
Abstract
Introduction Virtual reality (VR) is gaining recognition as a valuable tool for training dental students and its use by dental schools around the world is growing. It is timely to review the literature relating to the use of VR in dental education, in order to ensure that educators are well-informed of current areas of inquiry, and those requiring further investigation, to enable appropriate decisions about whether to employ VR as a teaching tool. Method A scoping review using the method outlined by Arksey and O'Malley was conducted. Both Web of Science and ERIC databases were searched. Inclusion and exclusion criteria were established to filter results. The data were collected and categorised using a custom data collection spreadsheet. Results The review identified 68 relevant articles. Following review, four educational thematic areas relating to the 'simulation hardware', the 'realism of the simulation', 'scoring systems' and 'validation' of the systems emerged. Conclusion This paper summarises and draws out themes from the current areas of inquiry in the literature, uncovering a number of weaknesses and assumptions. It recommends areas where additional investigation is required in order to form a better evidence base for the utility of VR in dental education, as well as to inform its future development.
Similar content being viewed by others


Key points
-
Summarises the current trends of virtual reality in dental education.
-
Questions a number of underlying assumptions in the current literature.
-
Identifies emergent themes in the current literature and makes recommendations for further investigation.
Introduction
Simulation has been part of dental training since the late 1800s,1,2 but the idea of using simulation based on virtual reality is relatively new. Currently, within dental education, virtual reality (VR) is used as an umbrella term to describe a number of technologies, from full three dimensional (3D) headsets that immerse the user in a virtual world, to systems that perform automated assessment of students performing cavity preparations on enhanced phantom heads equipped with stereoscopic cameras. The adoption of VR has been driven by limitations of traditional approaches in finding real world cases, lack of availability of tutor time, limitations of plastic teeth to simulate realistic experiences, and the subjectivity of assessment.3
VR systems are achieving recognition as a valuable tool for training dental students, and are being employed in dental schools around the world. This growing acceptance means that it is timely to review the literature relating to the use of VR in dental education, in order to ensure that educators are well-informed of current areas of inquiry and those requiring further investigation, and to enable appropriate decisions about whether to employ VR as a teaching tool. This work aims to identify any obvious omissions, areas of weakness, or assumptions within the literature which would benefit from further research in order to better inform pedagogic strategy.
Method
This scoping review was conducted using the methodology outlined in Arksey and O'Malley.4 This method provides a framework by which a field can be explored to identify any gaps in the evidence base, summarise existing research and disseminate findings in a comparatively short amount of time, when compared to a full systematic review. While the approach is not without its limitations, for example, the quality of the primary data surveyed is not assessed; it does allow for a wider breadth of literature to be surveyed and a broader question to be addressed. For the purposes of this study, this approach allowed a breadth of literature from different disciplines discussing the use of VR in dental education to be reviewed, which a more rigid systematic review approach might have excluded.
The research question to be addressed was: 'what are the uses and applications of virtual reality in dental education?' Relevant literature was sourced via Web of Science and the Educational Resources Information Centre (ERIC) databases. Web of Science is a multi-database search engine that allows most of the relevant sources to be consulted via a single search interface, whereas ERIC is a curated database focused on educational literature from journals, grey literature and individual submissions. A broad strategy was adopted to capture as much of the relevant literature as possible, with the intention of systematically filtering this later. There was no restriction on study design, source or date of publication, however, only papers written in the English language were included.
The first step was to find all sources mentioning the concept of 'virtual reality' in the title, within the topic area of dentistry. The terms 'virtual reality', 'VR' and the less common 'virtual environment' were selected as search fields. Additionally, in dentistry, VR dental simulation is often colloquially referred to as 'haptics'; this is known to appear in the title of a number of papers so it was also included in the search criteria. The topic area was restricted to 'dentistry' because while there is much research in the wider medical literature concerning the use of virtual reality, the objective of this review was to specifically investigate dental applications.
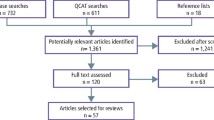
A broad search, querying titles containing the terms 'Virtual Reality OR VR OR Virtual Environment OR Haptic*' (with a restriction to topic areas of dent*), was performed on the Web of Science database and an equivalent search was performed against the ERIC database. A union of the two result sets was passed to the filtering stages (Fig. 1).

Literature search process
To begin the filtering process, titles were reviewed for any results that could be easily excluded from further analysis. Criteria for exclusion at this stage were papers that were clearly not relevant and simply shared key words used in different contexts, or were found as a result of a search term being found within another word. Abstracts were retrieved for the remaining results and evaluated against a series of inclusion criteria for the study:
-
1.
Papers describing the development of a dental simulator for use in education
-
2.
Evaluation of simulation in dental education and skills development
-
3.
Perception of simulation in dental education.
These criteria meant that work concerned with, for example, modelling dental occlusion via virtual reality articulators, use of virtual reality for dealing with dental anxiety, and the design of haptic algorithms/mathematical models for dental simulation were all excluded. The remaining papers were read in full and tagged into a data extraction spreadsheet based on emergent themes. Papers with shared attributes on the extraction spreadsheet were collated for summary and discussion.
Results and discussion
The search produced 128 results. Of these results, 29 were excluded during the title filtering process. After reviewing the abstracts, a further 28 results were excluded. Retrieval of the full text for the remaining 71 papers was attempted. The full text of two papers could not be retrieved and one duplicate was identified, so 68 papers in total were included in this study.
The relevant articles spanned a time period of 2002-2017. References for the papers included in this review and the categorisation of the publication they were printed in are shown in Table 1. Most papers in this review evaluated an operative or educational task, with a prevalence of cutting tasks such as cavity preparation. The frequency of each type of study and the references are summarised in Table 2.
