
Abstract
Background
Paediatric inflammatory multisystem syndrome (PIMS) is a rare condition temporally associated with SARS-CoV-2 infection. Using national surveillance data, we compare presenting features and outcomes among children hospitalized with PIMS by SARS-CoV-2 linkage, and identify risk factors for intensive care (ICU).
Methods
Cases were reported to the Canadian Paediatric Surveillance Program by a network of >2800 pediatricians between March 2020 and May 2021. Patients with positive versus negative SARS-CoV-2 linkages were compared, with positive linkage defined as any positive molecular or serologic test or close contact with confirmed COVID-19. ICU risk factors were identified with multivariable modified Poisson regression.
Results
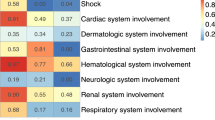
We identified 406 children hospitalized with PIMS, including 49.8% with positive SARS-CoV-2 linkages, 26.1% with negative linkages, and 24.1% with unknown linkages. The median age was 5.4 years (IQR 2.5–9.8), 60% were male, and 83% had no comorbidities. Compared to cases with negative linkages, children with positive linkages experienced more cardiac involvement (58.8% vs. 37.4%; p < 0.001), gastrointestinal symptoms (88.6% vs. 63.2%; p < 0.001), and shock (60.9% vs. 16.0%; p < 0.001). Children aged ≥6 years and those with positive linkages were more likely to require ICU.
Conclusions
Although rare, 30% of PIMS hospitalizations required ICU or respiratory/hemodynamic support, particularly those with positive SARS-CoV-2 linkages.
Impact
-
We describe 406 children hospitalized with paediatric inflammatory multisystem syndrome (PIMS) using nationwide surveillance data, the largest study of PIMS in Canada to date.
-
Our surveillance case definition of PIMS did not require a history of SARS-CoV-2 exposure, and we therefore describe associations of SARS-CoV-2 linkages on clinical features and outcomes of children with PIMS. Children with positive SARS-CoV-2 linkages were older, had more gastrointestinal and cardiac involvement, and hyperinflammatory laboratory picture.
-
Although PIMS is rare, one-third required admission to intensive care, with the greatest risk amongst those aged ≥6 years and those with a SARS-CoV-2 linkage.
Similar content being viewed by others

Introduction
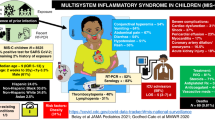
In April 2020, international reports simultaneously began describing children presenting with a rare but serious multisystem inflammatory condition, temporally associated with an antecedent SARS-CoV-2 infection.1,2,3 Clinical features included fever and hyperinflammation, Kawasaki disease (KD)-like presentation, and shock-like state partially overlapping with toxic shock syndrome (TSS).4,5 Several similar but not identical case definitions were developed by different international organizations, including paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS) and multisystem inflammatory syndrome in children (MIS-C).6,7,8 The Canadian Paediatric Surveillance Program (CPSP) is a national voluntary surveillance system jointly operated by the Canadian Paediatric Society and Public Health Agency of Canada that typically gathers information about rare diseases and conditions of high morbidity and mortality despite low frequency.9 In March 2020, it launched a national study of acute SARS-CoV-2 hospitalizations. In May 2020, recognizing the emergence of a post-infectious hyperinflammatory syndrome associated with this novel virus, the CPSP study was rapidly adapted to include surveillance of this syndrome.10,11
Using the reported information, we aimed to (1) study the impact and clinical implications of SARS-CoV-2 linkage on clinical and laboratory features, and outcomes, of hospitalized children presenting with this syndrome, (2) gain a better understanding of risk factors associated with ICU admission, and (3) define the minimum incidence of hospitalizations due to this syndrome and compare it to acute COVID-19.
Methods
Study design and participants
In the absence of a clear and universally accepted case definition in early 2020, and recognizing the need for a rapid launch of surveillance, the CPSP developed a surveillance case definition of suspected paediatric inflammatory multisystem syndrome (PIMS) as best understood at the time, consisting of (1) persistent fever (>38.0 °C for ≥3 days), (2) elevated inflammatory markers (C-reactive protein [CRP], erythrocyte sedimentation rate [ESR], or ferritin), (3) features of KD and/or TSS, and (4) ensuring no alternative etiology to explain the clinical presentation.11 Of note, this case definition was originally intended as a surveillance mechanism that helped assess trends, and was not made for the purpose of clinical diagnosis. In addition, careful consideration was made about the addition of SARS-CoV-2 testing, electing to keep this optional, in the face of limited testing capacity across Canada at the onset of the pandemic, and public health reporting capacity.
Through the CPSP platform, over 2800 pediatricians and pediatric subspecialists were surveyed weekly from March 2020 to May 31, 2021, to report all hospitalized patients <18 years of age, meeting the PIMS surveillance case definition. The full protocol and case report form for the study can be found at: https://www.cpsp.cps.ca/surveillance/study-etude/covid-19. Cases of “PIMS” that were included in the primary analysis were those who met the study definition for PIMS (complete algorithm in Appendix 1). A post hoc definition for MIS-C using the subsequently developed WHO case definition7 was also applied to reported cases. Results of this post hoc analysis are described in Appendix 1. Exclusion criteria included cases that did not meet PIMS criteria upon review, incomplete reports, and duplicates. Duplicates were identified using date of birth and other unique data points. Reporting physicians consented to follow-up for 97.5% of cases to clarify discrepant, missing, or pending data points.
