
Abstract
Background
The aim of this study was to investigate the influence of early-life pain/stress and medical characteristics on neurobehavioral outcomes in preterm infants.
Methods
A prospective cohort study was conducted with 92 preterm infants (28–32 weeks gestational age [GA]). Early-life pain/stress was measured via the Neonatal Infant Stressor Scale (NISS) during the first 28 days of NICU hospitalization. Neurobehavioral outcomes were evaluated using the NICU Network Neurobehavioral Scale at 36–38 weeks post-menstrual age. Functional regression and machine learning models were performed to investigate the predictors of neurobehavioral outcomes.
Results
Infants experienced daily acute pain/stress (24.99 ± 7.13 frequencies) and chronic events (41.13 ± 17.81 h). Up to 12 days after birth, both higher acute and chronic NISS scores were associated with higher stress scores; and higher chronic NISS scores were also related to lower self-regulation and quality of movement. Younger GA predicted worse neurobehavioral outcomes; GA < 31.57 weeks predicted worse stress/abstinence, self-regulation, and excitability; GA < 30.57 weeks predicted poor quality of movement. A higher proportion of maternal breastmilk intake predicted better self-regulation, excitability, and quality of movement in older GA infants.
Conclusions
Preterm infants are vulnerable to the impact of early-life pain/stress. Neurobehavioral outcomes are positively associated with increased GA and higher maternal breastmilk intake.
Impact
-
During the first 12 days of life, preterm infant neurobehavioral outcomes were vulnerable to the negative impact of acute and chronic pain/stress. Future research is warranted to investigate the long-term effects of early-life pain/stress on neurobehavioral outcomes.
-
Gestational age remains one of the critical factors to predict neurobehavioral outcomes in preterm infants; older gestational age significantly predicted better neurobehavioral outcomes.
-
Feeding with a higher proportion of maternal breastmilk predicted better neurobehavioral outcomes. Future research is warranted to investigate how maternal breastmilk may buffer the negative effects of early-life pain/stress on neurobehavioral outcomes.
Similar content being viewed by others
The survival rate of preterm infants has improved with advances in prenatal and neonatal care.1,2,3,4,5 However, up to 90% of preterm infants are admitted to the Neonatal Intensive Care Unit (NICU).6,7,8,9,10,11 These infants are subjected to numerous medically necessary but painful diagnostic and therapeutic procedures, and also exposed to stressful routine handling and touching, such as changing position, diaper change, mouth care, and bottle-feeding, which are not usually considered as “harmful” for the infants.6,7,8,9,10,11 Such cumulative pain/stress is exacerbated by the prolonged NICU stay with other adversities, e.g., maternal–infant separation, hypoxia, infection, and feeding difficulties. Altogether, they may lead to altered hormonal (cortisol) and physiologic (heart rate, blood pressure, respiratory rate, and oxygen saturation) responses and chronic stimulation of neuronal pain pathway (nociception) and stress.12 Thus, these early-life experiences result in a high risk of neurobehavioral deficits and chronic mental illnesses (e.g., anxiety, depression, eating disorders) and metabolic illness (e.g., obesity, diabetes, cardiovascular diseases) later in life.13,14,15,16 However, there are still unknown factors in unraveling the short- and long-term impact of early-life pain/stress on the programming of infant neurobehavioral outcomes.
Compared to adults and older children, preterm infants may have a lower pain threshold and pain tolerance that pose a different level of risk based on their birth gestational age (GA).17 Of note, the nociceptive nerve endings begin to develop at 7 weeks of GA, and are functional by week 30, allowing the fetus to localize and reflexively withdraw from painful stimuli.18 Myelin sheath begins to develop after 25 weeks of GA and is completed by week 37, acting as an electrical insulator and increasing the speed of a signal from the peripheral to the central nervous system.19 Depending on the birth GA and status of pain pathway development, preterm infants may experience pain differently. They are highly sensitive to repeated and prolonged pain/stress stimulation.6,12 For example, preterm infants have lower flexor reflex thresholds and poor localization and discrimination of sensory input, thus they experience prolonged hyperalgesia (enhanced sensitivity to pain) and allodynia (pain from stimuli that is not normally painful). Meanwhile, due to low tactile threshold and immature descending inhibitory pathways, even routine handling and touching may elicit significant pain/stress responses in preterm infants.6,12 It is still unclear how pain stimuli may affect preterm infants, when the pain pathway is not fully developed, especially those born less than 32 weeks of GA.
Despite the potential “harm” from pain/stress induced by routine care or medical procedures, preterm infants continue to receive inadequate pain alleviation during approximately 50% of their daily procedures.5,6,20,21 During a mean of 8 days NICU hospitalization, infants experienced a mean number 16 heel sticks and 4 venipunctures without routine analgesia.6 A study in 430 neonates revealed that approximately 80 painful procedures were performed without specific analgesia.5 Preterm infants may not be able to demonstrate robust behavioral responses to pain/stress due to their prematurity. Thus, subtle or absent behavioral responses may contribute to insufficient pain assessment and inadequate pain management. Inadequate comfort or pain alleviation may lead to decreased oxygenation, bradycardia or tachycardia, sleep disruption, behavioral agitation, hemodynamic and physiologic instability, or increased intracranial pressure.8,22,23 These unalleviated short-term pain/stress events may further contribute to long-term reduced anthropometric growth and negative developmental sequelae.
