
Abstract
Background
Limited data exist regarding child neurodevelopment in relation to maternal occupational exposure to endocrine-disrupting chemicals (EDCs).
Methods
We included 1058 mother–child pairs from the INfancia y Medio Ambiente (INMA) project (2003–2008). Using a job-exposure matrix, exposure probability scores for ten EDC groups were assigned to each mother based on her longest held job during pregnancy. At the child’s 5-year visit, the McCarthy Scales of Children’s Abilities was administered, yielding the general cognitive index and scales for specific cognitive domains. We analyzed region-specific associations between EDC exposures and each outcome separately using adjusted linear regression and combined region-specific effect estimates using random-effects meta-analyses.
Results
Approximately 24% of women were exposed to at least one EDC group, but exposure to most individual EDC groups was low (<5%). Maternal organic solvent exposure was associated with lower quantitative scores among children (−5.8 points, 95% confidence interval: −11.0, −0.5). Though statistically non-significant, exposures to polycyclic aromatic hydrocarbons, phthalates, alkylphenolic compounds, and miscellaneous chemicals were associated with poorer offspring performance for most or all cognitive domains.
Conclusions
This study found limited evidence for a role of maternal occupational EDC exposures on child cognition. Further research is needed to better characterize exposures among pregnant workers.
Impact
-
Using data from a prospective birth cohort, we help fill an important research gap regarding the potential consequences of work-related exposure to endocrine-disrupting chemicals (EDCs) among pregnant women on child neurodevelopment.
-
We expand on existing literature—largely limited to pesticide and organic solvent exposures—by using a job-exposure matrix to estimate exposure to several EDC groups.
-
We found limited evidence of an association between maternal occupational EDC exposure and children’s overall cognition.
-
We did observe specific associations between exposure to organic solvents and lower quantitative reasoning scores.
Similar content being viewed by others


Introduction
Endocrine-disrupting chemicals (EDCs) are ubiquitous environmental contaminants and pose a serious threat to human health, and exposures to EDCs that occur during sensitive periods of development may increase the risk of disease later in life.1,2 Fetal brain development is particularly vulnerable to EDC exposure, and changes in the brain that result from in utero EDC exposure are likely irreversible and may manifest in early-life deficits in cognitive function.1,3 Whether cognitive deficits are subclinical or present as clinically recognized disorders, such as learning disabilities, impairments in mental abilities may have significant negative implications for educational achievement, anti-social and criminal behavior, and economic productivity.2
The workplace may be an important source of exposure to EDCs among some pregnant women. In western countries, most women in the workforce are of reproductive age and may continue working while pregnant.4 Although exposure to many EDCs among the general population is widespread, women in certain professions may be exposed to higher concentrations or come into more frequent contact with EDCs than the community at large, thereby potentially leading to fetal exposure at levels above background concentrations.5 Exposure often occurs though handling of products in which EDCs are an ingredient; for example, the handling of pesticides in gardening and horticultural trades, the use of cosmetics—considered an exposure source for many chemicals—among beauticians and related occupations, and the use of cleaning agents, such as solvents or disinfectants, among industrial and domestic cleaners.6
While mounting evidence links prenatal exposure to EDCs in the general environment with impairment in various aspects of childhood cognitive function,7,8,9,10,11 less data exist regarding childhood neurodevelopment in relation to maternal exposure to EDCs in occupational settings. In a 2009 systematic review of literature examining workplace exposure to chemicals among pregnant women and their children’s neurodevelopment, Julvez and Granjean12 summarized 15 studies, the majority of which reported delays in infant or child neurodevelopment associated with maternal occupational chemical exposures. The authors, however, highlighted important limitations of the literature overall: the classes of chemicals assessed were limited to organic solvents and pesticides, most studies were based on small samples (n > 100), and there was significant methodologic heterogeneity in neurodevelopmental assessment regarding children’s ages and psychometric instrument used. Studies published since have either investigated specific occupational groups, such as hairdressers,13 or focused on pesticide exposure.14 Much of the evidence regarding pesticides arose from a cohort of children in a farmworker community and suggests that higher maternal levels of organophosphate metabolites during pregnancy is associated impairments in children’s intelligence and attention.15,16 Yet, a paucity of evidence remains in regard to the diversity of endocrine-disrupting compounds to which pregnant workers may be exposed.
Given the need for additional evidence, we applied a widely used job-exposure matrix (JEM)17,18 to examine associations between maternal occupational exposure to multiple EDC groups and child cognitive function at 5 years of age among a population-based prospective birth cohort and hypothesized that children’s cognitive abilities would be negatively associated with maternal work-related EDC exposure during pregnancy.
