
Abstract
Background
An oxygen saturation (SpO2) histogram classification system has been shown to enable quantification of SpO2 instability into five types, based on histogram distribution and time spent at SpO2 ≤ 80%. We aimed to investigate this classification system as a tool to describe response to doxapram treatment in infants with severe apnea of prematurity.
Methods
This retrospective study included 61 very-low-birth-weight infants who received doxapram. SpO2 histograms were generated over the 24-h before and after doxapram start. Therapy response was defined as a decrease of ≥1 histogram types after therapy start.
Results
The median (IQR) histogram type decreased from 4 (3–4) before to 3 (2–3) after therapy start (p < 0.001). The median (IQR) FiO2 remained constant before (27% [24–35%]) and after (26% [22–35%]) therapy. Thirty-six infants (59%) responded to therapy within 24 h. In 34/36 (94%) of the responders, invasive mechanical ventilation (IMV) was not required during the first 72 h of therapy, compared to 15/25 (60%) of non-responders (p = 0.002). Positive and negative predictive values of the 24-h response for no IMV requirement within 72 h were 0.46 and 0.94, respectively.
Conclusions
Classification of SpO2 histograms provides an objective bedside measure to assess response to doxapram therapy and can serve as a tool to detect changes in oxygenation status around respiratory interventions.
Impact
-
The SpO2 histogram classification system provides a tool for quantifying response to doxapram therapy.
-
The classification system allowed estimation of the probability of invasive mechanical ventilation requirement, already within a few hours of treatment.
-
The SpO2 histogram classification system allows an objective bedside assessment of the oxygenation status of the preterm infant, making it possible to assess the changes in oxygenation status in response to respiratory interventions.
Similar content being viewed by others

Introduction
Oxygenation instability with frequent hypoxic episodes is common in preterm infants during the first weeks after birth1 and is associated with the development of bronchopulmonary dysplasia (BPD), severe retinopathy of prematurity (ROP), cerebral palsy, and death.2,3,4,5 Although oxygen saturation (SpO2) is continuously monitored in preterm infants admitted to the neonatal intensive care unit (NICU), objective assessment of oxygenation instability remains challenging in daily clinical care.
SpO2 histograms graphically illustrate the percentage of time an infant spends at each SpO2 value, allowing bedside presentation of the oxygenation instability in preset time periods. Monitoring SpO2 histograms of preterm infants in the NICU increases the percentage of time infants are in the target SpO2 range6,7 and is associated with a reduction in BPD, severe ROP, and death.7,8 Furthermore, SpO2 histograms can predict successful weaning off nasal continuous positive airway pressure in preterm infants,9 as well as the need for prolonged respiratory care.10 A classification system based on histogram distribution and time spent at an SpO2 ≤ 80% for evaluation of oxygenation instability in preterm infants10 and their response to position change11 was recently described.
Doxapram is a respiratory stimulant used off-label as a second-line drug next to caffeine in the treatment of apnea of prematurity (AOP) to decrease the incidence of desaturation events and to avoid invasive mechanical ventilation (IMV).12
We hypothesized that classifying SpO2 histograms could provide objective, bedside assessment of oxygenation instability around clinical interventions. The aim of our study was therefore to assess the use of the SpO2 histogram classification system as an objective tool to describe the response to doxapram treatment in infants with severe AOP. We further examined whether the histogram classification system could estimate the probability of IMV requirement.
Methods
Study population and design
In this retrospective, observational study, prospectively collected data on SpO2 and supplemented oxygen around doxapram therapy in preterm infants were analyzed. All very-low-birth-weight (VLBW) preterm infants who received doxapram therapy during their admission at the level IV NICU of Erasmus MC Sophia Children’s Hospital (Rotterdam, The Netherlands) between December 2013 and June 2017 were eligible for inclusion. The included infants participated in the previous study that investigated the use of physiological data before and during doxapram therapy.13 In the current study, only infants with available monitor data were included (N = 61). The local ethics review board granted a waiver from approval according to the Medical Research Involving Human Subjects Act in the Netherlands (MEC-2018-1106).