Based on the results of the tagging processes, the following broad thematic areas emerged:
-
1.
Simulation hardware
-
2.
The realism of the simulation
-
3.
Automated feedback and scoring
-
4.
Validation of the exercises and the role of the tutor.
These four thematic areas will be discussed in turn and, as prescribed by the scoping review methodology, quantitative indications will be provided to illustrate the coverage of each attribute found within the literature.
1. Simulation hardware
This thematic area discusses aspects of the physical simulation hardware. Observations are made covering:
-
The simulator's form factor
-
The simulated tool
-
The force reproduction capabilities of the haptic arm
-
The presence of a finger rest in the simulator design
-
The use of simulated 3D depth.
Simulator form factor
The term 'virtual reality' has been applied to a number of different types of hardware. While there is no standardised form factor for a VR dental simulator, the simulators that emerged in this review can be classified into four broad types:
-
1.
Desktop PCs
-
2.
Haptic desktops
-
3.
Dental skills trainers
-
4.
Digitally-enhanced phantom heads.
Desktop PC
The simulator type most ergonomically removed from the interactions that would occur in a real clinical environment was the desktop PC. This was reported by one publication and used a traditional keyboard and mouse to control a handpiece for cavity preparation exercises.24 The affordance of a keyboard and mouse, in comparison to an actual handpiece, is considered to be very low for this task.
Haptic desktops
To represent the 3D nature of the interactions that occur in dentistry, many groups enhanced their systems with one or more haptic arms (Fig. 2) to produce a 'haptic desktop', as pictured in Figure 3. A haptic arm is a hardware device that allows the operator to receive tactile feedback in response to events triggered by the software, simply by holding and manipulating the device. This could allow the operator to feel like they are making contact with a physical tooth and as they run the virtual tool across its surface to feel the surface features. In reality, this sensation is being produced by electric motors responding to the user's movements. This was the most common type of hardware configuration reported in the literature (reported by 28 of the 69 papers reviewed).

3D Systems Touch X. Reproduced with permission from 3D Systems, USA

3 A student using a haptic desktop. Reproduced with permission from Siriwan Suebnukarn
One publication reported an alternative realisation of the haptic desktop, whereby the computer monitor was replaced with an augmented reality (AR) headset.12 These devices allow digital imagery to be projected onto the user's surroundings. This work projected a 3D tooth in front of the user, so that they could operate on it via a table top-mounted haptic arm.
Dental skills trainers
Dental skills trainers, as reported by 17 papers, are arguably the closest devices in concept to 'flight simulators' for dental education (Figs. 4 and 5). These take the haptic desktop approach one step further by providing a bespoke enclosure for the hardware. This enclosure adds dental specific features to facilitate a better operating position, such as a finger rest stage and height adjustment controls, recreating some of the environmental 'physicality' that is present in flight simulators.

A dental skills trainer. Reproduced with permission from HRV Simulation, France

A dental skills trainer. Reproduced with permission from Moog, USA
Digitally-enhanced phantom heads
Taking a different approach, four publications reported the use of digitally-enhanced phantom heads. These devices are based on a traditional phantom head and employ real dental tools. The operator works using preformed plastic 'typodont' teeth of known dimensions and a 3D camera tracks the operator's movements, recording handpiece activity. This information allows a digital recreation of the work to be produced so that students' performance can be visualised and assessed. It is debatable if these devices should be considered 'virtual reality' simulators as, arguably, they are closer to a computer assisted assessment/recording tool than what would traditionally be understood to be VR.
These four categorisations show significant differences between the hardware that supports VR in dentistry and this is reflected in the research studies reported in the literature. This raises questions about how translatable the findings are. The degree to which the design of the hardware impacts on the transferability or validity of the clinical skills that are developed is currently unknown.
The simulated tool
The tool attached to the haptic arm can take a generic form, or employ a more realistic facsimile of the actual dental instrument to be used. The majority of the papers surveyed (40 of 65 papers who reported using a computer input device) reported that the tool held by the operator was simply the stylus supplied by the haptic arm manufacturer. As can be seen in Figure 2, this resembles a marker pen in size and has a rubberised grip and clickable button. Only 11 of the 65 devices reported had a realistic facsimile of the relevant instrument for the operator to use and interact with the simulation.
Five studies reported the use of abstract modes of interaction to elicit real operative events in the simulation environment; for example, when recreating exodontia (extraction), the user would apply virtual forceps using the haptic arm, and then click a button in order for the forceps to 'grip' the tooth within the simulated environment.26 In another example, rather than switching to an amalgam carrier, the user would place the handpiece in 'restoration mode' whereby amalgam would grow from the tip of the handpiece to fill the prepared cavity.31 There were no obvious debates in the literature surveyed concerning the impact that tool affordance, fidelity or interaction mode has on the development and transferability of dental operative skills.
Force reproducibility
Haptic arms simulate the feeling of touching a real object via electric motors at the articulation points, providing resistance against the user's movements. By providing different amounts of torque, materials of different hardness can be simulated. To fully simulate all of the possible movements (degrees of freedom), a haptic arm must replicate six planes of movement: the translational, which represent movement in the x, y and z axes; and the rotational, which include pitch (vertical rotation), yaw (horizontal turning rotation) and roll (tilting rotation) (Fig. 6). In addition to tracking these movements, the haptic arm must also be able to apply forces to resist the movements in these directions. However, 46 of the papers reported using haptic arms that were not able to provide resistance in the rotational directions. The consequence of using a haptic arm that can only represent the translational forces is that if the simulated procedure requires any rotation at the tip of the tool, or if the user mistakenly rotates the tool, the system is unable to provide any tactile feedback to guide or correct this movement. Only four papers reported that they used the much more expensive haptic arms that could resist movements in all six directions.