Methods
Study population
The present analysis uses data from the INMA Project (INfancia y Medio Ambiente; Childhood and Environment), a population-based prospective birth cohort in Spain.19 The current analysis includes women and their children from three INMA regions—Gipuzkoa, Sabadell, and Valencia—where recruitment took place from 2003 to 2008 during women’s first routine prenatal care visit at the main public hospital in their respective study region. Women were recruited if they met the following eligibility criteria: ≥16 years of age, singleton pregnancy, 0–13 weeks of gestation, non-assisted conception, intention to deliver at the reference hospital, and no communication impairment. The study was approved by the ethics committees at the reference hospitals, and all women gave written informed consent prior to enrollment.
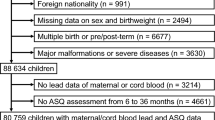
Mother–child pairs were followed up at approximately 32 weeks of gestation, at birth, and when the children were approximately 5 years of age. Of the women followed up at birth, 1739 (86%) reported having paid employment during pregnancy, of which 1519 had job titles for which EDC exposure could be estimated. At age 5 years, 1058 children completed the cognitive assessment and were included in the present analysis (see the study flowchart in Fig. 1).

Study flowchart for INMA participants in the Gipuzkoa, Sabadell, and Valencia regions, 2003–2008 (Spain).
Occupational EDC exposure
During the third trimester of pregnancy, trained interviewers administered a questionnaire that ascertained details about mothers’ employment status and occupational history. Based on mothers’ longest held job during pregnancy during the period of 1 month before conception and up to approximately 32 weeks of pregnancy, a JEM was applied to estimate occupational exposure to 10 EDC groups—polycyclic aromatic hydrocarbons (PAHs), polychlorinated bisphenols, pesticides, phthalates, organic solvents, bisphenol A (BPA), alkylphenolic compounds, brominated flame retardants, metals, and miscellaneous chemicals (i.e., benzophenones, parabens, and siloxanes). The JEM—originally created by Van Tongeren et al.20 and later updated by Brouwers et al.6—was developed with experts in occupational hygiene to assign exposure probability scores for 353 job titles. The exposure probability scores reflect the likelihood that exposure levels exceed background levels in the general population and are categorized into three levels: “unlikely” (unlikely to exceed general background levels), “possible” (expected to occur among up to 10% of workers with a given job title), or “probable” (expected to occur among >10% of workers with a given job title). The JEM also included a fourth exposure category, “unclassifiable”, for job titles for which an assignment could not be made.
Job titles of INMA participants’ longest held job during pregnancy were linked to International Standard Classification of Occupations 1988 (ISCO-88) codes. Because the JEM was developed using the Standard Occupational Classification 2000 (SOC2000) coding system,21 the JEM was first translated from SOC2000 to ISCO88 codes using the CAMSIS tool22 and expert opinion.23 Then, exposure probability scores were assigned based on mothers’ ISCO88 codes. Of the 1739 women who reported working during pregnancy and were followed up to birth, 220 (12.7%) had job codes for which exposure was assigned as “unclassifiable.” Accounting for attrition up to the 5-year study visit, exposure probability scores were available for 1058 women. Because data in the “probable” category were sparse (<5%), we collapsed the “possible” and “probable” exposure categories to create a dichotomous exposure variable for each EDC group. In addition, we created a metric for exposure to multiple EDC groups with three categories: unlikely exposure to any EDC group, possible or probable exposure to one EDC group, and possible or probable exposure to ≥2 EDC groups.
Cognitive function
At approximately 5 years of age, several domains of children’s cognitive function were assessed using a standardized version of the McCarthy’s Scales of Children’s Abilities (MSCA) adapted to the Spanish population24 and previously demonstrated to have high internal consistency (α-Cronbach >0.65) among a subset of children in the INMA study.25 The MSCA, consisting of 18 activity-based tasks, was administered by trained psychologists following a strict protocol to reduce inter-observer variability. During testing, the psychologists indicated any problems because of a child’s bad moods, tiredness, shyness, etc. Such tests were designated as poor quality (n = 45).
The tasks were grouped into five primary scales: verbal, perceptual-performance (i.e., non-verbal), quantitative reasoning, memory, and motor skills. The first three scales are mutually exclusive and include 15 of the 18 tasks. The general cognitive index, a measure of overall cognitive function, is created by combining the verbal, perceptual-performance, and quantitative scales. In addition, a measure associated with executive function was constructed using seven tasks critical to non-routine, goal-oriented situations performed by the prefrontal cortex.25 All scales were standardized to a mean of 100 and standard deviation (SD) of 15, with higher scores representing better cognitive or executive function.
