
Abstract
Background
We assessed associations between maternal stress, social support, and child resiliency during the COVID-19 pandemic in relation to changes in anxiety and depression symptoms in children in Mexico City.
Methods
Participants included 464 mother-child pairs from a longitudinal birth cohort in Mexico City. At ages 8–11 (pre-COVID, 2018–2019) and 9–12 (during COVID, May–Nov 2020) years, depressive symptoms were assessed using the child and parent-reported Children’s Depressive Inventory. Anxiety symptoms were assessed using the child-reported Revised Manifest Anxiety Scale. Linear regression models were used to estimate associations between maternal stress, social support, and resiliency in relation to changes in depressive and anxiety symptoms. We additionally assessed outcomes using clinically relevant cut-points. Models were adjusted for child age and sex and maternal socioeconomic status and age.
Results
Higher continuous maternal stress levels during the COVID-19 pandemic were associated with increases in depressive symptoms (β: 0.72; 95% CI: 0.12, 1.31), and higher odds of clinically relevant depressive and anxiety symptoms in the children.
Conclusions
Maternal stress during the pandemic may increase mental health symptoms in pre-adolescent children. Additional studies are needed that examine the long-term pandemic-related impacts on mental health throughout the adolescent years.
Impact
-
In this longitudinal cohort study of children in Mexico City, we observed that depressive symptoms were higher from before to during the pandemic.
-
Maternal stress surrounding the pandemic may increase mental health symptoms in pre-adolescent children.
-
Child resiliency may help to protect against pandemic-related stressors.
Similar content being viewed by others

Introduction
As the coronavirus disease 2019 (COVID-19) pandemic spread across the globe, several population-level interventions went into place. In Mexico City, the first confirmed case was in February 2020, with school closures and social distancing measures following shortly after in March. Though effective in reducing transmission, these preventative measures have contributed to social isolation and loneliness among several populations,1 leading to the new onset of or potentially further exacerbating mental health symptoms.2 The pandemic has posed a particular threat to the mental health of children, adolescents, and their caregivers.3,4 Of the existing cross-sectional and longitudinal studies on the mental health impacts of COVID-19-related stressors in children, several have found increases in depressive and anxiety symptoms.5,6,7 Previous studies have additionally shown associations with maternal stress and child mental health;8,9 however, the majority have focused on prenatal stress and long-term impacts. Maternal stress may have a heightened short-term impact during the pandemic due to home confinement and social isolation measures. The impact of protective factors such as social support additionally remains poorly understood. This is a major research gap as maternal social isolation has been linked to adverse health outcomes in the child including depression.3,10
The impact of pandemic-related stressors on child mental health remains even less studied in low and middle-income countries, such as Mexico. This is a critical gap given that up to 40% of adolescents in Mexico City may have a mental health condition.11 A recent study in Brazil found the impacts of the pandemic on anxiety and depressive symptoms in children with those from vulnerable populations most impacted.12 One recent study looked at the well-being of Mexican and Chilean adolescents during the pandemic and found an overall higher prevalence of languishing in adolescents.13
We take a socio-ecological approach to assessing pandemic-related impacts on mental health symptoms in children.14 This framework considers that it is a complex interplay between the individual, family, community, and society. The main objective of our study was to assess associations between maternal stress and social support and changes in anxiety and depression symptoms in children from a birth cohort in Mexico City from before to during the pandemic. We additionally aimed to assess sex differences in the associations. We hypothesized that (a) child mental health symptoms would increase, (b) maternal stress would be related to a higher number of symptoms, while maternal social support would be related to fewer, and (c) given differences in mental health symptoms by sex,15 that these associations would differ by child sex.
Methods
Study population
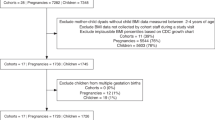
We used data from the Programming Research in Obesity, Growth, Environment and Social Stressors (PROGRESS) birth cohort in Mexico. Pregnant women were recruited between 2007 and 2011 at 12–24 weeks’ gestation in primary care clinics of the Mexican Social Security Institute. Women were eligible if they were ≥18 years, planned to live in Mexico City, <20 weeks gestation, had no medical history of heart or kidney disease, and did not consume alcohol daily.16 Of the 948 women who delivered a live birth and agreed to follow-up, 500 returned for both the pre- and post-COVID visit, and 464 of those women had complete data (Supplemental Fig. 1). Participant characteristics did not differ for those included and those in the original sample (Supplemental Table 1).