Evidence suggests growing concerns over the deleterious effects of repeated early-life pain/stress on the neurobehavioral outcomes of preterm infants. The brain structure and function are established during early periods of development in utero.13 During these neuroplasticity periods, brain development is highly susceptible to positive and negative experiences, which are theorized to build the foundation for future health and behaviors.13 For example, researchers showed that preterm infants who received 60 min up to 150 min kangaroo care (skin-to-skin holding) daily by their mothers demonstrated higher neurobehavioral scores compared to the control group over time.24,25 Mothers who directly breastfeed their infants also facilitate skin-to-skin contact and its benefits, thus, breastfeeding is considered the gold standard for infant care.26 On the other hand, recurrent early-life pain/stress during neuroplasticity periods may repeatedly activate a cascade of stress signaling, leading to poor growth and brain development. For instance, maternal–infant separation, a source of early-life stress, prevents important neural processes from taking place and leads to a permanently elevated stress system.27 Researchers also demonstrated a correlation between higher early skin-breaking procedures with lower head circumference15 and brain dysmaturation at 32 weeks post-menstrual age (PMA) and term equivalent,5,12,14,16,28 including reductions in thalamus volume, white matter, and gray matter,14 and frontal and parietal brain width.16,28 Of note, early-life pain/stress is also shown to impact long-term brain development, motor, visual, and cognitive.5 For example, in school-age children who were born prematurely, greater exposure of early-life pain/stress was predictive of the thinner cortex and smaller regional volumes in the limbic system and basal ganglia,12 and decreased cortical thickness and reduced cerebellar volumes.29,30 Such impairments in brain development are associated with adverse behavioral outcomes later in life (8 months corrected age to school-age),5 e.g., poor cognitive and motor development15,31 and altered affective and internalizing behaviors.10,32,33 Research has begun investigating the linkage between early-life pain/stress and neurobehavioral outcomes later in life. However, such associations during NICU hospitalization are underdeveloped. Little is known about the extent to which early-life pain/stress may impact how preterm infants exhibit neurobehaviors during early neurobehavioral examinations.
We hypothesized that preterm infants exposed to early-life pain/stress would develop altered neurobehavioral outcomes at 36 to 38 weeks PMA. The purpose of the study was to: (1) describe acute and chronic early-life pain/stress during the first 28 days of NICU hospitalization, (2) describe the neurobehavioral outcomes at 36–38 weeks PMA, and (3) investigate the influence of multiple factors including early-life pain/stress and infant medical characteristics on neurobehavioral outcomes in preterm infants during NICU hospitalization.
Methods
Design
A prospective cohort study design was employed to examine the association between early-life pain/stress during the first 28 days, infant medical characteristics, and neurobehavioral outcomes in a selected cohort of preterm infants during NICU hospitalization. Standard care was provided to all infants during their NICU hospitalization. The study was approved by the Institutional Review Boards of the study institutes.
Settings and participants
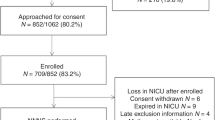
Ninety-two preterm infants were recruited from two Level IV NICUs in the Northeastern U.S. Inclusion criteria were preterm infants: (1) born between 28 and 33 weeks GA, (2) admitted to the NICU within 0–3 days after birth, and (3) with English or Spanish speaking parents who were ≥18 years to give consent. Exclusion criteria were infants having: (1) known congenital defects, (2) intraventricular hemorrhage (grades III and IV), (3) invasive surgery, and (4) maternal substance exposure history.6
Measurements
Demographic characteristics
Demographic characteristics were collected from electronic medical records, including the infant’s sex and maternal race/ethnicity, marital status, education level, and age.
Infant medical characteristics
Infant medical characteristics included GA, delivery type, premature rupture of membrane (PROM), growth parameters, Scale of Neonatal Acute Physiology with Perinatal Extension-II, and the length of hospitalization. We also collected the total number of daily feedings (up to 8 times per day), and the frequency of maternal breastmilk given to the infant each shift. We then calculated the daily proportion of maternal breastmilk given its frequency over the total number of daily feedings.
Early-life pain/stress
Early-life pain/stress was categorized as acute and chronic. We assessed acute and chronic pain/stress during the first 28 days of NICU hospitalization using the modified Neonatal Infant Stressor Scale (NISS).6 We adapted and validated the Australia version instrument34 based on the NICU settings in the USA.35 The early-life pain/stress was assessed by 47 acute events (e.g., diaper changes, x-ray, intravenous (IV) injection, etc.) and 23 chronic events [e.g., intranasal oxygen, nil per os, etc.].35 The acute and chronic pain/stress events were categorized into five severity levels (2 = “a little” to 5 = “extreme”). Detailed events of each pain/stress level are given in Supplementary Material. The principal investigator randomly audited the completed early-life pain/stress data for 20% of infants in the study and confirmed 95% agreement.