Axes of movement
In addition to being able to exert a force in all directions, there is also the factor of the amount of force that the haptic arm can exert. For example, the 3D Systems Touch and Touch X haptic arms, reported in many of the papers, are capable of producing a maximum of 2.35 N/mm of force.41 While this amount of force may be sufficient to simulate the forces involved in many dental procedures, it is not sufficient for them all. For example, in a report of the development of a simulator to train the motions necessary for a dental extraction26 the haptic arm reported in the study was incapable of fully reproducing the forces involved in this procedure by several orders of magnitude.73 Only five papers directly recognised there might be an issue with this lack of output power, although an additional eight papers inferred an awareness.
Related to the forces reproduced by the haptic arm is the operator's perception of those forces. The wearing of gloves of various materials compared to ungloved has been shown to significantly impact the perception of touch.74 However, none of the papers surveyed mention this as a factor influencing the simulation and just three papers picture operators wearing the full personal protective equipment, as would be worn in a clinical setting. This may introduce differences in the perception of the forces involved when translating to a real clinical environment.
The impact of training using an unrealistic force, with incomplete directions of force feedback and without normal protective equipment, is currently unexplored and may affect simulation acceptance, learning and the transferability of skills.
Finger rests
A safe finger rest is a critical element regarding handpiece control. Its value is stressed to dental trainees through recommended curricula75,76 and essential operative dental texts.77,78 It provides stability, a fulcrum for the actions of tools, and maintains contact with the patient in readiness for unexpected movements. However, despite its importance, only 14 of the 69 papers reported or illustrated hardware where a safe operating finger rest could be achieved, with just six papers explicitly acknowledging it as a factor in their hardware design. Five papers reported the use of a wrist rest built into a mouse pad. However, 22 reported hardware offering no support at all, resulting in the operator's hands being completely unsupported. The impact that the absence of a finger rest had on these studies is unknown.
Simulated 3D depth
Operative dentistry is a spatially complex task occurring in 3D space. Computer monitors are conventionally 2D, but some are able to simulate 3D depth by presenting different images to each eye via the use of stereoscopic glasses. Twenty-two of the papers reported the use of such hardware. Fully immersive virtual and augmented reality headsets can also reproduce 3D depth, as reported by six papers. Seventeen papers reported that they did not provide any 3D representation. This review only found one paper that investigated the importance of stereoscopy in a dental context.40 However, the authors failed to account for a confounder whereby using 3D glasses for their 2D display resulted in some participants suffering from eyestrain and headaches. As a result, their findings, that indicate a preference towards 3D display, could be considered unreliable.
In addition to stereoscopy, three-dimensional depth can be perceived in a number of other ways including inference from relative size, perspective and parallax effects. Only providing technologies to support stereoscopy, however, is unlikely to be sufficient for a spatially complex task like operative dentistry. While each eye is provided with an independent view, this does not allow the operator to move their head and check the angulation of their tool relative to the object being worked on. Only seven papers reported systems that could track head movement, of which six reported fully immersive VR/AR headsets. The question of the optimal method of producing a 3D effect, if one is even needed at all, and the effect of not being able to utilise other ways of perceiving depth in a dental context is currently unknown.
2. The realism of the simulation
The concept of 'real' and the need for the simulation to be as realistic as possible was widespread in the literature reviewed. Almost half of the papers surveyed claimed that realism is important, with 20 making direct claims to its necessity and a further 14 clearly inferring it. Quotes such as 'resemble reality as closely as possible'6 or 'the system should simulate as closely as possible the real clinical activity with patients'60 were common. At first glance, this does not seem to be an entirely unreasonable aim, however, nowhere that this assumption is stated is it supported with reference to relevant literature. The wider medical literature suggests that the outcomes from a high fidelity simulator offer no statistically significant benefit compared to a low fidelity simulation.79 Only three authors question the importance of realism, and this is perhaps framed more as a question of 'how much realism is needed'41 rather than questioning if the pursuit of reality is desirable.
Measurement of how 'realistic' participants found the simulation was undertaken by 16 of the papers in this review. In many cases this was done by asking participants the question 'is it realistic?' However, the measurement of 'realism' is a multi-faceted task and this kind of question can be interpreted in different ways, so it cannot be known if the respondent is referring to the visual appearance, the tactile feel, the sounds or even the subjective representation of the simulation world inside the user's head.80 Additionally, different baseline expectations of participants can also cloud the responses to such a question.
Most of the questioning into the realism of the simulation identified in this review has focused on the software aspect. However, even dental skills trainers with their bespoke dental-specific housings, discussed above, are somewhat removed from the ergonomics of a clinical environment. If we look at other disciplines such as aviation, the European Aviation Safety Agency defines certification specifications and categorisations for flight simulators.81 These range from a full flight simulator, with an accurate full size replica of a specific aircraft, views out of the cockpit and replication of the movements and forces, to a more basic desktop instrument training device that permits a trainee to learn the procedural aspects of flight. The differences in the fidelity of devices are recognised in aviation training by allowing appropriate simulator time to count towards flight accreditation.82 The impact of the simulator ergonomics for dental skills training should similarly be assessed, so that the effect on the translation of skills of training using different devices can be measured.
A 'real' tooth
A possible consequence of the drive towards realism is that roughly two thirds of the papers in this review (46 of 69) used realistic teeth or oral structures. However, this drive towards making the tooth look realistic may unintentionally shift expectations towards realism in every aspect, leading to rejection of the experience by learners and tutors.