Covariates
To guide the selection of covariates in the model, we created a directed acyclic graph (DAG) as a conceptual model for the association between occupational EDC exposures and child neurocognitive development. Based on the DAG, we included child sex from clinical records and the following variables from the first trimester questionnaire: maternal age at conception (years), highest achieved educational level (up to primary, secondary, or university), country of birth (Spain vs. other), and parity (0, 1, or ≥2 previous pregnancies). Also, using maternal height and self-reported weight information collecting during the first trimester, pre-pregnancy body mass index (kg/m2) was calculated and classified as underweight, normal weight, overweight, or obese, and gestational weight gain was classified as recommended, low or high following the Institute of Medicine guidelines.26 In addition, the following information collected during the third trimester questionnaire was included in our models as well: maternal smoking (any active smoking during pregnancy, yes vs. no) and alcohol consumption (at least one drink per week vs. fewer than one drink per week). We also included a proxy of maternal verbal intelligence quotient, estimated at the child’s 5-year visit using the Similarities subtest of the Wechsler Adult Intelligence Scales—Third Edition.27
Statistical analysis
To account for potential selection bias due to attrition, we used inverse probability weighting.28 Briefly, to calculate the probability of completing the outcome assessment at the 5-year visit, we fit logistic regression models to data from participants present at baseline from whom a JEM assignment could be made (n = 1519). We then used the inverse of these probabilities as weights in our main analysis so that the results would be representative of the subset of the initial cohort with complete exposure information during pregnancy. Additionally, for the 1058 mother–child pairs with complete exposure and outcome information, we performed multiple imputation of missing covariate values using chained equations, generating 25 complete datasets. The distributions of the imputed data were similar to the observed data (data not shown).
We used linear regression models to evaluate the association between maternal occupational EDC exposure and each MSCA score (i.e., general cognitive index, verbal, perceptual-performance, quantitative, memory, motor, and executive function). To account for potential heterogeneity between regions in the exposure–outcome association, we first analyzed associations separately by each region. Then, we combined region-specific effect estimates via random-effects meta-analysis. Because fetal sex determines the trajectory of fetal brain development29 and possibly responses to in utero EDC exposure,30 we explored potential differences in associations by stratifying analyses by child sex. Lastly, we performed a sensitivity analysis in which we excluded poor-quality tests (n = 45). All statistical analyses were performed using SAS 9.4 (Cary, NC). We considered associations with p values <0.05 as statistically significant.
Results
The demographic characteristics of mothers and children in the study population are described in Table 1. On average, mothers were approximately 31 years of age and 79% had completed at least a secondary education. Most were born in Spain (93.8%) and had no previous pregnancies (60.2%). The distribution of most covariates was similar across INMA regions with a few important differences. On average, children in Valencia performed the MSCA assessment at an older age (mean = 5.77 years) compared to children in Gipuzkoa and Sabadell (mean = 4.46 and 4.47 years, respectively). In addition, there were more mothers in Gipuzkoa with a university education (57.2%) compared to the other two regions (Sabadell: 35.3% and Valencia: 31.5%).
Approximately 17 and 14% of women were possibly or probably exposed to organic solvents and alkylphenolic compounds, respectively. For all other EDC groups, the potential for exposure was <5% and extremely low (<1%) for polychlorinated organic compounds, BPA, and brominated flame retardants (see Table 2). Most women with possible or probable exposure to two or more EDC groups (n = 167) were employed as hairdressers (19.8%) or domestic cleaners (57.5%), with hairdressers accounting for a significant proportion of women exposed to phthalates (68.8%), organic solvents (18.1%), alkylphenolic compounds (21.7%), and miscellaneous chemicals (78.6%) and domestic cleaners making up the majority of women with exposure to organic solvents (52.7%) and alkylphenolic compounds (63.2%). Other common professions with EDC exposures included waitresses (PAHs), assemblers of vehicles and metal goods (organic solvents), and plastics process operatives (phthalates, organic solvents, alkylphenolic compounds, metals, and miscellaneous chemicals).
We report unadjusted associations between maternal occupational EDC exposures and children’s cognitive function in Supporting Information, Table S1. Compared to the unadjusted results, the adjusted associations are attenuated (Table 3). Although mostly statistically non-significant, we observed consistent negative associations between cognitive domains and exposure to PAHs, phthalates, organic solvents, alkylphenolic compounds, and miscellaneous chemicals (Table 3). For example, exposure to organic solvents was associated with a 5.8-point decrease in quantitative reasoning scores (95% confidence interval (CI): −11.0, −0.5), and we found associations of similar magnitude and direction between exposure to alkylphenolic compounds and quantitative reasoning (−5.6; 95% CI: −11.4, 0.1). We observed unexpected positive associations between maternal occupational pesticide exposure with verbal (9.3; 95% CI: −8.5, 27.2), quantitative (8.6; 95% CI: −16.6, 33.8), and memory domains (8.9; 95% CI: −5.1, 22.8) among children, although these associations were imprecise. There were no clear differences in associations between boys and girls (see Supporting Information, Table S2). Among children whose mothers were exposed to any one EDC group during pregnancy, there was no clear pattern of associations. Compared to children of mothers with no EDC exposure during pregnancy, children whose mothers were exposed to any EDC group performed similarly, while those whose mothers were exposed to two or more EDC groups scored lower on most MCSA domains (Table 3).