Study definitions
Cases of PIMS were sub-divided into three groups based on their exposure history to the SARS-CoV-2 virus, as follows: (1) “PIMS cases with positive SARS-CoV-2 linkage” indicates a PIMS case with a positive polymerase chain reaction (PCR) test, rapid test, serology, or close contact with microbiologically confirmed SARS-CoV-2, (2) “PIMS cases with negative SARS-CoV-2 linkage” indicates a PIMS case with a negative serologic test with no other positive SARS-CoV-2 test or close contact, and (3) “PIMS cases with unknown SARS-CoV-2 linkage” indicates a PIMS case for whom SARS-CoV-2 testing, including serology, was either not conducted or not reported. Reporting physicians were re-contacted throughout the study to ascertain serology results not available at the time of original case reporting, and cases were reassigned as appropriate.
In all cases where physicians reported a concurrent microbiologically confirmed (i.e., by culture, PCR, or serology) or clinically diagnosed infection, at least one infectious disease specialist (authors S.K.M. or F.K.) and at least one rheumatologist (authors M.P.M. or R.A.B.) systematically reviewed all available clinical information to assess the contribution of the concurrent infection to the patient’s clinical presentation. Cases of disagreement were resolved by consensus of all four physicians. Reports of all radiologic findings were also reviewed and categorized as either abnormal, non-specific, or normal.
To assess laboratory criteria, investigators reporting cases were contacted in October 2020 to report their institutional age- and sex-specific laboratory reference ranges for D-dimer, liver enzymes, and troponin, and reference ranges were available for 75.6% of cases. Where references were not provided, we used references from the Canadian Laboratory Initiative on Pediatric Reference Intervals (CALIPER) study12 while an assumed threshold of 0.5 μg/mL was used for D-dimer. Patient markers above their corresponding institutional or CALIPER reference range were categorized as elevated. Coronary artery abnormalities were defined by lesions of Z-scores ≥2 SD which were further disaggregated into two categories of <2.5 and ≥2.5 SD with body surface area normalized measurements.13 The phases of the COVID-19 pandemic have been defined as “first wave” (March–August 2020) and “second and third” waves combined (September 2020–May 2021).
Statistical analysis
Characteristics were described using medians, interquartile ranges, frequencies, and percentages. Due to CPSP privacy policies, frequencies between one and four were masked as “<5”, and some frequencies were presented as ranges to prevent back-calculation of values <5. To assess differences in SARS-CoV-2 linkage groups, subgroup comparisons were drawn between PIMS cases with positive SARS-CoV-2 linkage and PIMS cases with negative SARS-CoV-2 linkage using χ2 tests, Fisher’s exact tests, and Wilcoxon rank-sum tests. To assess differences in continuous laboratory markers, values were log transformed and analyzed using multiple linear regression, adjusting for age category. The temporal lag between weekly PIMS hospitalizations and weekly Canadian SARS-CoV-2 case counts14 was assessed using Spearman’s rank correlation coefficient. Multivariable Poisson regression with robust standard errors was conducted to identify within-hospital factors associated with ICU admission due to PIMS, and to avoid inflated interpretations of risk from logistic regression. Secondary analyses were conducted to compare patients meeting versus not meeting criteria for PIMS, by pandemic wave, by age category, and by the highest level of care required. A p value <0.05 was considered statistically significant for all analyses. Analyses were conducted using Stata version 17.0.
Finally, we compared the burden of hospitalizations due to PIMS and acute COVID-19 reported to the CPSP as follows. Minimum incidence proportions were calculated by dividing the total and age-specific number of hospitalizations, ICU admissions, and deaths by corresponding population denominators retrieved from Statistics Canada.15 Confidence intervals were calculated by assuming a Poisson distribution, and were not calculated for values <5. The CPSP PIMS and COVID-19 hospitalization studies were conducted using the same reporting methods and period (i.e., up until May 31, 2021) and thus could be directly compared; however, sensitivity analyses excluding cases from Alberta were conducted as acute COVID-19 data were less complete in that province. Hospitalizations with incidentally identified SARS-CoV-2 infection were excluded from these comparisons, as previously described.10
Results
Patient demographics
A total of 493 cases were reported to the CPSP PIMS study, of whom 406 met the study definition of PIMS (Fig. 1) and were hospitalized within the study period. PIMS cases with positive SARS-CoV-2 linkage were reported among 202 children (49.8%). Of these children, 66.8% had a positive close contact, 52.0% had a positive PCR or rapid test, and 48.0% had positive serology (Table 1 and Supplementary Fig. S1). Among PCR-positive patients, 27.6% were positive during the hospital stay, while the remaining patients had a positive test a median of 4.6 weeks (IQR 3.4–5.9) prior to hospitalization. Among children with reported serologies (n = 213), 54.5% had a negative result (n = 116) though ten of these cases had a positive PCR or close contact. Therefore, among all PIMS cases, 26.1% had a negative SARS-CoV-2 linkage (n = 106), while 24.1% had an unknown SARS-CoV-2 linkage (n = 98), with no serology conducted or reported to CPSP.