We calculated the total and average daily acute and chronic pain/stress, for each subject. Average daily pain/stress for the first, second, third, and fourth week after birth was calculated by adding weekly frequencies (for acute) and hours (for chronic) of pain/stress events and then divided by 7 days each week. Total scores of pain/stress were calculated by adding frequencies (for acute) and hours (for chronic) of pain/stress events over 28 days. We assigned acute pain/stress of levels 2 and 3 as the expected standard care in the NICU, while levels 4 and 5 were considered “very” and “extreme” pain/stress events.36
Neurobehavioral outcomes
Neurobehavioral outcomes were evaluated via the NICU Neonatal Neurobehavioral Scale (NNNS)37,38 when the infant reached 36–38 weeks PMA.6 The NNNS is a standardized neurobehavioral assessment that provides an assessment of neurological integrity and behavioral function at 34–48 weeks PMA. The three main sections of NNNS are (1) neurological items for tone and reflexes, (2) behavioral items for state, sensory, and interactive processes, and (3) stress/abstinence-related items. The NNNS includes a total of 115 items and generates 13 summary scores. As the scope of the study was related to early-life pain/stress, our study analyses focused on four NNNS summary scores: stress/abstinence (NSTRESS), self-regulation (NREGULATION), quality of movement (NQMOVE), and excitability (NEXCITABILITY). The NSTRESS is based on signs of stress observed throughout the examination, including physiological, autonomic, central nervous system, skin, visual, gastrointestinal, and state. Higher NSTRESS indicates more stressful behavioral signs. The NREGULATION combines physiological, motor, and attentional activation. Higher NREGULATION indicates the better regulation ability of the infant to cope during the examination. The NQMOVE measures smoothness, maturity, modulation of movement of the limbs, startles, and tremors. Higher NQMOVE indicates less tremoring, startles, no jitteriness, and mature movement. The NEXCITABILITY measures levels of motor, state, and physiologic reactivity. Higher NEXCITABILITY indicates more irritability in response to handling during assessment and more difficulty to soothe by the assessors.
Procedure
Parents provided informed consent for their infants’ participation in the study. Data of demographic characteristics, infant medical characteristics, and pain/stress events during the first 28 days of NICU hospitalization were collected from electronic medical records. The neurobehavioral examination was administered when the infant reached 36–38 weeks PMA using the NNNS. The examination took place in a quiet room with the infant initially asleep and was completed in 30 min. The examination was administered by a neonatal developmental specialist in the NICU, who has been trained and certified for using the NNNS. The examiner was blinded to the infants’ history and health characteristics to control for examiner bias. Parents were encouraged to stay with infants during the examination.
Data analysis
Data were managed and analyzed using REDCap39 and R 4.1.0.40 Descriptive analyses described the demographic characteristics, infant medical characteristics, NISS, and NNNS score. Comparison of all variables was done between male and female infants, and p values for the difference between sex groups were calculated using the Mann–Whitney test for continuous variables and the Fisher’s Exact test for categorical variables. We also included a range for each NNNS summary score.
To examine the time-varying relationship between NNNS summary scores (scalar outcomes) and densely collected early-life pain/stress at NICU (functional predictors), we adopted a machine learning method for estimating functional regression models using the “FDboost” package in R.41 The functional regression models allow us to investigate the non-linear effect of the longitudinal pain/stress measures on each NNNS summary score over the NICU hospitalization. In each of the functional regression models, an NNNS summary score was considered the scalar outcome. Daily severe acute pain/stress (level 4 and level 5), daily chronic pain/stress, and daily proportion of maternal breastmilk were considered as functional predictors on the domain of postnatal days. To adjust the potential confounding effects, baseline characteristics, including birth GA, sex, delivery type, and PROM, were treated as scalar predictors with time-invariant effect on the NNNS summary scores. For the functional predictors, the non-linear effect was obtained by the base learners of cubic spline basis with the second-order penalty and 10 knots. Bootstrap confidence bands of the non-linear coefficients for the functional predictors were estimated using 1000 bootstrap samples.
We further applied the conditional inference tree (CTree)42 to identify the predictors of neurobehavioral outcomes. Specifically, a CTree model was constructed for each of the NNNS scores as an outcome variable. The birth GA, the daily proportion of maternal breastmilk, and daily average acute and chronic pain/stress at NICU were considered as predictors under each of the CTree models. The null hypothesis at the partition of each node was rejected if the corresponding p-value was less than 0.05. We conducted this regression tree analysis using the package “Partykit” in R.42
Results
Demographic characteristics
Ninety-two preterm infants were recruited in the study, with 55.4% female, 80.43% non-Hispanic, and 72.83% white. Demographic characteristics are summarized in Table 1.
Infant medical characteristics
The infant medical characteristics are summarized in Table 2. The mean GA was 30.64 weeks (SD = 1.86), and the length of hospital stay was 49 days (SD = 26.54). Male infants were older in GA (mean = 31.09, SD = 1.77) than female infants (mean = 30.28, SD = 1.87), p = 0.04. The infant feeding pattern is shown in Fig. 1. We observed an increase in the proportion of maternal breastmilk and a decrease in human donor milk and formula during the first 28 days.

The curve represents the daily averaged frequency of feeding types (i.e., maternal breastmilk, donor breastmilk, and formula).
Early-life pain/stress
Figure 2 shows the unweighted weekly mean acute and chronic pain/stress during the first 28 days of NICU hospitalization. For acute pain/stress, infants had a total mean frequency of 614.12 events (SD = 214.84) during the first 28 days and a daily mean frequency of 24.99 events (SD = 7.13). Of note, the total mean frequency of level 3 acute pain/stress was 18.57 events (SD = 4.27) and accounted for 74.29% of all acute pain/stress. Daily mean frequency of level 2 and 3 acute pain/stress increased while level 4 and level 5 decreased during the first 28 days of NICU hospitalization (Fig. 2a). For chronic pain/stress, infants had a total mean of 1023.65 h (SD = 493.03) and a daily mean of 41.13 h (SD = 17.81) during the first 28 days. Of note, the total mean of level 2 chronic pain/stress was 32.93 h (SD = 11.60) and accounted for 80.07% of all chronic pain/stress. The daily mean (hours) of all 3 chronic pain/stress levels decreased over time (Fig. 2b).