Protocols were approved by the institutional review boards at the Icahn School of Medicine at Mount Sinai, Harvard School of Public Health, and the Mexican National Institute of Public Health. All women provided informed consent and children provided assent.
Outcome measures
Mothers and children completed the pre-pandemic in-person assessments between 2018 and 2019. Mother–child pairs completed the telephone-based assessments during COVID between May and November 2020. Both pre- and post-pandemic assessments were administered in a standardized format by trained psychologists. Symptoms of anxiety and depression were assessed in children before and during the pandemic using the Spanish versions of the Children’s Depression Inventory (CDI-2) and Revised Children’s Manifest Anxiety Scale (RCMAS-2). Though both the CDI17 and RCMAS18 have shown high validity, these screening tools do not diagnose depression or anxiety but instead provide an indication of the severity of symptoms.
Children’s Depression Inventory
The CDI is a validated17 instrument developed to evaluate symptoms of depression in 7–17 year olds.19 The short form of the children’s version of the CDI-2 (CDI-C) contains 12 items; the parent-report version (CDI-P) contains 17 items. For both versions, items were summed to create a total raw score. Raw scores on the CDI-P ranged from 0 to 37 (Cronbach’s alpha = 0.8 for pre-COVID, 0.8 for COVID). Raw scores on the CDI-C ranged from 0 to 21 (Cronbach’s alpha = 0.6 for pre-COVID, 0.6 for COVID). Raw scores were converted to standardized T-scores based on normative samples.19 We analyzed T-scores as continuous measures, with higher scores indicating more severe symptoms. We additionally dichotomized scores using cut-off values recommended by the manual (≥65).
Revised Children’s Manifest Anxiety Scale
The RCMAS-2 is a validated18 self-report instrument developed to measure the nature and degree of anxiety in 6–19 year olds. The RCMAS-2 short form has 12 items rated as yes/no. Higher scores indicate greater symptoms. Individual items on the RCMAS-2 were summed to create a total raw score ranging from 0 to 10 (Cronbach’s alpha = 0.6 for pre-COVID and 0.70 for the COVID assessment). Raw total anxiety scores were converted to standardized T-scores based on normative samples. We analyzed scores as continuous and also dichotomized scores based on the manual (≥60).
Exposure measures
Maternal negative life events (NLEs)
Maternal stress was measured before and during the pandemic using data from the Spanish version of the validated20 Crisis in Family Systems (CRISYS)21 questionnaire. This 64-item questionnaire assesses the occurrence of stressful life events across several domains during the prior 6 months. Mothers rated the life event as positive, negative, or neutral. Studies demonstrate increased vulnerability when experiencing events across multiple domains.22 Therefore, the number of domains with one or more events endorsed as negative were summed to create a NLE domain score (range 0–11), with higher scores indicating greater stress, as done in prior research.23,24
Social support
Maternal social support from family, neighbors, and friends was assessed before and during the pandemic using the Spanish version of the Social Support Network (SSN) Scale. The SSN scale was previously validated in Mexican populations.25 Mothers rated their degree of agreement with each item on the SSN based on 4 levels scored from 1 (strongly disagree) to 4 (strongly agree). Social support scores ranged from 7–20 in our population, with higher scores indicating greater support. The Cronbach alpha was 0.89 for both the pre-pandemic and pandemic SSN scale.
Resiliency scale
Children’s resiliency was assessed using the Resiliency scale from the Behavioral Assessment System for Children (BASC-2).26 The Spanish version of the BASC-2 was administered to mothers prior to COVID—this assessment was not administered during the pandemic, and thus we only assessed impacts with this measure in sensitivity analyses. The Resiliency scale includes 10 items and measures the ability of the child to overcome stress and adversity. Raw scores were converted to standardized T-scores based on normative samples.26
Covariates
Covariate information was obtained from standardized questionnaires. The program DAGitty was used to construct our directed acyclic graph in order to identify the minimally sufficient adjustment set (Supplemental Fig. 2).27 The final adjustment set included the child’s age (before and during COVID), the child’s sex, maternal age (before and during COVID), and maternal SES prior to COVID. Thirteen variables derived from questionnaire results were used to classify study participants into six levels based on the SES index.28 We further collapsed this into lower, medium, and higher SES.