Excluding poor-quality tests from the regression analyses did not change the overall pattern of results, although associations of exposure to alkylphenolic compounds and organic solvents with quantitative scales increased in magnitude, and positive effect estimates associated with pesticide exposure were slightly attenuated (see Supporting Information, Table S3).
Discussion
In this study, we examined the potential role of maternal JEM-based exposure to EDCs during pregnancy and offspring cognitive function in early childhood. To our knowledge, this study is the first to evaluate work-related exposure among pregnant women to certain endocrine disrupting compounds—namely, PAHs, phthalates, metals, and alkylphenolic compounds—in relation to childhood cognition. Although most associations were not statistically significant, the overall pattern of results suggests that maternal work-related exposure to EDCs is associated with lower childhood scores in several cognitive domains. We also observed a statistically significant relationship between organic solvent exposure and lower quantitative reasoning scores.
Some epidemiologic evidence exists regarding workplace exposure to solvents among pregnant women and their children’s neurodevelopment. Similar to our findings, previous studies have found little evidence of an association with overall cognitive function. However, in contrast with our findings, previous studies have observed impairments in verbal abilities associated with maternal solvent exposure. For example, Till et al.31 and Laslo-Baker et al.32 each conducted a small matched case–control study in Canada, in which children of solvent-exposed mothers—identified via a health counseling program for pregnant women—had poorer performance in language function and verbal memory, respectively, compared to unexposed children. More recently, among mother–child pairs in a French birth cohort, Costet et al.33 evaluated maternal urinary concentrations of glycol ethers and reported lower verbal comprehension scores at 6 years of age among children whose mothers had high urinary levels of glycol ether metabolites during pregnancy. Our results did not suggest impairment in children’s verbal abilities, rather, we observed that maternal occupational solvent exposure was associated with lower quantitative reasoning abilities, which were not specifically assessed in the previous literature.
Though we did not observe a statistically significant association between JEM-estimated maternal occupational exposure to alkylphenolic compounds and children’s quantitative reasoning abilities at age 5 years, this result could be considered of borderline statistical significance, although it is unclear whether signal may be due to confounding by co-exposure to solvents. To our knowledge, our study is the first to examine work-related exposure to alkylphenolic compounds among pregnant women and early child cognitive function, and only one publication has examined maternal environmental sources of exposure in relation to neurodevelopmental outcomes in children but did not find evidence of an association.34 Our findings support the need for more research on the potential neurodevelopmental impacts of occupational exposure to organic solvents and alkylphenolic compounds during pregnancy.
In addition to alkylphenolic compounds, to our knowledge, our study is the first to report on child cognition in relation to maternal occupational exposure to PAHs, phthalates, and metals. Studies of environmental exposure to these compounds during pregnancy have reported adverse effects on subsequent childhood cognitive function. For example, studies investigating ambient PAH exposure among pregnant women report delays in offspring intelligence that persist throughout childhood.10,35,36 Previous findings on neurodevelopmental effects of phthalates, while inconsistent, provide concerning evidence of cognitive impairments associated with environmental exposure during the prenatal period.9 Concerning metals, the prenatal period is a sensitive window of exposure for the neurotoxic effect of lead and mercury and perhaps other heavy metals with endocrine-disrupting properties.8 In our study, we observed statistically non-significant negative associations with maternal PAH and phthalate exposure, while contrary to our hypothesis, we observed positive associations of maternal exposure to metals with various domains of cognitive function. We also observed positive associations with maternal occupational exposure to pesticides—which has been associated with adverse effects on child intelligence in previous studies11,12,14—although these results should be interpreted with caution given the low exposure prevalence and imprecision of effect estimates. While our results are largely statistically non-significant, taken together, they show a pattern of poorer cognitive performance among children whose mothers were exposed during pregnancy to EDCs at their workplaces. Given that the workplace may be an important source of exposure to EDCs among certain occupational groups, more research is needed to further investigate associations with child neurodevelopment.