a Daily averaged acute pain/stress frequency by week. b Daily averaged accumulated chronic pain/stress hours by week.
Neurobehavioral outcomes
NNNS scores were obtained from infants and summarized in Table 3. There was no significant difference between males and females.
Factors associated with neurobehavioral outcomes
Using the machine learning method, we found that the acute and chronic early-life pain/stress had different patterns of association with NNNS summary scores (NSTRESS, NREGULATION, and NQMOVE) over the first 17 postnatal days (Fig. 3). During 4–12 postnatal days, both higher acute pain/stress and chronic pain/stress were associated with higher NSTRESS (Fig. 3a1, a2). However, during 12–17 postnatal days, no association was noted for acute pain/stress and NSTRESS, while higher chronic pain/stress was associated with lower NSTRESS. The pattern of the association between acute pain/stress with NREGULATION was not clear since the estimated time-varying effect was flat (y = 0) over time (Fig. 3b1). During 5–10 postnatal days, higher chronic pain/stress was associated with lower NREGULATION (Fig. 3b2). However, during 13–17 postnatal days, higher chronic pain/stress was associated with higher NREGULATION. Before 12 postnatal days, there was no significant evidence for the association between acute pain/stress and NQMOVE (Fig. 3c1), but during 12–17 postnatal days, higher acute pain/stress was associated with lower NQMOVE. During 4–9 postnatal days, higher chronic pain/stress was associated with lower NQMOVE (Fig. 3c2), but during 13–17 postnatal days, higher chronic pain/stress was associated with higher NQMOVE.

The non-linear effect of acute and chronic pain/stress on NSTRESS (a1, b2), NREGULATION (b1, b2), and NQMOVE (c1, c2) during the first 17 postnatal days. The black solid curves represent the estimated time-varying effect of pain/stress on the neurobehavioral outcomes. A positive value (above the horizontal dashed line y = 0) indicates an increasing effect on the neurobehavioral outcomes at a certain time point, and vice versa. The red dashed curves show the 95% bootstrap confidence bands of the estimates. The more deviated from the horizontal dashed line at y = 0, the stronger evidence for an increasing/decreasing impact of the pain/stress on the neurobehavioral outcomes at the certain period. Each of the gray solid curves represents the estimate from each bootstrap sample.
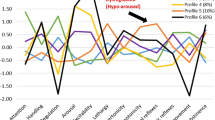
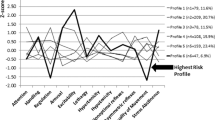
Figure 4 illustrates results of CTree models for partitioning the preterm infants into the subgroups with NNNS summary scores, NSTRESS (Fig. 4a), NREGULATION (Fig. 4b), NQMOVE (Fig. 4c), and NEXCITABILITY (Fig. 4d). Birth GA was an essential factor to influence neurobehavioral outcomes. The infants were partitioned based on the birth GA at 31.57 weeks to two subgroups with different NSTRESS (p < 0.001), NREGULATION (p < 0.001), and NEXCITABILITY (p = 0.048), while the cut-off GA for NQMOVE (p = 0.007) was at 30.57 weeks. Infants in the subgroup with younger GA had higher NSTRESS (mean = 0.23 vs. mean = 0.14), lower NREGULATION (mean = 4.34 vs. mean = 5.15), lower NQMOVE (mean = 3.71 vs. mean = 4.16), and higher NEXCITABILTIY (mean = 4.07 vs. mean = 2.83). Of note, within the older GA subgroups, the proportion of maternal breastmilk was also a significant predictor of neurobehavioral outcomes. In the subgroup with GA older than 30.57 weeks, infants demonstrated higher NQMOVE (mean = 4.72 vs. mean = 4.01, p = 0.041) when receiving a higher than 92.3% proportion of maternal breastmilk. In the subgroup with GA older than 31.57 weeks, infants demonstrated higher NREGULATION (mean = 5.66 vs. mean = 4.80, p = 0.042) when receiving higher than 75.4% proportion of maternal breastmilk; and lower NEXCITABILITY (mean = 2.10 vs. mean = 4.30; p = 0.039) when receiving higher than 44.2% proportion of maternal breastmilk.

Conditional inference trees for NNNS scores: a NSTRESS, b NREGUALTION, c NQMOVE, and d NEXCITABILITY. MBM maternal breastmilk.