Statistical analyses
Paired t tests were used to assess changes in T-scores from before to during COVID. We chose paired t tests for this analysis since measurements were taken from the same individual. McNemar’s test was used to assess changes in clinically elevated symptoms. We first estimated changes in depressive and anxiety symptoms by subtracting the continuous baseline total score from the score during the pandemic. Linear regression models were then used to assess the impact of continuous measures of maternal stress, social support, and changes in depressive and anxiety symptoms. Depressive and anxiety scores were also dichotomized at clinically relevant cut-points to see the impact of exposures on the odds of more severe mental health symptoms during the pandemic. For dichotomized outcomes, we used logistic regression models and odds ratio (OR) and 95% confidence intervals (CIs) were reported. In secondary analyses, we additionally assessed associations between child resiliency and mental health symptoms for those with resiliency measures available (N = 392).
We assessed whether associations differed by child sex by using an augmented product term approach.29 We specified a model that included product terms between sex and all covariates—this model is equivalent to a fully stratified model. From this model, we were able to evaluate the sex–exposure product term; a p < 0.10 cut-off was used to indicate a significant effect measure modification by child sex.29 All statistical analyses were conducted using Stata Version 17.0.
Results
Table 1 provides sample descriptive characteristics of the study population before and during COVID. Children were on average 11.1 ± 1.1 years (min: 8.9, max: 12.8) at the COVID visit; there was an even distribution of females and males. Mothers were on average 39 years and primarily of lower SES. Average maternal-reported NLEs were slightly lower during COVID compared to before (3.2 vs. 2.9). In our study population, COVID visit assessments occurred between May and October 2020; maternal-reported stress levels were higher for those assessed in later months (Supplemental Table 2).
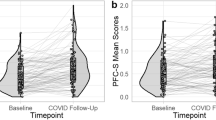
Overall, the mean anxiety T-score was comparable to the age-standardized population (i.e., means around 50); however, scores were slightly higher for both the child and parent-reported depressive symptom T-scores (Table 1). Table 2 presents the mean differences in child and parent-reported depressive symptom and child-reported anxiety symptom T-scores from before to during COVID. Overall, depressive symptoms increased from before to during COVID, for both child (1.18, 95% CI: 0.13, 2.23) and parent-reported measures (1.76, 95% CI: 0.96, 2.56) (Table 2). These differences were more prominent for girls, children from lower SES families, and those with less social support. On average, anxiety levels slightly decreased from before to during COVID, particularly for boys.
The percentage of females reporting depressive symptoms almost doubled from before to during COVID, for both child and parent-reported symptoms (Supplemental Table 3). Anxiety symptoms did not significantly change. Self-reported outcome measures were in general moderately correlated across measures and visits (Supplemental Fig. 3). Correlations between self and parent-reported depressive symptoms ranged from 0.18 (pre-COVID) to 0.39 (during COVID).
Table 3 presents the results for associations between continuous measures of maternal stress and social support during COVID-19 and changes in child depressive and anxiety symptoms. Higher maternal stress during the pandemic was associated with increases in parent and child-reported depressive scores. For every one-unit increase in maternal stress scores, child depressive scores increased by about 0.7 points (b: 0.72, 95% CI: 0.12, 1.31). We observed similar findings for parent-reported depressive symptoms (b: 0.77, 95% CI: 0.30, 1.23), but not with child-reported anxiety (Table 3). We additionally did not observe any overall associations between maternal social support and changes in depressive or anxiety symptoms (Table 3).