Data collection
Baseline characteristics, SpO2, and fraction of inspired oxygen (FiO2) were measured, stored, and processed as described in the methods of the previously conducted study.13 Baseline characteristics were collected from the electronic medical records (HiX version 6.1, Chipsoft, Amsterdam, Netherlands). Data on the FiO2 were collected from the electronic patient data management system (Picis Clinical Solutions, Inc., Wakefield, MA) and HiX. Per-second SpO2 data were automatically recorded (1 Hz) and extracted from bedside monitors (Draegerwerk AG & Co KGaA, Lübeck, Germany) and used to generate SpO2 histograms. Data were filtered for invalid measurements that were marked by the monitor, and zero values were removed from the analysis. Four histograms were generated for each infant over the available 48 h around doxapram start. At therapy start, a 24-h histogram was generated, summarizing oxygenation instability in the 24 h prior to therapy start. In addition, 4-, 12-, and 24-h histograms were generated, describing the oxygenation instability in the 4, 12, and 24 h after therapy start. A previously defined SpO2 histogram classification system was used to quantify SpO2 instability into five histogram types, based on the histogram distribution and the time spent at an SpO2 ≤ 80%.10 The histograms were generated and classified using the R software (version 3.5.3, R Foundation for Statistical Computing, Vienna, Austria). Types 1 and 2 have the smallest spread in SpO2 values and are therefore considered as stable histograms, while types 3–5 represent a large spread and SpO2 values ≤ 80% are considered as unstable histograms10 (Fig. 1). Additionally, the percentage of time spent within the unit’s target range of 89–95%, as well as time spent at SpO2 ≤ 80%, and SpO2 > 95% were calculated in the 24-h period before and after therapy start.

The graphs present the histograms of one subject during the 24 h before (a) and after (b) therapy start. The black bars present the time percentage spent at each SpO2 value, and the gray bars present the cumulative time percentage. The histograms are classified into 5 types based on the number of cumulative bars (gray) between the 10th and 90th percentile and the time spent at an SpO2 ≤ 80% (c). In this example, the histogram is classified as type 3 before therapy start (11 cumulative bars, and 3% of the time spent at an SpO2 ≤ 80%), and as type 2 after therapy start (5 cumulative bars, and no time spent at an SpO2 ≤ 80%).
Doxapram therapy
Doxapram was administered off-label according to the local protocol as a rescue treatment aiming to avoid IMV for infants with severe AOP. Therapy was indicated in infants with persisting apneas despite optimal caffeine treatment and maximal noninvasive ventilation support. Doxapram was only started if the occurrence of apneas could not be explained by other morbidities, such as sepsis, necrotizing enterocolitis, interventricular hemorrhage, and severe anemia. The local protocol stated a loading dose of 2.5 mg/kg over 10 min, followed by a maintenance dose of 2.0 mg/kg/h. Therapy was administered intravenously, or enterally via a nasogastric tube. The maintenance dose was titrated based on the frequency of apneas. Therapy was discontinued in infants who had no significant apneas left based on clinical indication or who required IMV. The first course of doxapram of each infant was included in the analysis. A new course was defined as therapy restart at least 24 h after termination of the previous course. Response and lack of response to doxapram therapy were defined based on the change in histogram type after therapy initiation. Response to therapy was defined as a drop of at least 1 histogram type after doxapram start, compared to the 24-h histogram type prior to doxapram start. The local criteria for IMV included persistent or severe apnea, increased oxygen needs, or severe desaturations.
Statistical analysis
Baseline characteristics were described as median (interquartile range (IQR)) or number (%). Differences in characteristics between the groups with and without therapy response were analyzed using the Wilcoxon rank-sum test, Fisher’s exact test, and X2 test where appropriate. The histogram types, SpO2, and the percentage of time in different SpO2 ranges were calculated as median (IQR). Differences before and after therapy were tested using the Wilcoxon signed-rank test. For the SpO2 and FiO2, the difference between the area under the curve before and after therapy was analyzed. The rates of therapy response in the 4, 12, and 24 h after therapy start were calculated based on the histogram type of the 24 h prior to therapy start. The positive predictive value (PPV) and negative predictive value (NPV) of therapy response at 4, 12, and 24 h for not needing IMV within 72 h were calculated. Statistical analyses were performed using the R software. The significance threshold was set to p < 0.05.