Discussion
As part of the routine and life-saving interventions, preterm infants are exposed to considerable procedural pain-related stress during weeks to months of hospitalization in the NICU.7 Using computer algorithms, we found an association between the acute and chronic pain/stress and NNNS during the first 17 postnatal days. We also observed that older GA and infants fed a higher proportion of maternal breastmilk were associated with significantly better neurobehavioral outcomes. To the best of our knowledge, this is the first study where machine learning models were applied to assess the early-life risk factors of neurobehavioral outcomes in preterm infants during their NICU hospitalization. Machine learning has been widely accepted as a research tool because of its accuracy and efficiency in analyzing complex medical data to predict potential risks.43
In our study, over a 28-days observational period, medically stable preterm infants may receive up to 59 acute procedures daily, including changing position, changing the diaper, mouth care, bottle-feeding, nasal suction, etc. In addition, infants would endure up to 18 h of chronic procedures daily, such as nasogastric/orogastric tube, IV line, phototherapy, etc. Many procedures that are part of essential daily handling, however, have been shown to be associated with pain/stress and physiological instability.12 Research showed that even clustered nursing care, which is routinely done in the NICU to limit stress exposure, was associated with physiological instability.44 Physical handling of the baby was probably the major component of this stress because, in the same study, researchers found that standardized neurobehavioral assessments that required physical handling caused more physiologic instability (e.g., tachycardia, heart rate instability) than one that did not require handling.44 In recognition of this fact, strategies such as ambient sound and light modifications, kangaroo care, behavioral supports during stressful procedures, “no-touch times” and non-nutritive sucking are currently being applied in our NICU. However, more needs to be done to ensure adequate recognition, assessment, and interventions to mitigate the effect of pain/stress in the NICU, and the noxious effects of these on neurodevelopment need further evaluation in the future.
Research has begun to shed light on neurobehavioral outcomes in infants using the NNNS, however, there are limited published norms of NNNS for preterm infants. The NNNS summary scores of the current study (Table 3) were within the range of previous studies of preterm infants.6,37 On the other hand, compared to full-term infants, our NNNS summary scores exhibited a higher trend for the following items: stress/abstinence, excitability, need for handling, non-optimal reflexes, lethargy; and lower scores in self-regulation, quality of movement, habituation, attention, arousal.45
We observed an association between the chronic early-life pain/stress and the summary scores of NNNS, in the domains of stress/abstinence, self-regulation, and quality of movement. Overall, during the first 12 postnatal days, higher chronic stress was significantly associated with more stressful behavioral signs, lower regulation ability, more tremors, startles, jitteriness, and less mature movement.46 We observed a reversed trend during 13–17 postnatal days, in the observation that higher chronic early-life pain/stress was associated with less stressful behavioral signs. Our findings suggest that infants are especially vulnerable to stress/pain during the first 12 postnatal days. Rantakari et al. found that hypoxic stress was correlated with abnormal neurobehavioral outcomes in preterm infants at their first 3 days of life.47 Nist et al. discovered that cumulative stress exposure over the first 14 days of life predicted later neurobehavioral deficits in preterm infants.48 The vulnerable period in the first 12 postnatal days, identified in this study, is supportive of the concept of early-life critical periods of neuroplasticity. During this period, the brain and its associated neurodevelopment in preterm infants are especially vulnerable to noxious stimuli as evidenced by reduced gray matter volumes, disrupted white matter proliferation, and alterations in synaptic pruning.49 Hence, higher chronic stress during the first 12 postnatal days may result in less optimal neurobehavioral outcomes. Additionally, the patterns of associations between chronic pain/stress and neurobehavioral outcomes in our study may be elucidated by the maturation of infant. Complex neurodevelopment begins as early as 2nd month of gestation as evidenced by the proliferation of radial glia and neurons and continues until 3 years of age.50 Viable preterm births can occur between 22 and 36 weeks of gestation. This period is marked by extreme neurobehavioral dynamics in physiologic, structural, and functional processes.13,51 Therefore, the consequences of prematurity on neurodevelopment can be numerous and diverse. We speculate that the disruption of intrauterine neurodevelopment due to an abrupt premature birth may induce disturbances in physiologic, structural, and functional processes of the immature neural networks, thus making preterm infants more vulnerable to chronic pain/stress during the first 12 postnatal days. We further speculate that after 12 days, the pain/stress response system in preterm infants may begin to adapt to the external environment. These adaptive changes may allow infants to buffer the negative effects of chronic pain/stress and exhibit appropriate neurobehavioral responses.
Additionally, during the first 12 postnatal days, higher acute stress was associated with more stressful behavioral signs; but no associations were found with the domains of regulation ability and quality of movement. We observed that acute pain/stress between 12 and 17 days was associated with less mature movements. The differences between acute and chronic pain are many and varied. Physiologically, they are perceived and processed via different brain regions and neuronal pathways; and as such could be considered different entities.52 Our findings indicate that preterm infants are more susceptible to the negative impacts of acute and chronic early-life pain/stress, especially during the first 12 postnatal days. Thus, strategies designed to protect infants from such influences during the first 12 postnatal life should be prioritized.
In addition, we found that infants who were born younger than 31 weeks and 4 days GA had higher stress/abstinence and excitability, lower self-regulation, and poorer quality of movement. These younger preterm infants had higher signs of stress and were more prone to the motor, state, and physiologic reactivity. In contrast, older preterm infants had more organized behaviors in response to stimulation while demonstrating more smooth and mature movements, and absence of startle and tremors. We speculate that the reason may be that younger preterm infants often have more medical complications and are more often exposed to a higher number of life-saving but painful procedures. This early-life pain/stress exposure in preterm infants, in turn, exerts numerous negative effects on neurobehavioral outcomes.7,46,53 It is well known that lower GA is negatively associated with infant survival.54 Therefore, it is not surprising that worse NNNS scores and neurodevelopment were correlated with lower GA probably because of infants’ poor ability to handle environmental stress.55 Our findings support that younger preterm infants are at higher risk for adverse neurobehavioral outcomes compared to older preterm and full-term infants.