Next, we assessed associations with dichotomized outcomes in order to assess associations with clinically relevant depressive and anxiety symptoms during the pandemic. Higher maternal stress during the pandemic was associated with higher odds of clinically elevated depressive (OR: 1.19, 95% CI: 1.03, 1.37) and anxiety (OR: 1.19, 1.02, 1.39) symptoms (Table 4). There was a significant sex interaction for child-reported depressive and anxiety symptoms. For instance, for child-reported anxiety symptoms, we observed associations in girls (OR: 1.36, 95% CI: 1.12, 1.66), but not in boys (OR: 0.92, 95% CI: 0.69, 1.22) (p-interaction: 0.03) (Table 4). Children of mothers with higher social support had lower odds of clinically elevated parent-reported depressive symptoms (Table 4).
We additionally assessed the role of child resiliency prior to COVID on changes in child anxiety and depressive symptoms for a subset of children with these measures available. We observed inconsistent findings for change scores, with non-significant decreases for child-reported measures and increases for parent-reported depressive symptoms (Table 3). In dichotomized models, we saw a protective effect of child resiliency, with fewer depressive and anxiety symptoms for those children with higher resiliency (Table 4). Specifically, there was a decreased odds of clinically elevated child (OR: 0.94, 95% CI: 0.91, 0.97) and parent-reported (OR: 0.89, 95% CI: 0.85, 0.93) depressive symptoms for every one-unit increase in child resiliency T-scores.
Discussion
In this investigation of maternal stress and social support during the pandemic in relation to child mental health, we leveraged a comprehensive assessment of anxiety and depressive symptoms pre- and post-pandemic that included both child and parent-reported measures. Similar to previous studies,30,31 we observed low-to-moderate correlations between child and parent-reported depressive symptoms. We additionally observed a higher prevalence of depressive symptoms for the child-reported compared to the parent-reported measures. This is consistent with other studies that have reported higher mental health symptoms for child-reported measures. A recent meta-analysis found the pooled prevalence of clinically significant depressive and anxiety symptoms to be around 0.25 and 0.21, respectively.32 Our clinically elevated depressive symptom prevalence was 0.19 and 0.16 for anxiety symptoms.
Overall, we found that higher maternal stress during the pandemic was associated with increases in child and parent-reported depressive symptoms and child-reported anxiety symptoms. A few recent studies have found consistent results with associations seen between COVID-related stressors and changes in mental health.33,34,35,36 Recent reviews have found the strongest associations with anxiety and depressive symptoms in youth.7 While we did not address COVID stress directly, our results are consistent with the literature regarding stressors during COVID on child mental health outcomes.
Research has shown that maternal social support may reduce the harmful impacts of stress by altering the perception of the situation.37 This is particularly important during the pandemic, as a greater perceived connection to family, friends, and the community may buffer against pandemic-related stressors and impacts from social isolation. In the current study, maternal-reported social support was associated with fewer parent-reported child mental health symptoms—though overall associations were inconsistent with maternal social support measures. It could be that child reported social support from friends is more important during the pandemic. We unfortunately did not have this information for the current study but will measure it in the future. We additionally found associations between child resiliency and fewer reported mental health symptoms. This is consistent with previous findings on child resilience during other major life stressors and provides support for promoting child resilience in the face of novel major life stressors.38
The proportion of children experiencing clinically elevated depressive symptoms increased from before to during COVID-19. This may in part be due to increases in mental health symptoms with the increasing age of the children. We accounted for this by controlling for age in both assessments. These differences were primarily driven by girls, with the proportion of girls experiencing significant mental health symptoms almost doubling from before to during the pandemic. We found slight decreases in continuous anxiety symptoms from before to during the pandemic, particularly for boys. We hypothesize that this finding may be related to decreases in social anxiety symptoms from reduced social interactions during the pandemic. We also observed differences in the maternal NLE–child anxiety association by sex, with associations only seen in girls. Several recent studies have shown higher levels of depression and anxiety in female youth during the pandemic15,33 and increased symptoms of loneliness and social media use.39 Thus, females may be both more impacted by the pandemic in general and also by family-related stressors.