Results
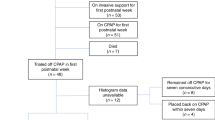
Oxygenation instability was studied in 61 VLBW preterm infants who received doxapram therapy. The demographic data of infants participated in the study are presented in Table 1. Histograms of four different time periods (24 h before doxapram start, and 4, 12, and 24 h after doxapram start) were generated and classified for each infant (Fig. 1), with a total of 244 histograms.
Overall, the median (IQR) histogram type dropped significantly from type 4 (3-4) in the 24-h histogram prior to therapy start to type 3 (2–3) in the 24-h histogram after therapy start (p < 0.001). The median (IQR) FiO2 requirements remained unchanged during the 24 h before (27% (24–35%)) and after therapy start (26% (22–35%); p = 0.28). The median SpO2 increased from 94% (93–95%) 24 h prior to doxapram start to 95% (94–96%) 24 h after doxapram start (p < 0.001). The median (IQR) time spent within the SpO2 target range of 89–95% remained stable in the 24 h before (47% (37–56%)) and after (45% (34–56%)) therapy start (p = 0.35). The median (IQR) time spent at an SpO2 ≤ 80% dropped significantly from 5% (3–7%) before to 2% (1–4%) after therapy (p < 0.001), and the median (IQR) time spent at an SpO2 > 95% increased significantly from 33% (23–43%) before to 42% (26–60%) after (p < 0.001).
The infants were divided into responders and non-responders, based on a decrease in the 24-h histogram type after therapy start, relative to the 24-h histogram type before therapy. Overall, 36/61 infants (59%) responded to doxapram initiation, with a median (IQR) decrease of 1 (1–1) type of histograms in responders. The demographic data of the responders and non-responders are presented in Table 1. The gestational age, birth weight, postmenstrual age at doxapram start, and mortality rate during hospital admission were similar in responders and non-responders (Table 1). Non-responders more often received IMV during the 24 h before therapy start (p = 0.02). The median (IQR) doxapram therapy duration was longer in responders (10 (5–15) days) when compared to non-responders (6 (2–10) days; p = 0.03). The median (IQR) postnatal age at therapy start was significantly higher in responders (21 (17–30) days) when compared to non-responders (18 (13–24) days); p = 0.04).
The median histogram type decreased significantly in the 24 h after treatment initiation in responders, while the median histogram type did not change in non-responders (Fig. 2a). The median SpO2 increased significantly during the 24 h after therapy start in responders and did not change in non-responders (Fig. 2b), while the median FiO2 did not change in both groups (Fig. 2c). The percentage of time spent at an SpO2 89–95% did not change significantly for both groups (Fig. 2d). The percentage of time spent at an SpO2 ≤ 80% decreased significantly in responders only (Fig. 2e), and the percentage of time spent at an SpO2 > 95% increased significantly in both groups (Fig. 2f).

Boxplots of the 24 h before and after doxapram therapy start among responders (N = 36) and non-responders (N = 25) for a histogram type, b oxygen saturation (%), c fraction of inspired oxygen (%), d percentage of time spent in oxygen saturation (SpO2) of ≤ 80%, e percentage of time spent in SpO2 89–95%, and f percentage of time spent in SpO2 > 95%. The boxplot contains the interquartile range (IQR) and the central line denotes the median value. The whiskers mark the minimum and maximum values. A significant difference before and after therapy is marked with an asterisk.
