
Abstract
Background
Optimal postsurgical management of prostate cancer (PCa) patients with nodal metastasis at the time of radical prostatectomy remains unclear. We sought to examine the role of postoperative PSA kinetics and pathologic tumor characteristics in guiding additional hormonal therapy use in pN1 men.
Methods
In total, 297 pN1 PCa patients treated with radical prostatectomy and ePLND between 2002 and 2018 were identified within our prospectively maintained institutional cancer data-registry. Following surgery, these patients were managed with either immediate androgen deprivation therapy (iADT) or observation with deferred ADT (dADT). The former was defined as ADT given within ≤6 months of surgery and the latter as >6 months. The primary outcome was metastasis. Regression-tree analysis was used to stratify patients into novel risk-groups based on post-prostatectomy tumor characteristics and PSA kinetics and the corresponding metastasis risk. Multivariable Cox regression analyses tested the impact of iADT versus observation ± dADT on metastasis, cancer-specific mortality, and overall mortality within each risk-group separately.
Results
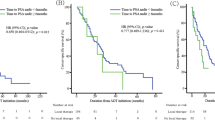
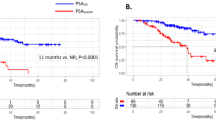
The median follow-up was 6.1 years (IQR 3.2–9.0). Regression-tree analysis stratified patients into 3 novel risk-groups (Harrell’s C-index 0.79) based on PSA-nadir and time to biochemical failure: group 1 (low-risk) included patients with time to biochemical recurrence >6 months (n = 115), while groups 2 and 3 included patients with biochemical failure within ≤6 months with a postoperative PSA-nadir <1.05 ng/mL (group 2 [intermediate-risk], n = 125) or ≥1.05 ng/mL (group 3 [high-risk], n = 57), respectively. No other patient or tumor characteristics were significant for risk stratification. Within each risk-group, the 10-year metastasis-free survival rates with iADT versus observation ± dADT use were: group 1, 100% versus 95.4% (Log-rank p = 0.738), group 2, 80.6% versus 53.5% (Log-rank p = 0.016), and group 3, 41.5% versus 0% (Log-rank p = 0.015), respectively. Adjusted Cox regression analyses confirmed the benefit of iADT utilization in reducing metastasis in group 2 (p = 0.029) and group 3 (p = 0.008) patients, with no benefit for group 1 patients (p = 0.918). Similar results were noted for cancer-specific and overall mortality.
Conclusions
Following radical prostatectomy, early postoperative PSA kinetics may provide valuable information for guiding the timing of ADT initiation—this may reduce over- and undertreatment of pN1 PCa men.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 4 print issues and online access
$259.00 per year
only $64.75 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout





Similar content being viewed by others

Data availability
Data are available to interested parties on request from the corresponding author.
References
Daneshmand S, Quek ML, Stein JP, Lieskovsky G, Cai J, Pinski J, et al. Prognosis of patients with lymph node positive prostate cancer following radical prostatectomy: long-term results. J Urol. 2004;172:2252–5.
Boorjian SA, Thompson RH, Siddiqui S, Bagniewski S, Bergstralh EJ, Karnes RJ, et al. Long-term outcome after radical prostatectomy for patients with lymph node positive prostate cancer in the prostate specific antigen era. J Urol. 2007;178:864–70. discussion 870-861.
Diaz M, Peabody JO, Kapoor V, Sammon J, Rogers CG, Stricker H, et al. Oncologic outcomes at 10 years following robotic radical prostatectomy. Eur Urol. 2015;67:1168–76.
Messing EM, Manola J, Sarosdy M, Wilding G, Crawford ED, Trump D. Immediate hormonal therapy compared with observation after radical prostatectomy and pelvic lymphadenectomy in men with node-positive prostate cancer. N Engl J Med. 1999;341:1781–8.
