
Abstract
Background
Large volumes of non-resuscitation fluids are often administered to critically ill children. We hypothesize that excess maintenance fluid is a significant contributor to non-resuscitation fluid and that non-resuscitation fluid administered beyond hydration requirements is associated with worse clinical outcomes in critically ill children.
Methods
We evaluated all patients admitted to two large urban pediatric intensive care units (PICU) between January 2010–August 2016 and January 2010–August 2018, respectively, who survived and remained in the hospital for at least 3 days following PICU admission. The primary outcome was in-hospital mortality. Association of excess fluid with outcomes was adjusted for confounders (age, Pediatric Risk of Mortality III score, study site, day 3 acute kidney injury, PICU era, resuscitation volume, and volume output) using multivariable regression.
Results
We evaluated 14,483 patients; 52% received non-resuscitation fluid in excess of hydration requirements. Non-resuscitation fluid in excess of hydration requirements was associated with higher in-hospital mortality after adjustment for confounders (adjusted odds ratio 1.01 per 10 mL/kg in excess fluid, 95% confidence interval: 1.002–1.02).
Conclusions
Non-resuscitation fluid in excess of hydration requirements is associated with increased mortality in critically ill children. Excess maintenance fluid is a modifiable contributor to this fluid volume. Strategies to reduce excess maintenance fluids warrant further study.
Impact
-
Critically ill children frequently receive non-resuscitation fluid in excess of their estimated hydration requirements.
-
Non-resuscitation fluid volume in excess of estimated hydration requirements is associated with higher morbidity and mortality in critically ill children.
-
Critically ill children receive a large volume burden from maintenance fluid.
-
Maintenance fluid represents a modifiable contributor of non-resuscitation fluid in excess of hydration requirements.
-
Strategies focused on limitation of maintenance fluid warrant further study.
Similar content being viewed by others

Introduction
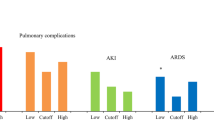
Fluid administration and management are cornerstones of critical care.1 Many critically ill patients receive large volumes of fluid both as part of their initial resuscitation and throughout the course of their critical illness, and this may lead to fluid overload (FO).2 FO is known to be associated with poor clinical outcomes, including higher mortality rates, increased duration of mechanical ventilation, longer lengths of stay, and higher incidence of acute kidney injury (AKI).3,4,5,6,7,8,9,10,11,12
Few studies have focused on the role that non-resuscitation fluids play in the development of FO. Van Regenmortel et al.2 demonstrated that, in an adult intensive care unit, almost 60% of the fluid administered to patients was in the form of maintenance fluids and “fluid creep,” defined as the combined volume used from medications, electrolytes, and continuous infusions used to keep access lines open. Furthermore, among patients with sepsis, the authors demonstrated that non-resuscitation fluids had a greater impact on cumulative fluid balance than resuscitation fluids. Similarly, Linden-Sonderso et al.13 demonstrated that non-resuscitation fluids represent a larger source of volume than resuscitation fluids. Studies in children have also demonstrated that a large fluid burden may result from non-resuscitation fluids, especially maintenance fluids.14,15 Recently, Al-Lawati et al.15 demonstrated that fluid exposure frequently exceeded hydration requirements on day 3 of pediatric intensive care unit (PICU) admission. However, the degree to which non-resuscitation fluid in excess of hydration requirements impacts clinical outcomes has not been previously studied.
In this large two-center observational cohort study, we aimed to describe the frequency at which non-resuscitation fluid exceeds hydration requirements and to describe the relative volume load from each contributing fluid source. We further aimed to evaluate the association of non-resuscitation fluid in excess of hydration requirements on in-hospital mortality and ventilator-free days in critically ill children.