Flow chart of participants meeting the case definition for PIMS.
The median age among children hospitalized for PIMS was 5.4 years (IQR 2.5–9.8) and more children were male (59.9%; Table 1). On average, cases with a positive SARS-CoV-2 linkage were significantly older (8.1 years, IQR 4.2–11.9) than PIMS cases with a negative SARS-CoV-2 linkage (4.1 years, IQR 1.7–7.7; p < 0.001), as were cases hospitalized in the second and third pandemic waves (6.2 years, IQR 3.1–10.1) versus first (3.8 years, IQR 1.7–8.2; Supplementary Table S1). Most children were previously well with 16.7% having a chronic comorbid condition including asthma (5.9%), neurologic conditions (3.0%), and obesity (3.0%) (Supplementary Table S2). Comparisons between children meeting versus not meeting PIMS study criteria are presented in Supplementary Tables S3 and S4.
Clinical, laboratory, and imaging features
Among all PIMS patients, the median total duration of fever was six days (IQR 5–8; Table 2). In addition to fever, 76.8% of patients had gastrointestinal symptoms (i.e. abdominal pain, diarrhea, and/or vomiting), and more than half had mucocutaneous changes including rash (70.9%), bilateral non-exudative conjunctivitis (70.4%), and changes to the lips/oral cavity (64.5%). Shock/hypotension was reported among 39.2% of patients. Cases with a positive SARS-CoV-2 linkage were more likely to experience gastrointestinal involvement than cases with a negative linkage (88.6% vs. 63.2%; p < 0.001), as well as shock/hypotension (60.9% vs. 16.0%; p < 0.001). Cases with a negative SARS-CoV-2 linkage were more likely to have KD features including changes in lips/oral cavity (75.5% vs. 56.9%; p = 0.001) and peripheral extremities than cases with a positive SARS-CoV-2 linkage (61.3% vs. 45.0%, p = 0.007).
Among all PIMS cases, the median CRP peak was 147 mg/L (IQR 97–221) and median ESR peak was 55 mm/h (IQR 41–78; Table 2). Cases with positive SARS-CoV-2 linkages had significantly higher peak CRP and ferritin values, while having significantly lower sodium, platelet, and albumin nadirs, compared to cases with negative linkages (all p values <0.001). One-third of PIMS cases had abnormal chest radiographs, with common findings including pulmonary opacities, pulmonary edema, peribronchial thickening, and pleural effusion.
Among PIMS patients for whom echocardiograms were conducted (n = 392), 48.7% had cardiac involvement (Table 2). Most common were coronary artery abnormalities (26.5%), among whom the median maximum Z-score was 3.0 (IQR 2.4–3.7) at the time of the report. Decreased heart function was also commonly reported (18.1%), with a median minimum ejection fraction of 45% (IQR 40–50%). Children <1 year old more commonly had coronary artery abnormalities with Z-scores ≥2.5 than older age groups (38.1% vs. 13.2–15.7%; p = 0.001), while children aged 6–17 more commonly had decreased heart function than younger age groups (31.3–32.1% vs. 0.0–7.4%; p < 0.001) (Supplementary Table S5). In those who had serum troponin levels measured, it was elevated in 44.4% with a median peak of 13 ng/L (IQR 9–90). Compared to cases with a negative SARS-CoV-2 linkage, cases with a positive SARS-CoV-2 linkage more commonly experienced decreased heart function (30.7–32.2% vs. 5.1–8.1%; p < 0.001) and elevated troponin (64.1% vs. 20.5%; p < 0.001), but no difference in coronary artery lesions (Table 2).
Treatments and supports
Overall, 28.6% of children required some form of respiratory or hemodynamic support, including more frequently in cases with a positive SARS-CoV-2 linkage than those with a negative linkage (49.0% vs. 9.4%; p < 0.001; Table 3). Respiratory or hemodynamic supports were also more frequently required during second/third waves (34.4% vs. 14.0% in wave one; p < 0.001) (Supplementary Table S1). Supports included vasopressors (20.0% of patients), low-flow oxygen (13.1%), high-flow nasal cannula (5.2%), conventional mechanical ventilation (3.4%), and non-invasive ventilation (3.2%). No patients received extracorporeal membrane oxygenation. Most PIMS patients (94.3%) received intravenous immunoglobulin G (IVIG; with 80.4% receiving one dose and 13.9% receiving two or more doses), and 67.0% received systemic corticosteroids. Together, 65.8% received both IVIG and steroids, 28.6% received IVIG only, 1.2% received corticosteroids only, and 4.4% received neither IVIG nor steroids, while 5.9% of patients received a biologic agent. Most patients received aspirin (90.1%) and 11.3% received either prophylactic or therapeutic anticoagulation. Forty-five patients (11.1%) had a concurrent infection determined to have contributed to clinical findings, though PIMS remained the primary cause of hospitalization (Supplementary Table S6), and the presentation of these patients versus all other patients is presented in Supplementary Table S7.