Writers in both illustration83 and robotics84 have observed that as the realism of a representation increases, undesirable side effects start to occur. If these observations are also present in VR dental simulation, the realistic simulated tooth would cease to be an abstract substrate on which a skill can be learned and become a tooth that is now expected to share all of the properties, feel and anatomical cues of the real structure. By adding further details to the virtual model, the focus of the exercise would blur from skills education to 'true to life' simulation. A possible consequence of this shift in expectations towards realistic simulation is that, now, any shortcomings in that representation could become the focus of criticism and lead to rejection of the simulation as a whole. The pedagogic effects of realism in dental simulation and how it impacts on both learning and acceptance are unreported in the current dental education literature.
Alternatives to teeth
Abstract or non-tooth shapes were the main approach reported by 11 of the papers in this study. These works did not draw attention to the fact that the exercise was not on a tooth or that this may even present a problem. One two-part series of studies46,47 led to the development of a folded torus-shaped manual dexterity test. Performance based on this shape was found to be discriminatory and could identify students who would require additional support with regard to their fine motor control. This clearly indicates that not being realistic does not preclude being useful and starkly contrasts with the presumption that realism is an essential attribute.
An interesting middle-ground was reported in the development of 'caries blocks'28 which, despite being cube-shaped, contained patterns and the variable densities found in a real carious lesion. Despite the 'unrealistic' appearance of these exercises, the authors claim they were well received by students and allowed an important concept to be developed without introducing the confounding effects of a realistic tooth shape.
These observations and assumptions regarding the realism of dental simulation can be related to an observation from the aviation simulation literature arguing that 'there will need to be a shift in focus from the designing of simulation for realism (and hope that learning occurs) to the design of human-centred training systems that support the acquisition of complex skills.'85 This is also referred to as deliberate practise and at present the use of this pedagogic approach is underreported in dental education. Further studies should explore the value of deliberate practise, which in turn will inform the degree of fidelity and realism that are required from modern simulation systems.
3. Automated feedback and scoring
Immediate feedback was regarded as an important aspect, with 38 of the publications reporting that their simulators gave immediate feedback. A number of approaches were evident in the literature:
-
1.
Target-based feedback
-
2.
Motion and force exertion tracking
-
3.
Time taken
-
4.
Clinical feedback.
Target-based
The most common feedback method, offered to users by 13 of the simulators reported, is target-based feedback. Here, the operator is presented with a 3D target area that they are instructed to remove using a dental handpiece. Feedback is then given using a combination of:
-
1.
The amount of the target shape removed
-
2.
How much damage was done to the area outside of the target
-
3.
How much time was spent on the exercise.
While it has been recognised that this approach has not yet been fully validated,41 it has a number of limitations that have not been explored in the literature. The provision of a percentage or volume of material removed inside or outside of a target area might not be a useful metric for the learner. Effectively, this approach is measuring the agreement between the shape produced by the user and a pre-programmed exercise target. However, not all material in a tooth or deviation from a target is equal. Removing a few cubic millimetres of material around the edge of the margin would still likely result in a restorable tooth, however, removing that same volume of material straight down and into the pulp would be much more serious. An appreciation of this difference is not always fully represented in this scoring method, so it might mislead a student as to what their real clinical performance would be. Furthermore, the scoring approach is only a measure of the final product, so does not consider the rationale underpinning the student's operative decisions. For example, was there a degree of poor handpiece control, lack of a finger rest, or poor posture, which drew the outcome away from the student's intended outcome? Similarly, was there a fundamental misunderstanding by the student in relation to their operative strategy? A feedback mechanism that reports these specific aspects, and allows a student to critically reflect on their performance, is not currently reported in the literature.
Motion and force exertion tracking
Nine studies reported capturing the motions of the handpiece and pressures applied by a user. This information was then used as the basis for comparison with an expert's performance on the same exercise. Comparing a student's performance with an expert in this way is using more factors than the shape agreement method previously discussed, however, to what extent are these actually the distinctions between levels of competence that should be focused on and how sophisticated are the comparisons? Informing a student that on this particular tooth, in this particular exercise, they should press harder here, or use a shorter stroke there, does not necessarily correlate with the internalisation of that skill so it can be transferable to other contexts.
Time taken
While learning and developing a skill, knowing how much time was taken may not be a useful metric. Yet 25 of the papers reported that they measured the student's operating time, combining it with the feedback methods noted previously. It may be true that an expert can perform a procedure more quickly than a novice, but providing this metric simply informs the novice of this fact without offering any guidance on how to achieve mastery. Additionally, it has been shown that introducing time pressures can negatively impact a novice's performance and impede their ability to concentrate on the factors that actually would lead to an improved performance.86
Clinical feedback
Finally, nine papers reported assessment based on other clinical measures, for example, drilling angle, drilling depth, presence of perforations, but assessment of these was often provided manually in conjunction with feedback from a tutor.
So, while many authors have shown that their simulators are able to reliably discriminate between novice and expert operators using these assessment methods, the extent to which they measure what matters, encourage desirable changes, or lead to transferable improvements in performance, requires further investigation.
4. Validation of the exercises
Given that most of the current generation of simulators adopt a 'shape agreement' approach to assessment, it is reasonable to ask how those prescribed shapes are arrived at and if they are objectively correct. The shape agreement scoring method can be considered appropriate when the user is asked to remove a simple shape from a block, because the accuracy of the agreement is the main consideration. However, with a tooth-based exercise the student is evaluating their performance, validating the decisions they made and their understanding of the procedure based on inferences taken from the deviation of their attempt from the target shape. It is vital, therefore, that these target shapes are clinically accurate. Only 16 papers detailed the process by which their exercises were created, and even these descriptions did not cater for any difference of opinion as to how the exercise should be solved.