Methods
Study design and population
This was a retrospective observational cohort study of all PICU patients admitted to the Ann & Robert H. Lurie Children’s Hospital between September 2010 and August 2018 and those admitted to the University of Chicago Comer Children’s Hospital between January 2010 and August 2016 who were in the hospital and alive on day 3 after PICU admission. We excluded patients recovering from cardiac surgery. In addition, we excluded patients who had no weight recorded and those who had no fluid inputs or outputs recorded. All data were extracted from the electronic health records (EHRs) of each institution using structured query language and underwent systematic quality checks to ensure conformance, completeness, and plausibility.16 The Institutional Review Boards at both centers approved the study with a waiver of informed consent.
Clinical variables
We collected the sources and volumes of fluid administered to patients, as recorded by the bedside clinicians in the EHR, from days 1 to 3 following PICU admission. Days following PICU admission were defined as the 24-h periods starting at the time of PICU admission (e.g., day 1 was from PICU admission to 24 h afterwards, not calendar days). We chose to study the first 3 days after PICU admission because the timing corresponds with the resuscitation and stabilization phase of care.17,18 Daily fluid balance was calculated as the total volume administered minus the daily fluid output (e.g., urine, drain output, etc.). FO percentage was calculated as the cumulative fluid balance in liters divided by the PICU admission weight in kilograms and multiplied by 100.5 Severity of illness on admission was based on the Pediatric Risk of Mortality III (PRISM III) score in the first 24 h.19 AKI was defined using the Kidney Disease Improving Global Outcomes serum creatinine criteria.20 Maximum creatinine was defined as the highest creatinine in the first 72 h after PICU admission. Baseline creatinine was defined as the lowest serum creatinine in the 3 months prior to admission. If no baseline creatinine was available, one was calculated based on previously validated estimations based on age and sex.21,22 PICU era was categorized into the first half of study years (January 2010–December 2013) and the second half of study years (January 2014–August 2018).
Outcomes
The primary outcome was in-hospital mortality and the secondary outcome was ventilator-free days at 28 days.
FO strata
To study the role of resuscitation and non-resuscitation fluids in the volume input of different FO strata, we stratified patients into one of three strata based on their degree of FO at the end of day 3 after PICU admission (<10, 10–20, and >20%), a method previously used in other studies.5,23,24,25 We compared the volume and sources of fluids administered across the FO strata.
Fluid sources and volumes
Fluid sources were grouped into six categories: (1) resuscitation, (2) maintenance fluids, (3) blood products, (4) enteral and parenteral nutrition, (5) renal replacement therapy, and (6) fluid creep.2 Fluid creep was defined as the combined volume used from medications, electrolytes, and continuous infusions used to keep access lines open, as previously described.2 Two authors (M.F.B., L.N.S.) verified the classification as recorded by nurses. If a single administration of crystalloid or colloid fluids was ≥10 mL/kg or was labeled as a “bolus” (e.g., “Normal Saline Bolus,” “Lactated Ringers Bolus,” etc.), it was classified as a resuscitation fluid. The other fluids were classified according to the clinical label recorded in the EHR (e.g., “Maintenance fluids,” “Blood product,” etc.). Of note, the term maintenance fluid here refers to the continuous intravenous fluid (with or without dextrose) administered to patients that was labeled as “maintenance” in the EHR by the bedside clinicians.
Non-resuscitation volume was defined as the total volume administered minus the resuscitation fluid volume. Hydration requirement volume was estimated based on the Holliday–Segar method (i.e., “4-2-1 rule”): 4 mL/kg/h for the first 10 kg, 2 mL/kg/h for the second 10 kg, and 1 mL/kg/h for each additional kg of weight.26 This estimation method was chosen for its conservative estimation of maintenance requirements in critically ill children and because it is commonly used in pediatrics: a recent survey showed that 96% of PICU providers used the 4-2-1 method for patients with acute respiratory distress syndrome.27 Non-resuscitation in excess of hydration requirements was defined as the total non-resuscitation volume minus the estimated hydration requirement volume for each patient.