As demonstrated in our study, intake of maternal breastmilk may buffer the effects of acute and chronic pain/stress on neurobehavioral outcomes. We found that infants who received a higher proportion of maternal breastmilk had higher self-regulation, higher quality of movement, and lower excitability. We had previously shown that increased duration of skin-skin contact and direct breastfeeding provided to premature infants, was associated with better habituation responses at 36–37 weeks PMA.6 The various benefits of breastmilk compared to the formula for early brain development have been well researched.56 Specifically, preterm infants fed breastmilk had better white matter development and cortical thickness of the brain structure.57 Even infants who received breastmilk at 34–41 weeks PMA demonstrated better orientation, which suggests better visual and auditory attention to people and objects.58 It is important to note that infants who received maternal breast milk had better neurobehavioral outcomes compared to infants who received donor breastmilk.59 The effect on preterm infant neurobehavioral outcomes of the type and volume of breastmilk received can be sustained into childhood.57 In a recent literature review, researchers concluded that maternal breastmilk may offer protection against severe morbidities such as necrotizing enterocolitis, late-onset sepsis, and retinopathy of prematurity.60 Such protection will nurture optimal health, growth, and development in premature infants. Our findings confirm the importance of maternal breastmilk for fostering optimal neurobehavioral outcomes in preterm infants.61 However, further investigation to understand the mechanisms underlying the use of maternal breastmilk and its association with early-life pain/stress and neurobehavioral outcomes needs to be a clinical priority.
There are several limitations to the study. The older GA of males compared with females was a confounder in our study, and we had to control for sex and GA factors in our statistical analysis. Some early-life painful events might not have been captured in the NICU due to incomplete documentation; in addition, our NISS data were limited to the first 28 days after birth. Additionally, participants in our research only reflected the diversity of race and education level of the northeastern area of Connecticut. These issues may limit the generalizability of our study findings. For the functional regression models using machine learning algorithms, there were no available inferential statistics, so the 95% confidence bands were based on a bootstrap method, and are essentially descriptive. Due to the small sample size of the study, the multiplicity adjustment was not adopted for the recursive partitioning algorithm in the machine learning models. In the future, a comprehensive study with a larger sample size will be required to verify the adequacy of the cut-off points obtained by the machine learning models.
Acute and chronic early-life pain/stress is inevitable in the NICU and exerts negative influences on neurobehavioral outcomes. Follow-up studies are warranted to investigate how early-life pain/stress is related to long-term neurobehavioral outcomes in preterm infants. Typically, neurobehavioral outcomes are evaluated when infants are relatively mature and medically stable. Thus, there might be an extensive gap between birth, and adequate neurobehavioral assessment can be done. This delays the early identification of preterm infants at risk for altered neurobehavioral outcomes and hinders the development of critical early interventions. The utilization of maternal breastmilk and other maternal/paternal involvement may buffer the negative influences of early-life pain/stress. Future studies are warranted to understand the benefits of such practices and identify/develop additional interventions to optimize neurobehavioral outcomes in preterm infants at risk.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Field, D. J., Dorling, J. S., Manktelow, B. N. & Draper, E. S. Survival of extremely premature babies in a geographically defined population: prospective cohort study of 1994-9 compared with 2000-5. BMJ 336, 1221–1223 (2008).
Itabashi, K. et al. Mortality rates for extremely low birth weight infants born in Japan in 2005. Pediatrics 123, 445–450 (2009).
Patel, R. M. et al. Causes and timing of death in extremely premature infants from 2000 through 2011. N. Engl. J. Med. 372, 331–340 (2015).
Norman, M. et al. Association between year of birth and 1-year survival among extremely preterm infants in Sweden during 2004-2007 and 2014-2016. JAMA 321, 1188–1199 (2019).
Mooney-Leber, S. M. & Brummelte, S. Neonatal pain and reduced maternal care: early-life stressors interacting to impact brain and behavioral development. Neuroscience 342, 21–36 (2017).
Cong, X. et al. The impact of cumulative pain/stress on neurobehavioral development of preterm infants in the NICU. Early Hum. Dev. 108, 9–16 (2017).
Chau, C. M., Cepeda, I. L., Devlin, A. M., Weinberg, J. & Grunau, R. E. The Val66Met brain-derived neurotrophic factor gene variant interacts with early pain exposure to predict cortisol dysregulation in 7-year-old children born very preterm: Implications for cognition. Neuroscience 342, 188–199 (2017).
Badr, L. K., Abdallah, B. & Kahale, L. A meta-analysis of preterm infant massage: an ancient practice with contemporary applications. MCN Am. J. Matern. Child Nurs. 40, 344–358 (2015).
Ganguly, A., Bhadesia, P. J., Phatak, A. G., Nimbalkar, A. S. & Nimbalkar, S. M. Pain profile of premature infants during routine procedures in neonatal intensive care: an observational study. J. Fam. Med. Prim. Care. 9, 1517–1521 (2020).
Mooney-Leber, S. M. & Brummelte, S. Neonatal pain and reduced maternal care alter adult behavior and hypothalamic-pituitary-adrenal axis reactivity in a sex-specific manner. Dev. Psychobiol. 62, 631–643 (2020).
Zimmerman, K. O. et al. Sedation, analgesia, and paralysis during mechanical ventilation of premature infants. J. Pediatr. 180, 99.e1–104.e1 (2017).