Messing EM, Manola J, Yao J, Kiernan M, Crawford D, Wilding G, et al. Immediate versus deferred androgen deprivation treatment in patients with node-positive prostate cancer after radical prostatectomy and pelvic lymphadenectomy. Lancet Oncol. 2006;7:472–9.
Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999;281:1591–7.
Wong YN, Freedland S, Egleston B, Hudes G, Schwartz JS, Armstrong K. Role of androgen deprivation therapy for node-positive prostate cancer. J Clin Oncol. 2009;27:100–5.
Touijer KA, Mazzola CR, Sjoberg DD, Scardino PT, Eastham JA. Long-term outcomes of patients with lymph node metastasis treated with radical prostatectomy without adjuvant androgen-deprivation therapy. Eur Urol. 2014;65:20–25.
Kim DK, Koo KC, Abdel Raheem A, Kim KH, Chung BH, Choi YD, et al. Single positive lymph node prostate cancer can be treated surgically without recurrence. PLoS One. 2016;11:e0152391.
Abdollah F, Karnes RJ, Suardi N, Cozzarini C, Gandaglia G, Fossati N, et al. Predicting survival of patients with node-positive prostate cancer following multimodal treatment. Eur Urol. 2014;65:554–62.
VanderWeele DJ, Finney R, Katayama K, Gillard M, Paner G, Imoto S, et al. Genomic heterogeneity within individual prostate cancer foci impacts predictive biomarkers of targeted therapy. Eur Urol Focus. 2019;5:416–24.
Sharifi N, Gulley JL, Dahut WL. Androgen deprivation therapy for prostate cancer. JAMA. 2005;294:238–44.
Keating NL, O’Malley AJ, Smith MR. Diabetes and cardiovascular disease during androgen deprivation therapy for prostate cancer. J Clin Oncol. 2006;24:4448–56.
Abdollah F, Sammon JD, Reznor G, Sood A, Schmid M, Klett DE, et al. Medical androgen deprivation therapy and increased non-cancer mortality in non-metastatic prostate cancer patients aged >/=66 years. Eur J Surg Oncol. 2015;41:1529–39.
Schmid M, Sammon JD, Reznor G, Kapoor V, Speed JM, Abdollah FA, et al. Dose-dependent effect of androgen deprivation therapy for localized prostate cancer on adverse cardiac events. BJU Int. 2016;118:221–9.
Menon M, Tewari A, Peabody J, Team VIP. Vattikuti Institute prostatectomy: technique. J Urol. 2003;169:2289–92.
Ghani KR, Trinh QD, Menon M. Vattikuti Institute Prostatectomy-Technique in 2012. J Endourol / Endourological Soc. 2012;26:1558–65.
Sood A, Jeong W, Peabody JO, Hemal AK, Menon M. Robot-assisted radical prostatectomy: inching toward gold standard. Urol Clin North Am. 2014;41:473–84.
Mattei A, Fuechsel FG, Bhatta Dhar N, Warncke SH, Thalmann GN, Krause T, et al. The template of the primary lymphatic landing sites of the prostate should be revisited: results of a multimodality mapping study. Eur Urol. 2008;53:118–25.
Thompson IM, Valicenti RK, Albertsen P, Davis BJ, Goldenberg SL, Hahn C, et al. Adjuvant and salvage radiotherapy after prostatectomy: AUA/ASTRO Guideline. J Urol. 2013;190:441–9.
Gharzai LA, Jiang R, Wallington D, Jones G, Birer S, Jairath N, et al. Intermediate clinical endpoints for surrogacy in localised prostate cancer: an aggregate meta-analysis. Lancet Oncol. 2021;22:402–10.
Segal MR. Regression trees for censored data. Biometrics. 1988;44:35–47.
Mandrekar JN. Receiver operating characteristic curve in diagnostic test assessment. J Thorac Oncol. 2010;5:1315–6.
Krasnova A, Epstein M, Marchese M, Dickerman BA, Cole AP, Lipsitz SR, et al. Risk of dementia following androgen deprivation therapy for treatment of prostate cancer. Prostate Cancer Prostatic Dis. 2020;23:410–8.