Notably, a substantial proportion of women with exposure to two or more EDC groups worked as hairdressers or barbers (19.8%) or domestic cleaners (57.5%), which is not surprising given the documented exposure to various chemicals among these occupational groups.37,38 Women employed as domestic cleaners accounted for 53 and 64% of those classified as exposed to organic solvents and alkylphenolic compounds, respectively. Among cleaners, cleaning products are the primary source of EDC exposure. For example, alkylphenol ethoxylate is a surfactant commonly found as an ingredient in detergents and all-purpose cleaners and has been shown to have adverse neurodevelopmental effects in rodents.39 Glycol ethers can be found as an active ingredient of heavy-duty surface cleaners. These and other organic solvents are known neurotoxicants among adult workers,40 and toxicological studies and clinical case reports have demonstrated that high levels of exposure to these compounds causes neurodevelopmental toxicity in exposed offspring, although the potential neurodevelopmental harm at lower levels of exposure is less clear.12 Although the specific mechanisms by which solvents and their metabolites may perturb brain development are not well understood, evidence from animal studies demonstrate that solvents can cross the placental barrier and fetal blood–brain barrier and that neurobehavioral abnormalities result from prenatal exposure, even at levels that cause no apparent maternal harm.41 Hairdressers have probable exposure to phthalates and parabens and possible exposure to alkylphenolic compounds and organic solvents through the use of cosmetic products, including dyes, sprays, and shampoos.6 Phthalates, in particular, are common ingredients in cosmetic products and may have negative impacts on the developing brain via disruptions in thyroid hormone homeostasis.42
Among women in our study population who worked as domestic cleaners or hairdressers, fewer had educational attainment beyond secondary school (7.3 and 12.1%, respectively)—a marker of lower socioeconomic status—compared to the overall study population (22.5%). Also, a greater proportion of women who were employed as cleaners were born outside of Spain (26%) compared to the overall population (6%). Given the potential for increased social vulnerability and burden of chemical exposures among these occupational groups, a direction for future work is to expand on previous research among these and related occupations—which has examined chronic adult health conditions and adverse birth outcomes13,37,43—to consider the potential impact of chemical exposures during pregnancy on developmental outcomes in their children.
Because most women who were classified as exposed to workplace chemicals had exposure to more than one EDC group, we cannot fully disentangle the independent effect estimates associated with each. We do, however, recognize that exposure to multiple chemicals more accurately reflects the reality of workplace exposures. Unfortunately, our study was not designed or powered to adequately examine the combined impact of multiple exposures. We report associations of maternal exposure to multiple EDCs, which are in line with our overall findings, such that children of women who were exposed to two or more EDC groups during pregnancy displayed worse performance in each domain of the MCSA (apart from motor skills).
The strengths of our study include the use of data from a prospective cohort study. Although attrition occurred, we were able to minimize any resulting selection bias by employing inverse probability weighting in our statistical analysis. Other advantages included the use of a standardized, psychologist-administered neurodevelopmental assessment, minimizing outcome misclassification, and detailed covariate information, allowing us to minimize potential confounding. Nonetheless, our study is subject to exposure misclassification. The JEM we applied assumes homogenous exposure for all members in each cell,44 and thus we were unable to account for differences in job tasks and work environments among individuals with the same job title. However, we expect exposure misclassification to be non-differential with respect to the outcome and thus bias our findings toward the null. In addition, the design of the JEM prioritizes sensitivity in exposure probability scores over specificity, thus it is likely that unexposed workers are misclassified as exposed, which may lead to underestimation of effect estimates. Notwithstanding this limitation of JEMs, they are still a valuable tool for exposure assessment in population-based studies in which occupational information is typically limited to job histories and industry and may have superior performance compared self-reported exposure information.45 In addition, although the JEM used in the present study can be refined to consider variations in exposure scenarios across time periods and countries for some job titles, data informing the risk of exposure within job titles and tasks, particularly for many of the prevalent job titles and exposures among INMA study participants, are limited. Additional research is needed to better characterize EDC exposure scenarios among specific occupations and tasks to further improve the value of a JEM in estimating work-related EDC exposures in population-based cohort studies. Other avenues for future work include the use of biomarkers of exposure to validate the JEM used in our study and the application of the JEM to population-based birth cohorts with larger study populations that are better powered to consider the combined impact of multiple workplace EDC exposures.
Our study should be interpreted considering additional limitations. Women in this study were likely exposed to EDCs through consumer goods and dietary sources, although we do not expect exposure levels in the general population to confound associations observed in this study, as it is unlikely that background concentrations of EDCs are associated with exposure in any given occupation. We cannot, however, rule out confounding due to other work-related chemical exposures not evaluated in the JEM. In addition, we did not consider other factors that may influence child neurodevelopment, including maternal psychiatric disorders, maternal gestational diabetes, or the postnatal diet of the child. However, we do not have evidence to suggest that these variables are associated with our JEM-based measures of EDC exposure and thus do not expect unmeasured confounding due to these variables. Lastly, we considered several domains of child cognitive function measured at age 5 years, but it is possible that child mental abilities at other ages are sensitive to maternal occupational EDC exposure. Further research is warranted that consider other aspects of neurodevelopmental function (e.g., behavior) at various developmental stages in relation to maternal occupational EDC exposures.