The histogram types over the 24 h before therapy initiation were stratified, after which response and intubation rates for IMV after 72 h of therapy and at therapy stop were calculated per histogram type (Table 2). While 35/49 (71%) of the infants with unstable histograms (types 3–5) before therapy initiation responded to therapy during the 24 h after therapy initiation, only 1/12 (8%) of infants with a stable histogram of type 2 responded. Thirty-four out of 36 responders (94%) and 15 out of 25 non-responders (60%) did not require intubation in the first 72 h (p = 0.002), with an overall intubation rate at therapy stop of 11/36 (31%) in responders and 15/25 (60%) in non-responders (p = 0.03). The intubation rate during the first 72 h is presented for each pre-therapy histogram type in Table 2. The median (IQR) time to intubation was 0.4 (0.2–3.4) days in infants with pre-therapy histogram type 2, 5.3 (2.5–9.6) days in infants with type 3, 2.6 (1.2–10.0) days in infants with type 4, and 6.6 (5.2–8.1) days in infants with type 5. Twenty-one out of 25 (84%) of the infants who were mechanically ventilated during the 24 h pre-therapy had a histogram type between 3 and 5, and 4/25 (16%) infants had a histogram type 2. Absence of response to doxapram in the first 4-, 12-, and 24-h period yielded a PPV between 0.40 and 0.46 for intubation within the first 72 h of therapy. The NPV varied between 0.88 and 0.94, meaning that responders had a probability of 88–94% to avoid intubation within 72 h of therapy start.
Discussion
In this study, we used an SpO2 histogram classification system to objectively assess oxygenation instability around doxapram treatment, given as a rescue treatment to avoid intubation in VLBW infants with severe AOP. We found that the use of an SpO2 histogram classification system as a bedside tool might allow the care team to objectively assess oxygenation instability, to quantify the response to doxapram therapy, and to estimate the probability for IMV requirement already within a few hours of treatment.
AOP plays a major role in oxygenation instability in preterm infants.14 The assessment of oxygenation instability and decisions on treatment for AOP are currently based on nursing staff’s documentation of pulse oximeter data and heart rate alarms. In the 1980s, NICU staff were found to recognize only one-third of apnea events occurring.15 Since then, despite major technical innovations in this field making it possible to objectively measure desaturations, the correlation with hypoxic events that are detected and documented by the bedside staff is still minimal.16 SpO2 histograms are easily displayed by most bedside monitors. They allow a bedside quantification of the median SpO2, the time spent within different SpO2 ranges, and changes in the oxygenation instability. Their use by the care team was associated with a reduction in BPD, severe ROP, and death.7,8
The SpO2 histograms showed that the participating infants in this study spent less time within the SpO2 target range of 89–95% and more time in the hyperoxic range when compared to the literature.7,10 This probably reflects the oxygenation instability among this homogenous group of infants, who met the criteria to receive doxapram as a rescue treatment, as compared to other studies that described a less homogenous population. Interestingly, the improvement in oxygenation instability in responders manifested as less time spent at an SpO2 ≤ 80% and more time spent >95%, with a comparable time spent within the target range. Furthermore, in the responders the median SpO2 increased significantly in the 24 h after therapy start, although it remained within the clinical SpO2 target range. An increase in hyperoxia at the expense of decreased hypoxemia after a beneficial intervention was previously observed among VLBW infants when placed prone vs. supine.11 This response most likely results from the care team tendency to react appropriately to desaturations by increasing FiO2, but a slower downward titration when a desaturation resolves.17 Presenting SpO2 histograms around respiratory interventions can alert clinicians of an increased time spent at SpO2 values above the target range.
In order to quantify oxygenation instability, we used an easily applicable SpO2 histogram classification system that is based on the histogram distribution and the time spent at an SpO2 ≤ 80%. The time spent at an SpO2 ≤ 80% was previously found to be associated with adverse neonatal outcomes.1,4 The histogram classification system adds new information to the bedside team when combining these data with the SpO2 histogram distribution to quantify oxygenation instability. Using this classification system around doxapram treatment, we revealed a group of infants that did not demonstrate oxygen instability prior to doxapram initiation, despite the impression of the bedside clinical team. Most of these infants did not require IMV during the 24 h prior to therapy, had failed to respond to doxapram administration after 24 h, and were intubated shortly after therapy initiation. Classification of SpO2 histograms may facilitate clinical decisions prior to respiratory interventions, for a large proportion of these infants were eventually intubated.
