Klein R, Klein BE, Nieto FJ. The association between serum uric acid level and long-term incidence of hypertension: Population-based cohort study. J Hum Hypertens. 2006;20:937–45.
Wang JG, Liu L. Global impact of 2017 American College of Cardiology/American Heart Association Hypertension Guidelines: a perspective from China. Circulation. 2018;137:546–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Ji, C., Wu, S., Shi, J. et al. Stage 1 hypertension defined by the 2017 ACC/AHA Hypertension Guidelines and Risk of Cardiovascular Events: a Cohort Study from Northern China. Hypertens Res 42, 1606–1615 (2019). https://doi.org/10.1038/s41440-019-0268-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-019-0268-9
Keywords
This article is cited by
-
Prevalence of high blood pressure under 2017 ACC/AHA guidelines: a systematic review and meta-analysis
Journal of Human Hypertension (2021)
-
Cardiovascular events associated with stage 1 hypertension in Asian populations: is this a more critical issue in younger adults?
Hypertension Research (2019)