In conclusion, we found only limited evidence of a role of maternal work-related exposure to EDCs, estimated using a JEM, during pregnancy on early childhood cognitive function. Our results suggest that there may be an association between maternal organic solvents exposure and child quantitative reasoning skills, although further investigation is needed to confirm this finding. Our study also highlights the need to better characterize EDC exposures among pregnant women working in certain occupations.
Data availability
Data are owned by the INMA Project and are available upon reasonable request by contacting inma@proyectoinma.org. Information regarding the INMA Collaboration Policy is available here: https://www.proyectoinma.org/en/inma-project/inma-collaboration-policy/.
Change history
22 September 2022
A Correction to this paper has been published: https://doi.org/10.1038/s41390-022-02300-8
References
Gore, A. C. et al. EDC-2: The Endocrine Society’s Second Scientific Statement on Endocrine-Disrupting Chemicals. Endocr. Rev. 36, E1–E150 (2015).
Grandjean, P. & Landrigan, P. J. Neurobehavioural effects of developmental toxicity. Lancet Neurol. 13, 330–338 (2014).
Rice, D. & Barone, S. Critical periods of vulnerability for the developing nervous system: evidence from humans and animal models. Environ. Health Perspect. 108(Suppl 3), 511–533 (2000).
Eurostat. Employment rate by sex. https://ec.europa.eu/eurostat/web/products-datasets/-/tesem010 (2020).
Hines, C. J. et al. Urinary phthalate metabolite concentrations among workers in selected industries: a pilot biomonitoring study. Ann. Work Expo. Health 53, 1–17 (2008).
Brouwers, M. M., van Tongeren, M., Hirst, A. A., Bretveld, R. W. & Roeleveld, N. Occupational exposure to potential endocrine disruptors: further development of a job exposure matrix. Occup. Environ. Med. 66, 607–614 (2009).
Nesan, D. & Kurrasch, D. M. Gestational exposure to common endocrine disrupting chemicals and their impact on neurodevelopment and behavior. Annu. Rev. Physiol. https://doi.org/10.1146/annurev-physiol-021119-034555 (2019).
Sanders, A. P., Claus Henn, B. & Wright, R. O. Perinatal and childhood exposure to cadmium, manganese, and metal mixtures and effects on cognition and behavior: a review of recent literature. Curr. Environ. Health Rep. 2, 284–294 (2015).
Radke, E. G., Braun, J. M., Nachman, R. M. & Cooper, G. S. Phthalate exposure and neurodevelopment: a systematic review and meta-analysis of human epidemiological evidence. Environ. Int. 137, 105408 (2020).
Perera, F. P. et al. Prenatal airborne polycyclic aromatic hydrocarbon exposure and child IQ at age 5 years. Pediatrics 124, e195–e202 (2009).
Gonzalez-Alzaga, B. et al. A systematic review of neurodevelopmental effects of prenatal and postnatal organophosphate pesticide exposure. Toxicol. Lett. 230, 104–121 (2014).
Julvez, J. & Grandjean, P. Neurodevelopmental toxicity risks due to occupational exposure to industrial chemicals during pregnancy. Ind. Health 47, 459–468 (2009).
Zhu, J. L., Vestergaard, M., Hjollund, N. H. & Olsen, J. Pregnancy outcomes among female hairdressers who participated in the Danish National Birth Cohort. Scand. J. Work Environ. Health 32, 61–66 (2006).
Andersen, H. R., Debes, F., Wohlfahrt-Veje, C., Murata, K. & Grandjean, P. Occupational pesticide exposure in early pregnancy associated with sex-specific neurobehavioral deficits in the children at school age. Neurotoxicol. Teratol. 47, 1–9 (2015).
Marks, A. R. et al. Organophosphate pesticide exposure and attention in young Mexican-American children: the CHAMACOS study. Environ. Health Perspect. 118, 1768–1774 (2010).
Bouchard, M. F. et al. Prenatal exposure to organophosphate pesticides and IQ in 7-year-old children. Environ. Health Perspect. 119, 1189 (2011).
Vrijheid, M., Armstrong, B., Dolk, H., van Tongeren, M. & Botting, B. Risk of hypospadias in relation to maternal occupational exposure to potential endocrine disrupting chemicals. Occup. Environ. Med. 60, 543–550 (2003).