The role of the tutor
When teaching in a simulation environment, tutors have been observed to compensate for shortcomings of the simulation.87 However, 21 of the 69 surveyed papers claim, or infer, that a cost saving is possible by relying on the simulator's feedback and dispensing with the tutor's presence. For this to be an acceptable step, the simulators must be seen to be valid for this purpose. However, half of the papers surveyed and almost half of those investigating a simulator's validity (6 of 13) originated in computer science publications. This might lead to the question of 'valid in terms of what?' If we compare simulators to the combination of wet phantom heads and tutor supervision, how many simulators tell students about their final cavity form, or indeed conceptual errors such as posture, or handpiece angulation, which are impacting critically on the outcome? When we talk about 'validity', do we wish to compare the feedback that simulators provide to 'real clinical feedback', or in comparison to a quantitative removal of zones of tooth tissue?
At present, simulator feedback does not have enough utility to fully replace the tutor and become an unsupervised activity. In isolation, it may be possible for a student to achieve high scores on a simulator exercise, yet be clinically ill-prepared for operative treatment on real patients.
General discussion
This scoping review suggests that there are tensions within the literature on the use of virtual reality simulation in dental education. Their purpose and where they fit in to the educational programme is not clear. Different authors place simulators as fulfilling different roles: should they simulate real procedures as accurately as possible in order to allow additional practice in a safe environment? Are they a tool to diagnose students who lack fine motor skills and who will likely struggle in pre-clinical exams? Or, are they a teaching tool with which to develop understanding of specific dental concepts and provide a safe and cost-effective learning environment? These are not mutually exclusive goals, but recognising that there are sometimes trade-offs between them may inform future development efforts. Additionally, an area missing from the discussion in the literature is the student's overall perception of the presence of VR simulators. As potentially fee-paying stakeholders, should they expect the latest equipment and facilities to be part of their training regardless of the actual utility?
The current generation of dental simulators have been driven by a desire to recreate current teaching methods and this has led to the creation of representational systems, effectively, a digital phantom head.60 However, this has resulted in creating an incomplete facsimile of an existing modality that begs comparisons with an established and familiar training device. Is the objective that VR simulation may one day replace traditional phantom head-based training, in which case many of the issues discussed above must be addressed; or alternatively, is the greatest opportunity for VR-based training to create something new but complementary to traditional training methods and together produce better educational outcomes?
Conclusions
This paper provides an important review of the current literature regarding VR simulation for dental education and it has highlighted a significant number of weaknesses and underlying assumptions in the existing literature. The authors recommend a number of areas requiring further investigation:
-
1.
There are no established educational standards for dental simulators or their associated exercises
-
2.
It is unclear how the variable fidelity across simulator systems may impact on skills acquisition
-
3.
A number of core operative concepts are underrepresented within the simulator environment such as a finger rest and student posture. The way in which this impacts on student development is unclear
-
4.
Comparisons between the relative importance of different methods of perceiving 3D depth for simulation-based dental training are not reported in the literature
-
5.
Further study should explore the value of deliberate practise, which in turn will inform the degree of fidelity and realism that are required from modern simulation systems
-
6.
The scoring mechanisms employed by many simulators have not been validated in relation to actual clinical performance and clinical tutor feedback
-
7.
The way in which VR is introduced and integrated into curricula is variable and its impact on student satisfaction and progression is unknown
-
8.
The synergy between clinical tutor and simulator-generated feedback must be further explored in order to maximise pedagogic value and the efficient utility of resources.
References
University of Glasgow. The University of Glasgow Story: Edward Oswald Fergus. 2010. Available at http://www.universitystory.gla.ac.uk/biography/?id=WH0736&type=P (accessed February 2019).
Owen H. Simulation in Dentistry and Dental Hygiene. In Owen H (ed) Simulation in Healthcare Education: An Extensive History. pp 431-450. Berlin: Springer, 2016.
Xia P, Mendes Lopes A, Restivo M T. Virtual reality and haptics for dental surgery: A personal review. Vis Comput 2013; 29: 433-447.
Arksey H, O'Malley L. Scoping studies: Towards a methodological framework. Int J Soc Res Methodol 2005; 8: 19-32.
Plessas A. Computerized Virtual Reality Simulation in Preclinical Dentistry: Can a Computerized Simulator Replace the Conventional Phantom Heads and Human Instruction? Simul Healthc 2017; 12: 332-338.
de Boer I R, Lagerweij M D, de Vries M W, Wesselink P R, Vervoorn J M. The Effect of Force Feedback in a Virtual Learning Environment on the Performance and Satisfaction of Dental Students. Simul Healthc 2017; 12: 83-90.
Kolesnikov M, Žefran M, Steinberg A D, Bashook P G. PerioSim: Haptic virtual reality simulator for sensorimotor skill acquisition in dentistry. 2009 IEEE International Conference on Robotics and Automation 2009; 689-694.
Wang D, Zhang Y, Sun Z. Multi-Modal Virtual Reality Dental Training System with Integrated HapticVisualAudio Display. In Tarn T J, Chen S B, Zhou C (eds) Robotic Welding, Intelligence and Automation. pp 453-462. Berlin: Springer, 2007.
Rhienmora P, Haddawy P, Suebnukarn S, Dailey M N. A VR Environment for Assessing Dental Surgical Expertise. Proceedings of the 2009 conference on Artificial Intelligence in Education: Building Learning Systems that Care: From Knowledge Representation to Affective Modelling. 2009; 746-748.
Tse B, Harwin W, Barrow A, Quinn B, San Diego J, Cox M. Design and Development of a Haptic Dental Training System - hapTEL. In Kappers A M L, van Erp J B F, Bergmann Tiest W M, van der Helm F C T (eds) Haptics: Generating and Perceiving Tangible Sensations. pp 101-108. Berlin: Springer, 2010.