There were 127 (31.3%) PIMS patients admitted to the ICU, among whom the median ICU length of stay was three days (IQR 2–4). No deaths due to PIMS occurred (Table 1). Children with a positive SARS-CoV-2 linkage were 2.7 times (95% CI 1.6–4.5) more likely to be admitted to ICU than children with a negative linkage (Table 4). Compared to children aged 1–5 years, older age was also associated with a greater risk of ICU admission for ages 6–12 years (aRR 2.5 [1.7–3.6]) and ages 13–17 years (aRR 2.3 [1.5–3.5]). We found no significant association with age under one year, sex, or comorbidities, and higher risk among the second and third waves in crude analyses was attenuated in multivariable analysis. When comparing clinical features among children by the level of care required (i.e., ICU vs. inpatient ward; Supplementary Table S8), children admitted to ICU were more likely to experience gastrointestinal involvement (92.2% vs. 70.5%; p < 0.001), and shock/hypotension (83.5% vs. 19%; p < 0.001).
Time series and epidemiology
Accounting for <18-year population denominators, the CPSP reported cases corresponding to a minimum study period incidence of 5.6 PIMS hospitalizations (95% CI 5.1–6.2) and 2.8 PIMS hospitalizations with a positive SARS-CoV-2 link (95% CI 2.4–3.2) per 100,000 population (Supplementary Table S9). PIMS hospitalizations peaked nationally first in May 2020 and again in January 2021 and were most strongly correlated with a 5-week lag behind Canadian SARS-CoV-2 case counts (Spearman’s rho 0.68) (Fig. 2). Most PIMS hospitalizations occurred in Ontario (39.9%), Quebec (36.5%), and Alberta (12.6%). A higher proportion of cases hospitalized in the second/third waves had SARS-CoV-2 linkages (61.6%) compared to the first wave (18.8%, p < 0.001; Supplementary Table S1).

a Monthly PIMS hospitalizations by region (left). It includes 406 hospitalizations from across Canada (CAN), including 162 from Ontario (ON), 148 from Quebec (QUE), 83 from Western Canada (WEST; 51 from Alberta, 15 from British Columbia, and 17 from Manitoba or Saskatchewan); 13 from Atlantic Canada (ATL; including New Brunswick, Newfoundland and Labrador, Nova Scotia, or Prince Edward Island); and zero from Territories (TER; including Northwest Territories, Nunavut, Yukon). b Weekly PIMS hospitalizations and SARS-CoV-2 cases across Canada (all ages and <20 years separately). PIMS data represent the 3-week moving average of weekly hospitalizations. Week zero is defined as the week beginning March 2, 2020; January 1, 2021, occurs in week 43. SARS-CoV-2 cases were extracted from https://health-infobase.canada.ca/covid-19/epidemiological-summary-covid-19-cases.html, and reflect the date of illness onset.
Discussion
Leveraging established national public health surveillance infrastructure using physician-reported data, this study describes 406 hospitalized children with PIMS across Canada from May 2020 to May 2021. By comparing PIMS cases with positive and negative SARS-CoV-2 linkages, we were able to study the impact of SARS-CoV-2 linkage on clinical and laboratory features, and outcomes in hospitalized children presenting with presumed post-infectious hyperinflammatory syndrome during the first three waves of the COVID-19 pandemic. It is important to note that as waves of SARS-CoV-2 continue to infect increasingly large proportions of populations around the world and pediatric vaccination increases, the utility of current serologic tests in the diagnosis of post-SARS-CoV-2 conditions and clinical decision making will lessen.