Snijder, C. A. et al. Occupational exposure to chemicals and fetal growth: the Generation R Study. Hum. Reprod. 27, 910–920 (2012).
Guxens, M. et al. Cohort profile: the INMA–INfancia y Medio Ambiente–(Environment and Childhood) Project. Int. J. Epidemiol. 41, 930–940 (2012).
Van Tongeren, M. et al. A job-exposure matrix for potential endocrine-disrupting chemicals developed for a study into the association between maternal occupational exposure and hypospadias. Ann. Occup. Hyg. 46, 465–477 (2002).
Office for National Statistics. Standard occupational classification 2000. Volume 1: Structure and descriptions of unit groups. https://www.ons.gov.uk/methodology/classificationsandstandards/standardoccupationalclassificationsoc/socarchive (2000).
CAMSIS. UK 2000 SOC to ISCO-88(COM) Social Interaction and Stratification Scale. http://www.camsis.stir.ac.uk/occunits/uksoc2000toisco88v3.sps (2005).
Birks, L. et al. Occupational exposure to endocrine-disrupting chemicals and birth weight and length of gestation: a European meta-analysis. Environ. Health Perspect. 124, 1785–1793 (2016).
McCarthy, D. MSCA: Escalas McCarthy de Aptitudes y Psicomotricidad Para Niños (TEA Ediciones, 2006).
Julvez, J., Forns, M., Ribas-Fito, N., Torrent, M. & Sunyer, J. Attention behavior and hyperactivity and concurrent neurocognitive and social competence functioning in 4-year-olds from two population-based birth cohorts. Eur. Psychiatry 26, 381–389 (2011).
IOM/NCR (Institute of Medicine/National Research Council Committee to Reexamine I. O. M. Pregnancy Weight Guidelines). Weight Gain During Pregnancy: Reexamining the Guidelines (eds Rasmussen, K. M. & Yaktine, A. L.) (National Academies Press, 2009).
Wechsler, D. & Kaufman, A. WAIS-III. Escala de Inteligencia de Wechsler Para Adultos (III) (Tea Ediciones, 2001).
Weisskopf, M. G., Sparrow, D., Hu, H. & Power, M. C. Biased exposure-health effect estimates from selection in cohort studies: are environmental studies at particular risk? Environ. Health Perspect. 123, 1113–1122 (2015).
McCarthy, M. M. & Nugent, B. M. Epigenetic contributions to hormonally-mediated sexual differentiation of the brain. J. Neuroendocrinol. 25, 1133–1140 (2013).
Sood, S., Shekhar, S. & Santosh, W. Dimorphic placental stress: a repercussion of interaction between endocrine disrupting chemicals (EDCs) and fetal sex. Med. Hypotheses 99, 73–75 (2017).
Till, C., Koren, G. & Rovet, J. F. Prenatal exposure to organic solvents and child neurobehavioral performance. Neurotoxicol. Teratol. 23, 235–245 (2001).
Laslo-Baker, D. et al. Child neurodevelopmental outcome and maternal occupational exposure to solvents. Arch. Pediatrics Adolesc. Med. 158, 956–961 (2004).
Costet, N. et al. Occupational exposure to organic solvents during pregnancy and childhood behavior: findings from the PELAGIE birth cohort (France, 2002-2013). Environ. Health. 17, 63 (2018).
Lin, C. C. et al. Prenatal phenolic compounds exposure and neurobehavioral development at 2 and 7 years of age. Sci. Total Environ. 605–606, 801–810 (2017).
Jedrychowski, W. A. et al. Prenatal exposure to polycyclic aromatic hydrocarbons and cognitive dysfunction in children. Environ. Sci. Pollut. Res. Int. 22, 3631–3639 (2015).
Edwards, S. C. et al. Prenatal exposure to airborne polycyclic aromatic hydrocarbons and children’s intelligence at 5 years of age in a prospective cohort study in Poland. Environ. Health Perspect. 118, 1326–1331 (2010).
Quiros-Alcala, L., Pollack, A. Z., Tchangalova, N., DeSantiago, M. & Kavi, L. K. A. Occupational exposures among hair and nail salon workers: a scoping review. Curr. Environ. Health Rep. 6, 269–285 (2019).
Gerster, F. M., Vernez, D., Wild, P. P. & Hopf, N. B. Hazardous substances in frequently used professional cleaning products. Int. J. Occup. Environ. Health 20, 46–60 (2014).
Acir, I.-H. & Guenther, K. Endocrine-disrupting metabolites of alkylphenol ethoxylates - a critical review of analytical methods, environmental occurrences, toxicity, and regulation. Sci. Total Environ. 635, 1530–1546 (2018).
Dick, F. D. Solvent neurotoxicity. Occup. Environ. Med. 63, 221–6, 179 (2006).