Somrang N, Chotikakamthorn N. Interactive haptic simulation of dental plaque removal. 2006 International Symposium on Communications and Information Technologies. 2006; 319-322.
Rhienmora P, Gajananan K, Haddawy P et al. Haptic augmented reality dental trainer with automatic performance assessment. Proceedings of the 15th international conference on Intelligent user interfaces. 2010. 425-426.
Zheng F, Lu W F, Wong Y S, Foong K W C. Graphic Processing Units (GPUs)-Based Haptic Simulator for Dental Implant Surgery. J Comput Inf Sci Eng 2013; 13: 041005.
Chen L Y, Fujimoto A, Miwa A, Abe T, Sumi A, Ito Y. A dental training system using virtual reality. Proceedings 2003 IEEE International Symposium on Computational Intelligence in Robotics and Automation. Computational Intelligence in Robotics and Automation for the New Millennium. 2003; 430-434.
Jamieson E S, Chandler J H, Culmer P R, Manogue M, Mon-Williams M, Wilkie R M. Can virtual reality trainers improve the compliance discrimination abilities of trainee surgeons? 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society. 2015; 466-469.
Wang D, Zhang Y, Hou J et al. iDental: A haptic-based dental simulator and its preliminary user evaluation. IEEE Trans Haptics 2012; 5: 332-343.
Li Y, Zhang S, Ye X. Penalty-based haptic rendering technique on medicinal healthy dental detection. Multimed Tools Appl 2017; 76: 10825-10835.
Rhienmora P, Haddawy P, Khanal P, Suebnukarn S, Dailey M N. A virtual reality simulator for teaching and evaluating dental procedures. Methods Inf Med 2010; 49: 396-405.
Germans D M, Spoelder H J W, Renambot L, Bal H E, van Daatselaar S, van der Stelt P. Measuring in Virtual Reality: A case study in dentistry. IEEE Trans Instrum Meas 2008; 57: 1177-1184.
Medellín-Castillo H I, Govea-Valladares E H, Pérez-Guerrero C N, Gil-Valladares J, Lim T, Ritchie J M. The evaluation of a novel haptic-enabled virtual reality approach for computer-aided cephalometry. Comput Methods Programs Biomed 2016; 130: 46-53.
Ioannou I, Kazmierczak E, Stern L. Comparison of oral surgery task performance in a virtual reality surgical simulator and an animal model using objective measures. Conf Proc IEEE Eng Med Biol Soc 2015; 5114-5117. DOI: 10.1109/EMBC.2015.7319542.
Syllebranque C, Duriez C. Six degree-of freedom haptic rendering for dental implantology simulation. In Syllebranque C, Duriez C (eds) Biomedical Simulation. pp 139-149. Berlin: Springer, 2010.
Deshpande S, Nahavandi S, Mullins J, Khan M B, Creighton D. Enhancing audio-haptic enabled novel dental training platform performance. ASME 2012 International Design Engineering Technical Conferences and Computers and Information in Engineering Conference. 2012; 1371-1376. DOI: 10.1115/DETC2012-70666.
Mohamed N F F, Luke D A. Virtual reality on the WWW: Simulating class I procedures in restorative dentistry. Student Conference on Research and Development. 2002; 360-363. DOI: 10.1109/SCORED.2002.1033132.
Wang D, Zhao X, Shi Y, Zhang Y, Hou J, Xiao J. Six DegreeofFreedom Haptic Simulation of Probing Dental Caries Within a Narrow Oral Cavity. IEEE Trans Haptics 2016; 9: 279-291.
Wang D, Tong H, Shi Y, Zhang Y. Interactive haptic simulation of tooth extraction by a constraint-based haptic rendering approach. IEEE International Conference on Robotics and Automation (ICRA). 2015; 278-284. DOI: 10.1109/ICRA.2015.7139012.
Escobar-Castillejos D, Noguez J, Neri L, Magana A, Benes B. A Review of Simulators with Haptic Devices for Medical Training. J Med Syst 2016; 40: 104.
Osnes C, Keeling A J. Developing haptic caries simulation for dental education. J Surg Simul 2017; 4: 29-34.
Wu J, Wang D, Wang C C L, Zhang Y. Toward Stable and Realistic Haptic Interaction for Tooth Preparation Simulation. J Comput Inf Sci Eng 2010; 10: 021007.
Luciano C, Banerjee P, DeFanti T. Haptics-based virtual reality periodontal training simulator. Virtual Real. 2009; 13: 69-85.
Kim L, Park S H. Haptic interaction and volume modeling techniques for realistic dental simulation. Vis Comput 2006; 22: 90-98.
Wang D X, Zhang Y, Wang Y, Lu P. Development of dental training system with haptic display. 12th IEEE International Workshop on Robot and Human Interactive Communication. 2003; 159-164. DOI: 10.1109/ROMAN.2003.1251836.
Luciano C, Banerjee P, DeFanti T, Mehrotra S. Realistic cross-platform haptic applications using freely-available libraries. Proceedings. 12th International Symposium on Haptic Interfaces for Virtual Environment and Teleoperator Systems. 2004; 282-289. DOI: 10.1109/HAPTIC.2004.1287207.
Wang D, Zhang Y, Wang Y, Lü P, Zhou R, Zhou W. Haptic rendering for dental training system. Sci China, Ser F Inf Sci. 2009; 52: 529-546.
Konukseven E I, Onder M E, Mumcuoglu E, Kisnisci R S. Development of a visio-haptic integrated dental training simulation system. J Dent Educ 2010; 74: 880-891.