Sanda MG, Dunn RL, Michalski J, Sandler HM, Northouse L, Hembroff L, et al. Quality of life and satisfaction with outcome among prostate-cancer survivors. N. Engl J Med. 2008;358:1250–61.
van Andel G, Kurth KH. The impact of androgen deprivation therapy on health related quality of life in asymptomatic men with lymph node positive prostate cancer. Eur Urol. 2003;44:209–14.
Kang JJ, Reiter RE, Steinberg ML, King CR. Ultrasensitive prostate specific antigen after prostatectomy reliably identifies patients requiring postoperative radiotherapy. J Urol. 2015;193:1532–8.
Grivas N, de Bruin D, Barwari K, van Muilekom E, Tillier C, van Leeuwen PJ, et al. Ultrasensitive prostate-specific antigen level as a predictor of biochemical progression after robot-assisted radical prostatectomy: Towards risk adapted follow-up. J Clin Lab Anal. 2019;33:e22693.
Mottet N, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer-2020 update. part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. 2021;79:243–62.
Cornford P, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. EAU-EANM-ESTRO-ESUR-SIOG guidelines on prostate cancer. Part II-2020 update: treatment of relapsing and metastatic prostate cancer. Eur Urol. 2021;79:263–82.
Abdollah F, Karnes RJ, Suardi N, Cozzarini C, Gandaglia G, Fossati N, et al. Impact of adjuvant radiotherapy on survival of patients with node-positive prostate cancer. J Clin Oncol. 2014;32:3939–47.
Touijer KA, Karnes RJ, Passoni N, Sjoberg DD, Assel M, Fossati N, et al. Survival outcomes of men with lymph node-positive prostate cancer after radical prostatectomy: a comparative analysis of different postoperative management strategies. Eur Urol. 2018;73:890–6.
Tilki D, Chen MH, Wu J, Huland H, Graefen M, Wiegel T, et al. Adjuvant versus early salvage radiation therapy for men at high risk for recurrence following radical prostatectomy for prostate cancer and the risk of death. J Clin Oncol. 2021;39:2284–93.
Wang X, Kattan MW. Cohort studies: design, analysis, and reporting. Chest. 2020;158(1S):S72–S78.
Hoffmann MA, Buchholz HG, Wieler HJ, Miederer M, Rosar F, Fischer N et al. PSA and PSA kinetics thresholds for the presence of (68)Ga-PSMA-11 PET/CT-detectable lesions in patients with biochemical recurrent prostate cancer. Cancers (Basel). 2020;12:398.
Bhargava P, Ravizzini G, Chapin BF, Kundra V. Imaging Biochemical Recurrence After Prostatectomy: Where Are We Headed? AJR Am J Roentgenol. 2020;214:1248–58.
Daly T. Evolution of definitive external beam radiation therapy in the treatment of prostate cancer. World J Urol. 2020;38:565–91.
Magnan S, Zarychanski R, Pilote L, Bernier L, Shemilt M, Vigneault E, et al. Intermittent vs continuous androgen deprivation therapy for prostate cancer: a systematic review and meta-analysis. JAMA Oncol. 2015;1:1261–9.
Author information
Authors and Affiliations
Contributions
Conception and design: AS, FA. Acquisition of data: LTZ, MB, MS. Analysis and interpretation of data: AS, FA. Drafting of manuscript: AS, LTZ, MB, MS, JRA, RG, JOP, CGR, MM, FA. Critical revision of the manuscript for important intellectual content: AS, FA. Statistical analysis: JK. Funding: MM. Administrative, technical, or material support: MM. Other: -.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Sood, A., Zhang, L.T., Keeley, J. et al. Optimizing anti-androgen treatment use among men with pathologic lymph-node positive prostate cancer treated with radical prostatectomy: the importance of postoperative PSA kinetics. Prostate Cancer Prostatic Dis 27, 58–64 (2024). https://doi.org/10.1038/s41391-022-00572-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41391-022-00572-z