Compared to children with a negative SARS-CoV-2 linkage, children with a positive SARS-CoV-2 linkage were older, had more severe gastrointestinal and cardiac involvement (decreased heart function, shock), a more hyperinflammatory laboratory picture (higher CRP, ferritin, and troponin peak levels with coagulation dysfunction), higher rates of ICU admission, requirements of respiratory/hemodynamic support, and were more likely to receive corticosteroids and antibiotics. Our study findings for this group are in line with descriptive case series describing clinical signs and symptoms of PIMS and MIS-C regardless of case definition, yet most comparisons are made with COVID-19 patients and/or pre-pandemic KD.16,17 The number of PIMS hospitalizations and ICU admissions was also consistent with a Canadian national case series describing high-level MIS-C outcomes.18
Conversely, children with a negative SARS-CoV-2 linkage were younger, experienced more KD features including changes in lips/oral cavity and peripheral extremities, and a higher platelet peak after admission. While the younger age and thrombocytosis seen in this group may be consistent with a KD phenotype, there are several features that suggest at least some of these cases are not entirely typical of pre-pandemic KD. The incidence of shock (16%) in this group is more than twice that reported in KD shock syndrome (7%).13 Secondly, approximately 10–20% of patients with KD have recalcitrant fever after their first IVIG infusion, also known as being “IVIG resistant.”13 In our study, more than half of these cases (54.7%) were treated with corticosteroids, with 15.1% receiving ≥2 IVIG infusions. While the order in which immunomodulatory agents were given (i.e., concurrently or sequentially) was not captured in this study, these combined treatments surpass the rates of recalcitrant KD.13 Of note, the American College of Rheumatology task force first recommended that IVIG and glucocorticoids could be used alone or in combination for the treatment of this syndrome in July 2020 (Version 1), and by April 2021 (Version 2), recommended upfront steroids, when early data emerged showing the high rate of IVIG resistance during the pandemic. This may partly explain higher steroid use in those patients.19,20 Therefore, although this group did not have evidence of SARS-CoV-2 linkage, many still experienced the severe end of the disease spectrum. While SARS-CoV-2 linkage is an important epidemiologic feature, requiring it in a case definition may be overly specific and result in missing certain cases. A recent study showed that some individuals do not develop a serologic response because of pre-existing memory T-cell responses, with cross-protective potential against SARS-CoV-2.21
Infectious triggers are known to be associated with inflammation syndromes in children; however, it remains unclear whether MIS-C is a new syndrome consisting of SARS-CoV-2 immune-mediated fever with cytokine release, SARS-CoV-2 triggered KD, SARS-CoV-2 triggered shock, or some combination thereof. In our analysis, MIS-C and “PIMS with positive SARS-CoV-2 linkages“ have a near 1:1 overlap. Specifically, 198 cases met the criteria for both labels, 11 cases met the criteria for MIS-C but not PIMS with positive linkages, and <5 met the criteria for PIMS with positive linkages but not MIS-C (due to small differences in case definitions globally). In addition, some children categorized as “PIMS with negative SARS-CoV-2 linkages” (as well as some with unknown linkages), fit the American Heart Association definition of KD, with the stratification of PIMS cases by positive vs. negative SARS-CoV-2 linkages acting as a proxy comparison for MIS-C vs. KD in this study. The classification terminology debate is compounded by the fact that MIS-C, PIMS, and KD are “syndromes” and not “diseases” and do not have unique diagnostic tests. Additional study is needed to better understand the post-infectious hyperinflammatory syndrome spectrum and the heterogeneous range of phenotypes described, and relationship with the infectious trigger.
Thirty percent of PIMS cases required ICU admission, emphasizing the importance of identifying potential risk factors for ICU admission that might inform prognosis and early intervention. Our study showed an association with older age groups (6–12 and 13–17 years) and SARS-CoV-2 linkage but no association with sex or underlying comorbidities. Furthermore, the identified risk factors above are consistent with trends seen in previous literature.22 It remains unclear why there may be a possible predilection towards older children, though some theories related to age-based immune response and susceptibility have been proposed.5,16,20,23,24 Though confounded by the PIMS-associated age distribution, the reported numbers of specific comorbid conditions in our study including asthma (5.9%), obesity (3.0%), and neurologic/neurodevelopmental conditions (3.0%) fall within reported prevalence in the general pediatric population.25,26 Five children (1.2%) had a prior history of KD, which is in keeping with the reported percentage of recurrence of KD pre-pandemic that could vary among different ethnicities.13
During the study period, the minimum national incidence of PIMS hospitalization was 5.6 per 100,000 population, and for ICU admission was 1.8 per 100,000 population (2.8 and 1.4 per 100,000 population for cases with positive SARS-CoV-2 linkages, respectively) which are comparable to that of acute COVID-19 disease ascertained in the same CPSP study (4.6 hospitalizations and 0.8 ICU admissions per 100,000 population, excluding incidental SARS-CoV-2).10 The incidence of PIMS hospitalizations with positive SARS-CoV-2 linkages was highest in those aged 1–5 years (3.3 per 100,000 population) and those aged 6–12 years (3.1 per 100,000 population). The estimate of the worldwide incidence of this syndrome is still unknown. Although PIMS is a rare complication of SARS-CoV-2 infection, these figures underscore an important consequence of the COVID-19 pandemic in the pediatric population. Reassuringly, observational studies have shown overall low mortality in PIMS with relatively rapid recovery of organ dysfunction with appropriate, timely treatment, though longitudinal follow-up is limited.27,28 It also supports the importance of vaccination of eligible children as early evidence supports this to be effective at preventing PIMS in adolescents.29 As new variants of SARS-CoV-2 emerge, there is evidence that MIS-C occurs less frequently after infection with Omicron variants.30,31 These studies have also found MIS-C to be less severe during Omicron waves, requiring shorter hospital and ICU stays as well as less vasopressor use.31,32 Ongoing monitoring for incidence following infection from future variants will be essential as risk may continue to change.
While our study cannot establish causality, the findings showed that peaks of PIMS hospitalizations correlated with a temporal lag of five weeks after peaks in all Canadian SARS-CoV-2 infections, similarly reported in other studies ranging from 2 to 6 weeks.2,16 Higher peaks were seen in three Canadian jurisdictions (Ontario, Quebec, and Alberta) with the highest numbers of acute SARS-CoV-2 infections. This supports a possible post-infectious immune dysregulation phenomenon.33 The higher numbers of cases witnessed in second/third waves vs. first (Supplementary Table S1) may partly reflect the real-time learning curve of health care providers in better identifying cases. This also highlights the success of this voluntary reporting system.