Furthermore, 41% of the infants who participated in our study were extubated <24 h prior to doxapram initiation. Most of these infants had oxygenation instability in the 24-h prior to doxapram start, did not respond to doxapram, and were eventually reintubated. Various demographic, cardiovascular, and respiratory parameters are associated with extubation failure; however, predicting extubation failure among preterm infants remains challenging.18,19,20,21,22 By using the histogram classification system before and during doxapram treatment, we were able to estimate the probability for IMV requirement within 72 h at 4 h after the start of treatment. This could help the team to make decisions regarding intubation and limit exposure to hypoxemia and oxygenation instability by preventing prolonged ineffective doxapram treatment.
In previous publications, we showed in the same infants that continuous physiological monitor data can be used to measure the effect of doxapram therapy and predict therapy failure, as well as improve therapy with continuous monitoring.23 In the current study, we demonstrate the advantages of using the histogram classification system as a bedside tool. Histograms are broadly available in the currently used bedside monitors, and the graphical display of the histograms clearly presents the oxygenation stability and the time spent within different SpO2 ranges. The classification system can easily be applied to classify the histograms and compare them between different time frames.
Our study has a few limitations. The first limitation of our study is that an accurate understanding of the clinical decisions regarding the start, change, and stop of doxapram therapy was not possible due to the retrospective nature of the study. Objective criteria for respiratory insufficiency and intubation are unfortunately lacking in neonatal care. Scores to assess the severity of apnea have been suggested in literature, yet have not been validated in clinical practice.24 Although our study reflects the current standard of care, these issues with tracing back clinical decisions could pose a limitation. The second limitation is that we did not explore the response rates taking into account the doxapram dosages and route of administration. A difference in the exposure to doxapram could have influenced the level of response, although all infants were treated according to the same, local protocol.
It is challenging to treat preterm infants suffering from severe AOP. Trying to avoid IMV in order to reduce the risk of BPD and poor neurodevelopmental outcomes25 might lead to increased hypoxic exposure, which increases the risk of poor neurodevelopmental outcome.26 Using the SpO2 histogram classification system allows objective bedside evaluation of the oxygenation instability of the infant in several time periods, making it possible to assess the changes in oxygenation status in response to respiratory interventions. Future studies are needed to assess the clinical implication of SpO2 histograms classification on clinical decision support and outcomes of preterm infants.
Data availability
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
References
Di Fiore, J. M. et al. A higher incidence of intermittent hypoxemic episodes is associated with severe retinopathy of prematurity. J. Pediatr. 157, 69–73 (2010).
Imanishi, Y. et al. Effect of fluctuation of oxygenation on the development of severe retinopathy of prematurity in extremely preterm infants. J. Perinatol. 40, 515–521 (2020).
Poets, C. F. et al. Association between intermittent hypoxemia or bradycardia and late death or disability in extremely preterm infants. JAMA 314, 595–603 (2015).
Di Fiore, J. M. et al. Patterns of oxygenation, mortality, and growth status in the surfactant positive pressure and oxygen trial cohort. J. Pediatr. 186, 49.e1–56.e1 (2017).
Pillekamp, F. et al. Factors influencing apnea and bradycardia of prematurity - implications for neurodevelopment. Neonatology 91, 155–161 (2007).
Sivanandan, S. et al. Target oxygen saturation among preterm neonates on supplemental oxygen therapy: a quality improvement study. Indian Pediatr. 55, 793–796 (2018).
Gentle, S., El-Ferzli, G., Winter, L., Salas, A. A. & Philips Iii, J. B. Oxygen saturation histogram monitoring to reduce death or retinopathy of prematurity: a quality improvement initiative. J. Perinatol. 40, 163–169 (2020).
Srivatsa, B., Malcolm, K., Clark, R. H. & Kupke, K. G. Effect of a novel oxygen saturation targeting strategy on mortality, retinopathy of prematurity, and bronchopulmonary dysplasia in neonates born extremely preterm. J. Pediatr. 234, 33.e3–37.e3 (2021).
Gentle, S. J., Ambalavanan, N. & Carlo, W. A. Oxygen saturation histograms predict nasal continuous positive airway pressure-weaning success in preterm infants. Pediatr. Res. 88, 637–641 (2020).
Borenstein-Levin, L., Konikoff, L. & Solimano, A. Clinical quantification of SpO2 instability using a new histogram classification system: a clinical study. Pediatr. Res. 87, 716–720 (2020).