De Boer I R, Wesselink P R, Vervoorn J M. The creation of virtual teeth with and without tooth pathology for a virtual learning environment in dental education. Eur J Dent Educ 2013; 17: 191-197.
Ben-Gal G, Weiss E I, Gafni N, Ziv A. Testing manual dexterity using a virtual reality simulator: Reliability and validity. Eur J Dent Educ 2013; 17: 138-142.
Eve E, Koo S, Alshihri A A et al. Performance of Dental Students Versus Prosthodontics Residents on a 3D Immersive Haptic Simulator. J Dent Educ 2014; 78: 630-637.
Suebnukarn S, Chaisombat M, Kongpunwijit T, Rhienmora P. Construct validity and expert benchmarking of the haptic virtual reality dental simulator. J Dent Educ 2014; 78: 1442-1450.
de Boer I R, Wesselink P R, Vervoorn J M. Student performance and appreciation using 3D vs. 2D vision in a virtual learning environment. Eur J Dent Educ 2016; 20: 142-147.
Wang D, Li T, Zhang Y, Hou J. Survey on multisensory feedback virtual reality dental training systems. Eur J Dent Educ 2016; 20: 248-260.
Suebnukarn S, Haddawy P, Rhienmora P, Jittimanee P, Viratket P. Augmented kinematic feedback from haptic virtual reality for dental skill acquisition. J Dent Educ 2010; 74: 1357-1366.
Kikuchi H, Ikeda M, Araki K. Evaluation of a virtual reality simulation system for porcelain fused to metal crown preparation at Tokyo Medical and Dental University. J Dent Educ 2013; 77: 782-792.
Gottlieb R, Lanning S K, Gunsolley J C, Buchanan J A. Faculty impressions of dental students' performance with and without virtual reality simulation. J Dent Educ 2011; 75: 1443-1451.
Gal G B, Weiss E I, Gafni N, Ziv A. Preliminary assessment of faculty and student perception of a haptic virtual reality simulator for training dental manual dexterity. J Dent Educ 2011; 75: 496-504.
Urbankova A, Engebretson S P. The use of haptics to predict preclinic operative dentistry performance and perceptual ability. J Dent Educ 2011; 75: 1548-1557.
Urbankova A, Eber M, Engebretson SP. A complex haptic exercise to predict preclinical operative dentistry performance: a retrospective study. J Dent Educ 2013; 77: 1443-1450.
Steinberg A D, Bashook P G, Drummond J, Ashrafi S, Zefran M. Assessment of faculty perception of content validity of PerioSim, a haptic-3D virtual reality dental training simulator. J Dent Educ 2007; 71: 1574-1582.
Wierinck E R, Puttemans V, Swinnen S P, van Steenberghe D. Expert performance on a virtual reality simulation system. J Dent Educ 2007; 71: 759-766.
Roy E, Bakr M M, George R. The need for virtual reality simulators in dental education: A review. Saudi Dent J 2017; 29: 41-47.
Corrêa C G, Machado M A M, Ranzini E, Tori R, Nunes F L S. Virtual Reality simulator for dental anaesthesia training in the inferior alveolar nerve block. J Appl Oral Sci 2017; 25: 357-366.
Suebnukarn S, Haddawy P, Rhienmora P, Gajananan K. Haptic virtual reality for skill acquisition in endodontics. J Endod 2010; 36: 53-55.
Joseph D, Jehl J P, Maureira P et al. Relative contribution of haptic technology to assessment and training in implantology. Biomed Res Int 2014; 413951. DOI: 10.1155/2014/413951.
Kusumoto N, Sohmura T, Yamada S, Wakabayashi K, Nakamura T, Yatani H. Application of virtual reality force feedback haptic device for oral implant surgery. Clin Oral Implants Res 2006; 17: 708-713.
Suebnukarn S, Hataidechadusadee R, Suwannasri N, Suprasert N, Rhienmora P, Haddawy P. Access cavity preparation training using haptic virtual reality and microcomputed tomography tooth models. Int Endod J 2011; 44: 983-989.
Heiland M, Petersik a, Pflesser B et al. Realistic haptic interaction for computer simulation of dental surgery. Int Congr Ser 2004; 1268: 1226-1229.
Suebnukarn S, Phatthanasathiankul N, Sombatweroje S, Rhienmora P, Haddawy P. Process and outcome measures of expert/novice performance on a haptic virtual reality system. J Dent 2009; 37: 658-665.
Sabalic M, Schoener J D. Virtual Reality-Based Technologies in Dental Medicine: Knowledge, Attitudes and Practice Among Students and Practitioners. Tech Know Learn 2017; 22: 199-207.
Shahriari-Rad A, Cox M, Woolford M. Clinical Skills Acquisition: Rethinking Assessment Using a Virtual Haptic Simulator. Tech Know Learn 2017; 22: 185-197.
San Diego J P, Cox M J, Quinn B F A, Newton J T, Banerjee A, Woolford M. Researching haptics in higher education: The complexity of developing haptics virtual learning systems and evaluating its impact on students' learning. Comput Educ 2012; 59: 156-166.
Cormier J, Pasco D, Syllebranque C, Querrec R. VirTeaSy a haptic simulator for dental education. The 6th International Conference on Virtual Learning. 2011; 61-68.
Păvăloiu IB, Ioaniţescu R, Drăgoi G, Grigorescu S, Sandu S A. Virtual Reality for Education and Training in Dentistry. The 12th International Scientific Conference eLearning and Software for Education Bucharest. 2016; 115-120. DOI: 10.12753/2066-026X-16-052.
Fernández C, Esteban G, Conde-Gonzalez M, Garcia- Peñalvo F J. Improving motivation in a haptic teaching/learning framework. Int J Eng Educ 2016; 32: 553-562.