This study has a few limitations. The voluntary nature of CPSP reporting means that not all cases may have been reported. Second, the online PIMS case report form was developed soon after the first identification of the clinical entity; therefore, data on other important clinical or laboratory markers such as NT-proBNP and lymphopenia were not included in the study. In addition, several indicators were ascertained by physician report, including population group of the child and cardiac findings such as myocarditis and shock (which were not based on pre-defined diagnostic criteria). Another limitation of this study is that it is difficult to determine if laboratory tests were done before or after the administration of immune-modulating treatments like IVIG which may impact some laboratory values. In addition, at the time of this study, there were no standardized treatment protocols across Canada; thus, treatment and timing of treatment may have differed, which may have affected clinical outcomes. Lastly, this study does not capture data on the more recent variants of COVID-19, namely Delta and Omicron, since the enrollment period concluded in May 2021.
In conclusion, while PIMS is rare, it remains an important consequence of SARS-CoV-2 infection in children in which almost one in three hospitalized children required ICU admission and respiratory/hemodynamic support. At-risk groups for ICU admission include children 6 years and older and those with positive SARS-CoV-2 linkages. These results provide baseline data prior to the implementation of SARS-CoV-2 vaccination for children and can be used to monitor changes to the epidemiology of PIMS as vaccination in different age groups is introduced. We demonstrate that in the milieu of widespread SARS-CoV-2 transmission, post-infectious hyperinflammatory phenotypes observed are more severe regardless of recognized SARS-CoV-2 exposure compared to pre-pandemic KD. Collectively, these findings help both better define the epidemiology of this condition in Canada and serve to inform clinical practice and public health responses to PIMS.
Data availability
De-identified data that underlie the results reported in this article (text, tables, figures, and appendices) and that abide by the privacy rules of the Canadian Paediatric Surveillance Program and the Public Health Agency of Canada can be made available to investigators whose secondary data analysis study protocol has been approved by an independent research ethics board.
References
Riphagen, S., Gomez, X., Gonzalez-Martinez, C., Wilkinson, N. & Theocharis, P. Hyperinflammatory shock in children during COVID-19 pandemic. Lancet 395, 1607–1608 (2020).
Feldstein, L. R. et al. Multisystem inflammatory syndrome in U.S. children and adolescents. N. Engl. J. Med. 383, 334–346 (2020).
Whittaker, E. et al. Clinical characteristics of 58 children with a pediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2. JAMA 324, 259–269 (2020).
Tam, H., El Tal, T., Go, E. & Yeung, R. S. M. Pediatric inflammatory multisystem syndrome temporally associated with COVID-19: a spectrum of diseases with many names. CMAJ 192, E1093–E1096 (2020).
Radia, T. et al. Multi-system inflammatory syndrome in children & adolescents (MIS-C): a systematic review of clinical features and presentation. Paediatr. Respir. Rev. 38, 51–57 (2021).
The Royal College of Paediatrics and Child Health. Guidance: Paediatric Multisystem Inflammatory Syndrome Temporally Associated with COVID-19; https://www.rcpch.ac.uk/sites/default/files/2020-05/COVID-19-Paediatric-multisystem-%20inflammatory%20syndrome-20200501.pdf.
World Health Organization. Multisystem Inflammatory Syndrome in Children and Adolescents with COVID-19: Scientific Brief; https://www.who.int/publications/i/item/multisystem-inflammatory-syndrome-in-children-and-adolescents-with-covid-19 (2020).
Centers for Disease Control and Prevention, Emergency Preparedness and Response 8. Multisystem Inflammatory Syndrome in Children (MIS-C) Associated with Coronavirus Disease 2019 (COVID-19); https://emergency.cdc.gov/han/2020/han00432.asp (2020).
Canadian Paediatric Surveillance Program. About the CPSP; https://cpsp.cps.ca/about-apropos.
Drouin, O. et al. Characteristics of children admitted to hospital with acute SARS-CoV-2 infection in Canada in 2020. CMAJ 193, E1483–E1493 (2021).
Canadian Paediatric Surveillance Program. COVID-19. www.cpsp.cps.ca/surveillance/study-etude/covid-19.
Adeli, K., Higgins, V., Trajcevski, K. & White-Al Habeeb, N. The Canadian laboratory initiative on pediatric reference intervals: a CALIPER white paper. Crit. Rev. Clin. Lab Sci. 54, 358–413 (2017).
McCrindle, B. W. et al. Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation 135, e927–e999 (2017).
Statistics Canada. Preliminary dataset on confirmed cases of COVID-19. Public Health Agency of Canada; https://doi.org/10.25318/132600032020001-ENG (2020)
Statistics Canada. Population Estimates on July 1st, by Age and Sex; https://doi.org/10.25318/1710000501-ENG (2021)
Feldstein, L. R. et al. Characteristics and outcomes of US children and adolescents with multisystem inflammatory syndrome in children (MIS-C) compared with severe acute COVID-19. JAMA 325, 1074–1087 (2021).