Miller-Barmak, A. et al. Oxygenation instability assessed by oxygen saturation histograms during supine vs prone position in very low birthweight infants receiving noninvasive respiratory support. J. Pediatr. 226, 123–128 (2020).
Flint, R. et al. Retrospective study shows that doxapram therapy avoided the need for endotracheal intubation in most premature neonates. Acta Paediatr. 106, 733–739 (2017).
Poppe, J. A. et al. Use of continuous physiological monitor data to evaluate doxapram therapy in preterm infants. Neonatology 117, 438–445 (2020).
Di Fiore, J. M. et al. Prematurity and postnatal alterations in intermittent hypoxaemia. Arch. Dis. Child. Fetal Neonatal Ed. 106, 557–559 (2021).
Southall, D. P. et al. Undetected episodes of prolonged apnea and severe bradycardia in preterm infants. Pediatrics 72, 541–551 (1983).
Brockmann, P. E. et al. Under-recognition of alarms in a neonatal intensive care unit. Arch. Dis. Child. Fetal Neonatal Ed. 98, F524–F527 (2013).
van Zanten, H. A. et al. The risk for hyperoxaemia after apnoea, bradycardia and hypoxaemia in preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 99, F269–F273 (2014).
Goel, N., Chakraborty, M., Watkins, W. J. & Banerjee, S. Predicting extubation outcomes-a model incorporating heart rate characteristics index. J. Pediatr. 195, 53–58 (2018).
Chakraborty, M., Watkins, W. J., Tansey, K., King, W. E. & Banerjee, S. Predicting extubation outcomes using the heart rate characteristics index in preterm infants: a cohort study. Eur. Respir. J. 56, 1901755 (2020).
Shalish, W. et al. Patterns of reintubation in extremely preterm infants: a longitudinal cohort study. Pediatr. Res. 83, 969–975 (2018).
Manley, B. J., Doyle, L. W., Owen, L. S. & Davis, P. G. Extubating extremely preterm infants: predictors of success and outcomes following failure. J. Pediatr. 173, 45–49 (2016).
Chawla, S. et al. Markers of successful extubation in extremely preterm infants, and morbidity after failed extubation. J. Pediatr. 189, 113.e2–119.e2 (2017).
Poppe, J. A. et al. Precision dosing of doxapram in preterm infants using continuous pharmacodynamic data and model-based pharmacokinetics: an illustrative case series. Front. Pharmacol. 11, 665 (2020).
Poets, C. F. Interventions for apnoea of prematurity: a personal view. Acta Paediatr. 99, 172–177 (2010).
Vliegenthart, R. J. S., van Kaam, A. H., Aarnoudse-Moens, C. S. H., van Wassenaer, A. G. & Onland, W. Duration of mechanical ventilation and neurodevelopment in preterm infants. Arch. Dis. Child. Fetal Neonatal Ed. 104, F631–F635 (2019).
Poets, C. F. & Lorenz, L. Prevention of bronchopulmonary dysplasia in extremely low gestational age neonates: current evidence. Arch. Dis. Child. Fetal Neonatal Ed. 103, F285–F291 (2018).
Funding
This study was supported by the Sophia Foundation (grant number: S18-27).
Author information
Authors and Affiliations
Contributions
L.B.L. and J.A.P. drafted the first version of this article. The authors substantially contributed to conception and design (L.B.L., J.A.P., S.H.P.S., W.v.W., A.K.), contributed to acquisition of data (J.A.P., I.K.M.R., W.v.W., H.R.T.), and to the analysis and interpretation of data (L.B.L., J.A.P., S.H.P.S., O.H.). All authors revised the article critically for important intellectual content and gave their final approval of the version to be published. The local ethics review board granted a waiver from approval according to the Medical Research Involving Human Subjects Act (WMO) in the Netherlands (MEC-2018-1106).
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Borenstein-Levin, L., Poppe, J.A., van Weteringen, W. et al. Oxygen saturation histogram classification system to evaluate response to doxapram treatment in preterm infants. Pediatr Res 93, 932–937 (2023). https://doi.org/10.1038/s41390-022-02158-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-022-02158-w