Bogdan C M, Dinca A, Popovici DM. A Brief Survey of Visuo-Haptic Simulators for Dental Procedures Training. The 6th International Conference on Virtual Learning. 2011; 55-61.
Păvăloiu I B, Sandu S A, Grigorescu S, Dragoi G. Inexpensive Dentistry Training Using Virtual Reality Tools Proceedings of INTED2016 Conference. 2016; 279-285.
Yoshida Y, Yamaguchi S, Kawamoto Y, Noborio H, Murakami S, Sohmura T. Development of a multi-layered virtual tooth model for the haptic dental training system. Dent Mater J 2011; 30: 1-6.
Sofronia R E, Davidescu A, Savii G G. Development of an Efficient Haptic System for Tooth Processing. Adv Mater Res 2012; 463-464: 651-654.
Toosi A, Arbabtafti M, Richardson B L. Virtual Reality Haptic Simulation of Root Canal Therapy. Appl Mech Mater 2014; 666: 388-392.
Yamaguchi S, Yoshida Y, Noborio H, Murakami S, Imazato S. The usefulness of a haptic virtual reality simulator with repetitive training to teach caries removal and periodontal pocket probing skills. Dent Mater J 2013; 32: 847-852.
Wang D, Zhao S, Li T, Zhang Y, Wang X. Preliminary evaluation of a virtual reality dental simulation system on drilling operation. Biomed Mater Eng 2015; 26 (Spec Iss): S747-756.
Kozhevnikov M, Schloerb D W, Blazhenkova O et al. Egocentric versus Allocentric Spatial Ability in Dentistry and Haptic Virtual Reality Training. Appl Cogn Psychol 2013; 27: 373-383.
Umemura H. Effects of haptic information on the perception of dynamic 3D movement. PLoS One 2014; 9: e106633.
Cicciù M, Bramanti E, Signorino F, Cicciù A, Sortino F. Experimental study on strength evaluation applied for teeth extraction: an in vivo study. Open Dent J 2013; 7: 20-26.
Martin N, Mylon P, Lewis R, Carr M J. Evaluation of the effect of medical gloves on dexterity and tactile sensibility using simulated clinical practice tests. Int J Ind Erg 2016; 53: 115-123.
Field J C, Cowpe J G, Walmsley A D. The Graduating European Dentist: A New Undergraduate Curriculum Framework. Eur J Dent Educ 2017; 21 (Spec Iss): 2-10.
Field J, Stone S, Orsini C et al. Curriculum content and assessment of pre-clinical dental skills: A survey of undergraduate dental education in Europe. Eur J Dent Educ 2018; 22: 122-127.
Field J. Pre-Clinical Dental Skills at a Glance. New Jersey, USA: Wiley Blackwell, 2016.
Banerjee A, Watson T F. Pickard's Guide to Minimally Invasive Operative Dentistry. 10th ed. Oxford: OUP, 2015.
Norman G, Dore K, Grierson L. The minimal relationship between simulation fidelity and transfer of learning. Med Educ 2012; 46: 636-647.
Wages R, Grünvogel S M, Grützmacher B. How realistic is realism? Considerations on the aesthetics of computer games. In Rauterberg M (ed) Entertainment Computing - ICEC 2004. pp 216-225. Berlin: Springer, 2004
European Aviation Safety Agency. Certification Specifications for Aeroplane Flight Simulation Training Devices. 2012. Available at https://www.easa.europa.eu/sites/default/files/dfu/CS-FSTD(A)%20Initial%20Issue.pdf (accessed February 2019).
Civil Aviation Authority. PPL (A) requirements. Available at https://www.caa.co.uk/General-aviation/Pilot-licences/EASA-requirements/PPL-SPL-BPL/PPL-(A)-requirements/ (accessed February 2019).
McCloud S. Understanding Comics: The Invisible Art. New York, USA: HarperCollins, 2001.
Mori M. The Uncanny Valley. Energy. Robot Autom Mag 2012; 19: 98-100.
Salas E, Bowers C A, Rhodenizer L. It Is Not How Much You Have but How You Use It: Toward a Rational Use of Simulation to Support Aviation Training. Int J Aviat Psychol 1998; 8: 197-208.
Beilock S L, Bertenthal B I, McCoy A M, Carr T H. Haste does not always make waste: Expertise, direction of attention, and speed versus accuracy in performing sensorimotor skills. Psychon Bull Rev 2004; 11: 373-379.
Hindmarsh J, Hyland L, Banerjee A. Work to make simulation work: "Realism", instructional correction and the body in training. Discourse Stud 2014; 16: 247-269.
Declaration of interests
The research team hold an active R&D collaboration with Haptique & Réalité Virtuelle, Laval, France that is part-funding a PhD studentship for the lead author, Ashley Towers.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Towers, A., Field, J., Stokes, C. et al. A scoping review of the use and application of virtual reality in pre-clinical dental education. Br Dent J 226, 358–366 (2019). https://doi.org/10.1038/s41415-019-0041-0
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-019-0041-0
This article is cited by
-
Enhancing learning experiences in pre-clinical restorative dentistry: the impact of virtual reality haptic simulators
BMC Medical Education (2023)
-
Application of virtual reality in dental implants: a systematic review
BMC Oral Health (2023)
-
How does Dental Students’ expertise influence their clinical performance and Perceived Task load in a virtual Dental Lab?
Journal of Computing in Higher Education (2023)
-
Blended learning and simulation: the future of dental education in a post-COVID era
British Dental Journal (2022)
-
Effectiveness of technology-enhanced teaching and assessment methods of undergraduate preclinical dental skills: a systematic review of randomized controlled clinical trials
BMC Medical Education (2020)