McPherson, C., Miller, S. P., El-Dib, M., Massaro, A. N. & Inder, T. E. The influence of pain, agitation, and their management on the immature brain. Pediatr. Res. 88, 168–175 (2020).
Barrero-Castillero, A., Morton, S. U., Nelson, C. A. 3rd & Smith, V. C. Psychosocial stress and adversity: effects from the perinatal period to adulthood. Neoreviews 20, e686–e696 (2019).
Brummelte, S. et al. Procedural pain and brain development in premature newborns. Ann. Neurol. 71, 385–396 (2012).
Vinall, J. et al. Neonatal pain in relation to postnatal growth in infants born very preterm. Pain 153, 1374–1381 (2012).
Smith, G. C. et al. Neonatal intensive care unit stress is associated with brain development in preterm infants. Ann. Neurol. 70, 541–549 (2011).
Slater, R. et al. Premature infants display increased noxious-evoked neuronal activity in the brain compared to healthy age-matched term-born infants. Neuroimage 52, 583–589 (2010).
Kostovic, I. & Rakic, P. Developmental history of the transient subplate zone in the visual and somatosensory cortex of the macaque monkey and human brain. J. Comp. Neurol. 297, 441–470 (1990).
Perry, M. et al. Neonatal pain: perceptions and current practice. Crit. Care Nurs. Clin. North Am. 30, 549–561 (2018).
Committee on Fetus and Newborn and Section on Anesthesiology and Pain Medicine. Prevention and management of procedural pain in the neonate: an update. Pediatrics 137, e20154271 (2016).
Campbell-Yeo, M. et al. Sustained efficacy of kangaroo care for repeated painful procedures over neonatal intensive care unit hospitalization: a single-blind randomized controlled trial. Pain 160, 2580–2588 (2019).
Banga, S., Datta, V., Rehan, H. S. & Bhakhri, B. K. Effect of sucrose analgesia, for repeated painful procedures, on short-term neurobehavioral outcome of preterm neonates: a randomized controlled trial. J. Trop. Pediatr. 62, 101–106 (2016).
Meesters, N. J. et al. Acute pain assessment in prematurely born infants below 29 weeks: a long way to go. Clin. J. Pain 35, 975–982 (2019).
Wang, Y., Zhao, T., Zhang, Y., Li, S. & Cong, X. Positive effects of kangaroo mother care on long-term breastfeeding rates, growth, and neurodevelopment in preterm infants. Breastfeed. Med. 16, 282–291 (2021).
El-Farrash, R. A. et al. Longer duration of kangaroo care improves neurobehavioral performance and feeding in preterm infants: a randomized controlled trial. Pediatr. Res. 87, 683–688 (2020).
Cheong, J., Burnett, A. C., Treyvaud, K. & Spittle, A. J. Early environment and long-term outcomes of preterm infants. J. Neural Transm. 127, 1–8 (2020).
Bergman, N. J. Birth practices: maternal-neonate separation as a source of toxic stress. Birth Defects Res. 111, 1087–1109 (2019).
Zwicker, J. G. et al. Score for neonatal acute physiology-II and neonatal pain predict corticospinal tract development in premature newborns. Pediatr. Neurol. 48, 123.e1–129.e1 (2013).
Ranger, M. et al. Neonatal pain-related stress predicts cortical thickness at age 7 years in children born very preterm. PLoS ONE 8, e76702 (2013).
Ranger, M. et al. Neonatal pain and infection relate to smaller cerebellum in very preterm children at school age. J. Pediatr. 167, 292–298.e291 (2015).
Grunau, R. E. et al. Neonatal pain, parenting stress and interaction, in relation to cognitive and motor development at 8 and 18 months in preterm infants. Pain 143, 138–146 (2009).
Moore, G. A., Cohn, J. F. & Campbell, S. B. Infant affective responses to mother’s still face at 6 months differentially predict externalizing and internalizing behaviors at 18 months. Dev. Psychol. 37, 706–714 (2001).
Ranger, M., Synnes, A. R., Vinall, J. & Grunau, R. E. Internalizing behaviours in school-age children born very preterm are predicted by neonatal pain and morphine exposure. Eur. J. Pain 18, 844–852 (2014).
Newnham, C. A., Inder, T. E. & Milgrom, J. Measuring preterm cumulative stressors within the NICU: the Neonatal Infant Stressor Scale. Early Hum. Dev. 85, 549–555 (2009).
Gao, H. et al. Efficacy and safety of repeated oral sucrose for repeated procedural pain in neonates: a systematic review. Int. J. Nurs. Stud. 62, 118–125 (2016).
Stokowski, L. A. Quantifying neonatal stress in the NICU. Adv. Neonatal Care 9, 205 (2009).
Lester, B. M., Andreozzi-Fontaine, L., Tronick, E. & Bigsby, R. Assessment and evaluation of the high risk neonate: the NICU Network Neurobehavioral Scale. J. Vis. Exp. 3368 (2014).
Lester, B. M., Tronick, E. Z. & Brazelton, T. B. The Neonatal Intensive Care Unit Network Neurobehavioral Scale procedures. Pediatrics 113, 641–667 (2004).
Harris, P. A. et al. The REDCap consortium: building an international community of software platform partners. J. Biomed. Inform. 95, 103208 (2019).