Rock, K. D. & Patisaul, H. B. Environmental mechanisms of neurodevelopmental toxicity. Curr. Environ. Health Rep. 5, 145–157 (2018).
Miodovnik, A., Edwards, A., Bellinger, D. C. & Hauser, R. Developmental neurotoxicity of ortho-phthalate diesters: review of human and experimental evidence. Neurotoxicology 41, 112–122 (2014).
European Agency for Safety and Health at Work. The Occupational Safety and Health of Cleaning Workers (European Agency for Safety and Health at Work, 2009).
Kromhout, H., Symanski, E. & Rappaport, S. M. A comprehensive evaluation of within- and between-worker components of occupational exposure to chemical agents. Ann. Occup. Hyg. 37, 253–270 (1993).
Delclos, G. L., Gimeno, D., Arif, A. A., Benavides, F. G. & Zock, J.-P. Occupational exposures and asthma in health-care workers: comparison of self-reports with a workplace-specific job exposure matrix. Am. J. Epidemiol. 169, 581–587 (2009).
Acknowledgements
The authors would like to thank all the participants in this study for their generous collaborative efforts.
Funding
This work was supported by grants from the National Institutes of Health/National Institute of Environmental Health Sciences (R01ES028842), Instituto de Salud Carlos III (Red INMA G03/176, CB06/02/0041; FIS-FEDER: PI03/1615, PI04/1509, PI04/1112, PI04/1931, PI05/1079, PI05/1052, PI06/0867, PI06/1213, PI07/0314, PI09/02647, PI11/01007, PI11/02591, PI11/02038, PI13/1944, PI13/2032, PI14/00891, PI14/01687, PI16/1288, PI17/00663, FIS-PI18/01142 incl. FEDER funds; Miguel Servet-FEDER CP11/00178, CP15/00025, CPII16/00051, CPII18/00018, and CP16/00128), Generalitat de Catalunya-CIRIT 1999SGR 00241, EU Commission (FP7-ENV-2011 cod 282957 and HEALTH.2010.2.4.5-1), Generalitat Valenciana: FISABIO (UGP 15-230, UGP-15-244, and UGP-15-249) and Conselleria d’Educació AICO/2020/285, and Alicia Koplowitz Foundation 2017, Department of Health of the Basque Government (2005111093), Provincial Government of Gipuzkoa (DFG06/002), and annual agreements with the municipalities of the study area (Zumarraga, Urretxu, Legazpi, Azkoitia y Azpeitia y Beasain). We also acknowledge support from the Spanish Ministry of Science and Innovation and the State Research Agency through the “Centro de Excelencia Severo Ochoa 2019-2023” Program (CEX2018-000806-S), and support from the Generalitat de Catalunya through the CERCA Program. J.I., D.G.R.d.P., and G.L.D. are partly supported by the Southwest Center for Occupational and Environmental Health (SWCOEH), the Centers for Disease Control and Prevention (CDC) National Institute for Occupational Safety and Health (NIOSH) Education and Research Center (T42OH008421) at The University of Texas Health Science Center at Houston (UTHealth) School of Public Health. K.W.W. and E.S. are supported in part by the by the Gulf Coast Center for Precision Environmental Health (GC-CPEH) at Baylor College of Medicine (P30ES030285).
Author information
Authors and Affiliations
Contributions
J.I. led the planning of the study, statistical analysis, interpretation of data, and drafting of the manuscript with substantial contributions and critical review from D.G.R.d.P., K.W.W., G.L.D., M.D.S., and E.S. K.W.W., E.S., and D.G.R.d.P. significantly contributed to the design of the study, supervision, and interpretation of data. M.G., M.C., J.M.I., A.L., C.I., and M.R. contributed to the design and/or conduct of the INMA Project, acquisition of data, and critically reviewed the manuscript for intellectual content. All authors read and approved the final manuscript and agree to be accountable for all aspects of the work.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
All participants gave written informed consent prior to enrollment in the IMNA Project study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The sample sizes listed for each category of exposure to multiple chemical groups did not accurately reflect the number of participants included in the model and have been adjusted in Table 3 and in the text. The exposure prevalence stated in the abstract was also corrected.
Supplementary information
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Ish, J., Symanski, E., Gimeno Ruiz de Porras, D. et al. Maternal occupational exposure to chemicals and child cognitive function. Pediatr Res 92, 1153–1160 (2022). https://doi.org/10.1038/s41390-022-02089-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-022-02089-6
This article is cited by
-
Association between prenatal exposure to alkylphenols and intelligence quotient among preschool children: sex-specific effects
Environmental Health (2024)
-
Imperative to accelerate research aligning real-time clinical demand with mental health supply
Pediatric Research (2022)