Cherqaoui, B., Koné-Paut, I., Yager, H., Bourgeois, F. L. & Piram, M. Delineating phenotypes of Kawasaki disease and SARS-CoV-2-related inflammatory multisystem syndrome: a French study and literature review. Rheumatology (Oxford) 60, 4530–4537 (2021).
Laverty, M. et al. Multisystem inflammatory syndrome in children in Canada. Can. Commun. Dis. Rep. 47, 461–465 (2021).
Henderson, L. A. et al. American College of Rheumatology Clinical Guidance for multisystem inflammatory syndrome in children associated with SARS-CoV-2 and hyperinflammation in pediatric COVID-19: version 1. Arthritis Rheumatol. 72, 1791–1805 (2020).
Henderson, L. A. et al. American College of Rheumatology Clinical Guidance for multisystem inflammatory syndrome in children associated with SARS-CoV-2 and hyperinflammation in pediatric COVID-19: version 2. Arthritis Rheumatol. 73, e13–e29 (2021).
Swadling, L. et al. Pre-existing polymerase-specific T cells expand in abortive seronegative SARS-CoV-2. Nature 601, 110–117 (2022).
Abrams, J. Y. et al. Factors linked to severe outcomes in multisystem inflammatory syndrome in children (MIS-C) in the USA: a retrospective surveillance study. Lancet Child Adolesc. Health 5, 323–331 (2021).
Yurttutan, S., Güllü, U. U., İpek, S., Gungor, S. & Yurttutan, N. Clinical and laboratory findings of multisystem inflammatory syndrome in children (MIS-C) below age 1. Clin. Rheumatol. 40, 2515–2516 (2021).
Brodin, P. SARS-CoV-2 infections in children: understanding diverse outcomes. Immunity 55, 201–209 (2022).
Public Health Agency of Canada. Asthma in Canada – Data Blog; https://health-infobase.canada.ca/datalab/asthma-blog.html (2018).
Public Health Agency of Canada. Childhood Obesity; https://www.canada.ca/en/public-health/services/childhood-obesity/childhood-obesity.html (2016).
Mahmoud, S. et al. Treatment of MIS-C in children and adolescents. Curr. Pediatr. Rep. 10, 1–10 (2022).
Matsubara, D. et al. Longitudinal assessment of cardiac outcomes of multisystem inflammatory syndrome in children associated with COVID-19 infections. J. Am. Heart Assoc. 11, e023251 (2022).
Zambrano, L. D. et al. Effectiveness of BNT162b2 (Pfizer-BioNTech) mRNA vaccination against multisystem inflammatory syndrome in children among persons aged 12-18 years – United States, July-December 2021. MMWR Morb. Mortal. Wkly Rep. 71, 52–58 (2022).
Holm, M. et al. Risk and phenotype of multisystem inflammatory syndrome in vaccinated and unvaccinated Danish children before and during the Omicron wave. JAMA Pediatr. 176, 821–823. https://doi.org/10.1001/jamapediatrics.2022.2206 (2022)
Levy, N. et al. Severity and incidence of multisystem inflammatory syndrome in children during 3 SARS-CoV-2 pandemic waves in Israel. JAMA 327, 2452–2454. https://doi.org/10.1001/jama.2022.8025 (2022)
Kenney, P. O., Chang, A. J., Krabill, L. & Hicar, M. D. Decreased clinical severity of pediatric acute COVID-19 and MIS-C and increase of incidental cases during the Omicron wave in comparison to the Delta wave. Viruses 15, 180 (2023).
Henderson, L. A. & Yeung, R. S. M. MIS-C: early lessons from immune profiling. Nat. Rev. Rheumatol. 17, 75–76 (2021).
Acknowledgements
The authors wish to thank the pediatricians, pediatric subspecialists, and health professionals who voluntarily responded to CPSP surveys. We also wish to thank the members and leadership of the Paediatric Inpatient Research Network (PIRN) for the cases reported and their dedication to the CPSP. We are enormously grateful to the staff of the CPSP for their dedication, diligence, and commitment to this study. Lastly, the authors also wish to thank members of the CPSP Scientific Steering Committee who serve as stewards of the program.
Funding
Financial support for the Canadian Paediatric Surveillance Program (CPSP) was received from the Public Health Agency of Canada (PHAC). The CPSP is governed by an independent Scientific Steering Committee (SSC) comprised of individuals from both CPS and PHAC (the funder). Members of the SSC reviewed and approved the study design. Individuals from PHAC, CPS, and the SSC participated in the interpretation of the data. The final report was provided to PHAC for review; however, the study team maintained scientific independence and the authors were under no obligation to accept or incorporate changes to the manuscript.