In Mexico City, the first confirmed COVID case was in February 2020, with school closures and social distancing measures following shortly after in March. Our assessment occurred during May–November 2020, so captures pandemic-related stressors during the early wave of the pandemic in Mexico City. During this early period, COVID cases peaked around July 2020 and continued for several months through the fall. Thus, our assessments were conducted when COVID cases were considerably high in Mexico City. Although cases were high throughout this time, there may be other factors that would have changed throughout this time from May to November 2002. We assessed changes in outcome symptoms by assessment month and observed no apparent differences.
Our study is not without limitations. We had no direct measure of how the pandemic affected the mother or child or whether other individuals in the family had contracted COVID-19. Additionally, we assessed symptoms in children using screening tools and acknowledge that these tools do not diagnose depression or anxiety, but instead provide an indication of severity. Cronbach’s alphas ranged from 0.6 to 0.8 for our outcome measures. While we acknowledge that these are on the lower side, these are acceptable ranges for internal consistency.40 We also acknowledge the potential impact of unmeasured confounders. Maternal SES was only available at baseline, yet the economic standing of many families likely changed during the pandemic. Economic standing was part of the stress questionnaire, thus adjusting for the change in SES would likely remove some of the variances we were interested in capturing. We also did not have information on whether the child felt they had adequate social support or suffered undue economic distress during the pandemic. Finally, we acknowledge the loss to follow-up in our study. We evaluated close to 600 participants at visits prior to and during COVID; however, participants were only included in the analysis if they had complete data for both visits.
Our study has several strengths. We leveraged data from a longitudinal prospective birth cohort study to assess the association between both maternal-reported stress and social support in relation to child mental health outcomes. Our study incorporated outcome data measured prior to and during the pandemic, and thus we were able to assess changes in mental health symptoms in the same cohort of children. Our results showed similar findings across respondents, thus giving strength to the evidence for an association with mental health outcomes. We additionally controlled for time-varying confounders, including child age. Finally, our main analyses used a dimensional outcome assessment approach and showed subclinical effects on mental health.41
Conclusion
The COVID-19 pandemic has disrupted nearly all aspects of life, creating unique stressors and placing under-resourced populations at a potential increased risk of mental health conditions. Thus, under these unprecedented times, where the most effective way to prevent the virus from spreading is social distancing, we need to also consider the impact these policies may have on the stagnation of children’s development and the likelihood this may lead to mental health symptoms. The findings from our study highlight the need for additional resources and programs for parents, clinicians, and mental health providers to be able to provide support for children going through similar events to reduce mental health impacts in this population, as well as increased screening of mental health symptoms. Emphasis should be placed on promoting social support and children’s resilience as children transition through these early years, particularly in the face of a novel major life stressor. Finally, PROGRESS is continuing to follow up participants—future analyses will continue to assess support, resilience, and mental health outcomes in children, with a particular emphasis on long-term pandemic-related impacts throughout the adolescent years.
Data availability
The datasets generated during and/or analyzed during the current study are not publicly available due to privacy concerns, but a limited dataset may be available from the corresponding author on reasonable request.
References
Brooks, S. K. et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 395, 912–920 (2020).
Lee, C. M., Cadigan, J. M. & Rhew, I. C. Increases in loneliness among young adults during the Covid-19 pandemic and association with increases in mental health problems. J. Adolesc. Health 67, 714–717 (2020).
Loades, M. E. et al. Rapid systematic review: the impact of social isolation and loneliness on the mental health of children and adolescents in the context of Covid-19. J. Am. Acad. Child Adolesc. Psychiatry 59, 1218.e3–1239.e3 (2020).
Russell, B. S., Hutchison, M., Tambling, R., Tomkunas, A. J. & Horton, A. L. Initial challenges of caregiving during Covid-19: caregiver burden, mental health, and the parent-child relationship. Child Psychiatry Hum. Dev. 51, 671–682 (2020).
Cost, K. T. et al. Mostly worse, occasionally better: impact of Covid-19 pandemic on the mental health of canadian children and adolescents. Eur. Child Adolesc. Psychiatry 31, 671–684 (2021).
Qin, Z. et al. Prevalence and risk factors associated with self-reported psychological distress among children and adolescents during the Covid-19 pandemic in China. JAMA Netw. Open 4, e2035487 (2021).