R Core Team. R: A Language and Environment for Statistical Computing (Computer Program) (R Foundation for Statistical Computing, 2017).
Brockhaus, S., Rügamer, D. & Greven, S. Boosting functional regression models with FDboost. J. Stat. Softw. 94, 1–50 (2020).
Hothorn, T., Hornik, K. & Zeileis, A. Unbiased recursive partitioning: a conditional inference framework. J. Comput. Graph. Stat. 15, 651–674 (2006).
Dutt, S., Sivaraman, A., Savoy, F. & Rajalakshmi, R. Insights into the growing popularity of artificial intelligence in ophthalmology. Indian J. Ophthalmol. 68, 1339–1346 (2020).
Allinson, L. G. et al. Physiological stress responses in infants at 29-32 weeks’ postmenstrual age during clustered nursing cares and standardised neurobehavioural assessments. BMJ Paediatr. Open 1, e000025 (2017).
Tronick, E. Z. et al. Normative neurobehavioral performance of healthy infants on the Neonatal Intensive Care Unit Network Neurobehavioral Scale. Pediatrics 113, 676–678 (2004).
D’Agata, A. L. et al. FKBP5 genotype and early life stress exposure predict neurobehavioral outcomes for preterm infants. Dev. Psychobiol. 59, 410–418 (2017).
Rantakari, K. et al. Early oxygen levels contribute to brain injury in extremely preterm infants. Pediatr Res. 90, 131–139 (2021).
Nist, M. D., Pickler, R. H., Steward, D. K., Harrison, T. M. & Shoben, A. B. Inflammatory mediators of stress exposure and neurodevelopment in very preterm infants: protocol for the stress neuro-immune study. J. Adv. Nurs. 75, 2236–2245 (2019).
DeMaster, D. et al. Nurturing the preterm infant brain: leveraging neuroplasticity to improve neurobehavioral outcomes. Pediatr. Res. 85, 166–175 (2019).
Rice, D. & Barone, S. Jr Critical periods of vulnerability for the developing nervous system: evidence from humans and animal models. Environ. Health Perspect. 108(Suppl. 3), 511–533 (2000).
Wallois, F., Routier, L. & Bourel-Ponchel, E. Impact of prematurity on neurodevelopment. Handb. Clin. Neurol. 173, 341–375 (2020).
Apkarian, A. V., Bushnell, M. C., Treede, R. D. & Zubieta, J. K. Human brain mechanisms of pain perception and regulation in health and disease. Eur. J. Pain 9, 463–484 (2005).
Holsti, L., MacLean, K., Oberlander, T., Synnes, A. & Brant, R. Calmer: a robot for managing acute pain effectively in preterm infants in the neonatal intensive care unit. Pain Rep. 4, e727 (2019).
Pierrat, V. et al. Neurodevelopmental outcome at 2 years for preterm children born at 22 to 34 weeks’ gestation in France in 2011: EPIPAGE-2 cohort study. BMJ 358, j3448 (2017).
Eeles, A. L. et al. Continuum of neurobehaviour and its associations with brain MRI in infants born preterm. BMJ Paediatr. Open. 1, e000136 (2017).
Brown Belfort, M. The science of breastfeeding and brain development. Breastfeed. Med. 12, 459–461 (2017).
Lechner, B. E. & Vohr, B. R. Neurodevelopmental outcomes of preterm infants fed human milk: a systematic review. Clin. Perinatol. 44, 69–83 (2017).
Pineda, R. et al. Maternal milk and relationships to early neurobehavioral outcome in preterm infants. J. Perinat. Neonatal Nurs. 34, 72–79 (2020).
O’Connor, D. L. et al. Effect of supplemental donor human milk compared with preterm formula on neurodevelopment of very low-birth-weight infants at 18 months: a randomized clinical trial. JAMA 316, 1897–1905 (2016).
Miller, J. et al. A systematic review and meta-analysis of human milk feeding and morbidity in very low birth weight infants. Nutrients 10, 707 (2018).
Quigley, M., Embleton, N. D. & McGuire, W. Formula versus donor breast milk for feeding preterm or low birth weight infants. Cochrane Database Syst. Rev. 6, CD002971 (2018).
Acknowledgements
The authors thank medical and nursing staff in the NICUs of Connecticut Children’s Medical Center at Hartford and Farmington, CT for their support and assistance. We thank Victoria Vazquez, Shari Galvin, Megan Fitzsimons, and Dorothy Vittner for their assistance in recruiting subjects and data collection.
Funding
This study was supported by the NIH/NINR (grant numbers: K23NR014674 and NR016928; PI: X.C.; F31NR019940, PI: T.Z.).
Author information
Authors and Affiliations
Contributions
All authors met the Pediatric Research authorship requirements. Substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data: all authors. Drafting and revising the manuscript: T.Z., T.G., Y.Z., H.L., and X.C. Thoroughly reviewed and critiqued the manuscript for revision: B.L. and N.H. Final approval of the version to be published: all authors.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
Patient consent was required for our paper. Eligible infants were identified by the research study personnel after birth and/or admission to the NICU and consent from parents of the eligible infant was required and obtained for participating in our study.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Zhao, T., Griffith, T., Zhang, Y. et al. Early-life factors associated with neurobehavioral outcomes in preterm infants during NICU hospitalization. Pediatr Res 92, 1695–1704 (2022). https://doi.org/10.1038/s41390-022-02021-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-022-02021-y