Author information
Authors and Affiliations
Contributions
The study was conceived by T.E.T., M.-P.M., S.K.M., D.S.F., E.H., R.S., and R.S.M.Y.; T.E.T. wrote the first draft of the manuscript, and D.S.F. conducted the statistical analysis. All authors had access to the data, and D.S.F., C.M.H., M.L., M.K., and S.K.M. accessed and verified the data underlying the study. All authors contributed to data collection, reviewed the study results and manuscript, and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
M.-P.M. has received consulting fees from Sobin and AbbVie and payment for expert testimony from the Canadian Medical Protective Association. S.K.M. has received honoraria for lectures from GlaxoSmithKline, was a member of ad hoc advisory boards for Pfizer Canada and Sanofi Pasteur, and is an investigator on an investigator-led grant from Pfizer. R.A.B. has received honoraria and participated in advisory boards with SOBI, Roche, Amgen, and AbbVie. K.B. served as Past President of the Community Paediatrics Section of the Canadian Paediatric Society and has received royalties from Brush Education. K.C. is Chair of the Acute Care Committee of the Canadian Paediatric Society and is past president of the Emergency Medicine Section of the Canadian Paediatric Society. E.J.D. is Chair of the Scientific Research Committee and a director of Epilepsy Canada. She is also a member of Partners Against Mortality in Epilepsy and the advisory boards of Cardiol, Pendopharm and Stoke Therapeutics. C.F. is Chair of the Scientific Steering Committee for the Canadian Paediatric Surveillance Program, former Chair of the Specialty Committee in Pediatrics of the Royal College of Physicians and Surgeons of Canada, former President of the Canadian Paediatric Society, and member of the Executive as Secretary of the Canadian Critical Care Society. She has received reimbursement for travel expenses from Canadian Paediatric Society and the Royal College of Physicians and Surgeons of Canada. She has also received an honorarium for a presentation at a continuing education conference from the Université de Sherbrooke. S.F. is the President of the Association of Medical Microbiology and Infectious Disease Canada and has received consulting fees from Toronto Metropolitan University. F.K. has received honoraria for presentations given to the Association des Pédiatres du Québec and receives CMV testing kits from Altona Diagnostics. R.M.L. has received honoraria for serving as a consultant to Sobi, Novartis, Sanofi, and Eli Lilly, as chair for data monitoring committees for Eli Lilly and Novartis, and from the Canadian Rheumatology Association. C.M.H. is the Director of Children’s Mental Health of Ontario, and the Director of medical affairs for the Canadian Paediatric Society and the Canadian Paediatric Surveillance Program. J.P. reports grants from MedImmune, grants and personal fees from Merck and AbbVie, and personal fees from AstraZeneca, all outside the submitted work. R.P. is a consultant for Verity Pharmaceuticals. M.S. is supported via salary awards from the BC Children’s Hospital Foundation and the Michael Smith Foundation for Health Researc and has been an investigator on projects funded by GlaxoSmithKline, Merck, Moderna, Pfizer, Sanofi Pasteur, Seqirus, Symvivo and VBI Vaccines. All funds have been paid to his institute, and he has not received any personal payments. M.L.S. is an employee of the Public Health Agency of Canada. R.S. has received honoraria and served on an advisory board and as a consultant with Novartis, honoraria from Canadian Rheumatology Association, is a board member for Rheumatology for All, and her institution receives funding from Bristol Myers Squibb for a patient registry for which she is PO. E.H. has participated in advisory board meetings of CSL-Behring and Takeda, data safety monitoring boards of Rocket Pharmaceutical and Jasper Therapeutics, and has a patent application with the biotech Immugenia and the biotech Immune Biosolutions. All other authors report no declaration of interests.
Ethics approval and consent to participate
Research ethics approval was obtained at Health Canada-PHAC (REB #2020-002P), The Hospital for Sick Children (REB #1000070001), the Centre Hospitalier Universitaire Sainte-Justine (IRB #MP-21-2021-2901), and at individual sites as required by local policies. In Quebec, the study was conducted as a multicenter study with clinical data collected by study co-investigators, and serologies from CHUSJ done for research purposes (REB #3195) prior to the introduction of clinical testing were also included. The CPSP operates under legal authority derived from Section 4 of the Department of Health Act and Section 3 of the Public Health Agency of Canada Act. As a national surveillance program operating under these authorities (with the exception of the Province of Quebec), the CPSP does not collect any individual data elements deemed to be unique identifiers, and physicians who report cases to the CPSP are not required to obtain informed consent from patients. Participating physicians from Quebec obtain Research Ethics Board approvals from their institution in order to report clinical data to the Program. This is consistent with the Canadian Medical Association and Tri-Council Policy Statements, which allow for the collection of non-nominal and non-identifiable information for conditions under surveillance. All CPSP participants are pediatricians and pediatric subspecialists who voluntarily report cases, based on information already included in the medical chart. If any data elements requested on the questionnaire are not readily available in the chart, the physician indicates that they are unknown and do not contact the families to seek these specific details. In some cases, individual reporting physicians may provide consent to the CPSP to contact them (i.e., the reporting physician) directly to clarify cases of discrepant, missing, or unclear data. A willingness to be contacted by the CPSP is not a condition of participation in the program. Only the CPSP staff who have security clearance are aware of the name of the reporting physician; the study team does not receive this information in order to further protect patient confidentiality.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
El Tal, T., Morin, MP., Morris, S.K. et al. Paediatric inflammatory multisystem syndrome in Canada: population-based surveillance and role of SARS-CoV-2 linkage. Pediatr Res 94, 1744–1753 (2023). https://doi.org/10.1038/s41390-023-02668-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-023-02668-1