Samji, H. et al. Review: Mental health impacts of the Covid-19 pandemic on children and youth - a systematic review. Child Adolesc. Ment. Health 27, 173–189 (2021).
Khambadkone, S. G., Cordner, Z. A. & Tamashiro, K. L. K. Maternal stressors and the developmental origins of neuropsychiatric risk. Front. Neuroendocrinol. 57, 100834 (2020).
Van den Bergh, B. R. H. et al. Prenatal developmental origins of behavior and mental health: the influence of maternal stress in pregnancy. Neurosci. Biobehav. Rev. 117, 26–64 (2020).
Serrano-Villar, M., Huang, K. Y. & Calzada, E. J. Social support, parenting, and social emotional development in young Mexican and Dominican American children. Child Psychiatry Hum. Dev. 48, 597–609 (2017).
Benjet, C., Borges, G., Medina-Mora, M. E., Zambrano, J. & Aguilar-Gaxiola, S. Youth mental health in a populous city of the developing world: results from the Mexican adolescent mental health survey. J. Child Psychol. Psychiatry 50, 386–395 (2009).
Zuccolo, P. F. et al. Children and adolescents’ emotional problems during the Covid-19 pandemic in Brazil. Eur. Child Adolesc. Psychiatry https://doi.org/10.1007/s00787-022-02006-6 (2022).
Bravo-Sanzana, M., Oriol, X. & Miranda, R. Characterization of wellbeing and its relationship with exposure to violence in Mexican and Chilean early and late adolescents during the Covid-19 pandemic. Child Indic. Res. 15, 553–578 (2022).
CDC. The social-ecological model: a framework for prevention. https://www.cdc.gov/violenceprevention/about/social-ecologicalmodel.html (2021).
Meherali, S. et al. Mental health of children and adolescents amidst Covid-19 and past pandemics: a rapid systematic review. Int. J. Environ. Res. Public Health 18, 3432 (2021).
Braun, J. M. et al. Relationships between lead biomarkers and diurnal salivary cortisol indices in pregnant women from Mexico City: a cross-sectional study. Environ. Health 13, 50 (2014).
Davanzo, P. et al. Spanish translation and reliability testing of the child depression inventory. Child Psychiatry Hum. Dev. 35, 75–92 (2004).
Ferrando, P. J. Factorial structure of the Revised Children Manifest Anxiety Scale in a Spanish sample - relations with Eysenck personality dimensions. Pers. Indiv. Differ. 16, 693–699 (1994).
Kovacs, M. & MHS Staff. Children’s Depression Inventory 2nd Edition (Cdi 2) Technical Manual (MHS, Inc., 2011).
Berry, C. A., Quinn, K. A., Portillo, N. & Shalowitz, M. U. Reliability and validity of the Spanish Version of the Crisis in Family Systems-Revised. Psychol. Rep. 98, 123–132 (2006).
Shalowitz, M. U., Berry, C. A., Rasinski, K. A. & Dannhausen-Brun, C. A. A new measure of contemporary life stress: development, validation, and reliability of the Crisys. Health Serv. Res. 33, 1381–1402 (1998).
Myers, H. F. Ethnicity- and socio-economic status-related stresses in context: an integrative review and conceptual model. J. Behav. Med. 32, 9–19 (2009).
Rosa, M. J. et al. Prenatal and postnatal stress and wheeze in Mexican children: sex-specific differences. Ann. Allergy Asthma Immunol. 116, 306–312 e301 (2016).
Tamayo, Y. O. M. et al. Maternal stress modifies the effect of exposure to lead during pregnancy and 24-month old children’s neurodevelopment. Environ. Int. 98, 191–197 (2017).
Mendoza-Núñez, V. M., González-Mantilla, F., Correa-Muñoz, E. & Retana-Ugalde, R. Relationship between social support networks and physical functioning in older community-dwelling Mexicans. Int. J. Environ. Res. Public Health 14, 993 (2017).
Reynolds, C. R. & Kamphaus, R. W. Basc-2: Behavior Assessment System for Children, 2 (Pearson, 2004).
Textor, J., Hardt, J. & Knuppel, S. Dagitty: a graphical tool for analyzing causal diagrams. Epidemiology 22, 745 (2011).
Carrasco, A. J. E. The Amai system of classifying households by socio-economic level: the experience of Mexico and its comparison with Brazil and Argentina. www.esomar.org (2002).
Buckley, J. P., Doherty, B. T., Keil, A. P. & Engel, S. M. Statistical approaches for estimating sex-specific effects in endocrine disruptors research. Environ. Health Perspect. 125, 067013 (2017).
Achenbach, T. M., McConaughy, S. H. & Howell, C. T. Child/adolescent behavioral and emotional problems: implications of cross-informant correlations for situational specificity. Psychol. Bull. 101, 213–232 (1987).
De Los Reyes, A. & Kazdin, A. E. Informant discrepancies in the assessment of childhood psychopathology: a critical review, theoretical framework, and recommendations for further study. Psychol. Bull. 131, 483–509 (2005).
Racine, N. et al. Global prevalence of depressive and anxiety symptoms in children and adolescents during Covid-19: a meta-analysis. JAMA Pediatr. 175, 1142–1150 (2021).
Hawes, M. T., Szenczy, A. K., Klein, D. N., Hajcak, G. & Nelson, B. D. Increases in depression and anxiety symptoms in adolescents and young adults during the Covid-19 pandemic. Psychol. Med. https://doi.org/10.1017/S0033291720005358 (2021).
Tang, S., Xiang, M., Cheung, T. & Xiang, Y. T. Mental health and its correlates among children and adolescents during Covid-19 school closure: the importance of parent-child discussion. J. Affect Disord. 279, 353–360 (2021).
Mohler-Kuo, M., Dzemaili, S., Foster, S., Werlen, L. & Walitza, S. Stress and mental health among children/adolescents, their parents, and young adults during the first Covid-19 lockdown in Switzerland. Int. J. Environ. Res. Public Health 18, 4668 (2021).
Qi, M. et al. The effect of social support on mental health in chinese adolescents during the outbreak of Covid-19. J. Adolesc. Health 67, 514–518 (2020).
Barnett, M., Mortensen, J., Tilley, E. & Gonzalez, H. Global and parenting-specific social support as protective factors for the well-being of Mexican American mothers of toddlers. Fam. Sci. 4, 98–109 (2013).
Masten, A. S., Lucke, C. M., Nelson, K. M. & Stallworthy, I. C. Resilience in development and psychopathology: multisystem perspectives. Annu. Rev. Clin. Psychol. 17, 521–549 (2021).
Ellis, W., Dumas, T. & Forbes, L. Physically isolated but socially connected: psychological adjustment and stress among adolescents during the initial Covid-19 crisis. Can. J. Behav. Sci. 52, 177–187 (2020).
Shrout, P. E. Measurement reliability and agreement in psychiatry. Stat. Methods Med. Res. 7, 301–317 (1998).
Sagiv, S. K., Kalkbrenner, A. E. & Bellinger, D. C. Of decrements and disorders: assessing impairments in neurodevelopment in prospective studies of environmental toxicant exposures. Environ. Health 14, 8 (2015).
Funding
This work was supported by the NIH [grant numbers T32HD049311, R01ES013744, R01ES021357, P30ES023515, R00ES027496, R24ES028522, and K99ES032480].
Author information
Authors and Affiliations
Contributions
We confirm that all coauthors have made substantial contributions to the conception and design, acquisition of data, or analysis and interpretation of data; drafting the article or revising it critically for important intellectual content; and final approval of the version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
All women provided informed consent and children provided assent.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
McGuinn, L.A., Rivera, N.R., Osorio-Valencia, E. et al. Changes in depressive and anxiety symptoms during COVID-19 in children from the PROGRESS cohort. Pediatr Res 94, 349–355 (2023). https://doi.org/10.1038/s41390-022-02379-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-022-02379-z
This article is cited by
-
Trajectory of depressive symptoms over adolescence in autistic and neurotypical youth
Molecular Autism (2024)
-
Anxiety increased among children and adolescents during pandemic-related school closures in Europe: a systematic review and meta-analysis
Child and Adolescent Psychiatry and Mental Health (2023)