To estimate the relative impact that maintenance fluids had on the non-resuscitation fluid in excess of hydration requirements, we calculated the potential decrease in % FO that would have occurred with a limitation of maintenance fluid to not exceed the estimated hydration requirements. For example, if a patient received non-resuscitation fluids in excess of hydration requirements and this volume included maintenance fluids, the potential decrease was equivalent to the amount of maintenance fluid given in excess of hydration needs. We further compared the median % FO for subjects before and after maintenance adjustment and performed a Wilcoxon rank-sum test for statistical significance.
Statistical analysis
To evaluate the association of FO strata with mortality, we performed a multivariable logistic regression analysis adjusting for confounders including age, PRISM III score, day 3 AKI, study site, and PICU era.
To evaluate the association of non-resuscitation fluid in excess of hydration requirements on in-hospital mortality, we performed a multivariable logistic regression analysis adjusting for confounders, including age, PRISM III score, day 3 AKI, study site, PICU era, resuscitation volume (in mL/kg during the first 3 days), and output volume (including urine and other outputs in mL/kg during the first 3 days). The resuscitation volume and output volume were included in these regression analyses in order to adjust for other fluid-relevant measures of severity of illness. To assess our secondary outcomes of ventilator-free days at 28 days, we performed a multivariable Poisson regression adjusting for the same confounders. The confounding variables were chosen a priori and are the same as above. Non-resuscitation fluid in excess of hydration requirements was used as a continuous variable. In addition, we performed two sensitivity analyses. First was in the subpopulation of patients requiring mechanical ventilation at some point during the first 3 days after PICU admission; and second, was in the subpopulation of patients who received maintenance fluid on each of the first 3 days of their PICU admission.
Data analysis was performed using STATA 14 (StataCorp LP, Texas) and R version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria). Clinical, demographic, and fluid data were summarized and compared between groups. Non-normally distributed continuous variables were compared using Wilcoxon rank-sum and Kruskal–Wallis tests and categorical variables were compared using the χ2 test. Statistical significance level was set at a two-sided α < 0.05.
Results
There were 14,825 patients who were alive and in the hospital on day 3 after PICU admission. Three hundred and forty-two did not have a weight on admission or fluids recorded and were excluded. The final analysis included 14,483 patients; of these, 45% (n = 6545) were female. The patients had a median age of 4.6 years (interquartile range [IQR] 1.2–11.9), a median weight of 16.8 kg (IQR 9.4–38), a day 3 AKI rate of 11% (n = 1587), a median length of stay of 6 days (IQR 3.8–11.5), and a mortality rate of 2.1% (n = 311). A large proportion of patients received maintenance fluid each day (day 1: 91%; day 2: 79%; and day 3: 61%). In addition, many patients received resuscitation fluid each day (day 1: 30.4%; day 2: 11.5%; and day 3: 8.9%).
Table 1 presents the clinical characteristics and outcomes of the study population stratified by % FO on day 3 after PICU admission. There were significant differences in age, sex, weight, PRISM III scores, day 3 AKI rates, hospital length of stay, ventilator-free days, and mortality based on FO strata.
Fluid Sources and Volumes in the FO Strata
Table 2 summarizes the relative volumes of different sources of fluid for each of the first 3 days following PICU admission using mean volumes (Supplementary Table 1 presents the same information using median volumes). Maintenance fluid and nutrition were the largest contributors to the fluid input. Maintenance fluid decreased daily in all FO strata but remained a large volume load (day 1: 63%, 52%, and 37% vs. day 3: 34%, 27%, and 23% across the <10%, 10–20%, and >20% strata, respectively). Nutrition increased in proportion daily in all FO strata (day 1: 22%, 31%, 30% vs. day 3: 59%, 66%, and 51% across the <10%, 10–20%, and >20% strata, respectively). The vast majority of nutrition was enteral for all strata (>89% enteral vs. <11% parenteral for all days). Notably, while the relative contribution was lower, the absolute volume from each source increased with increasing FO strata. Resuscitation fluid decreased over the first 3 days in all FO strata. Fluid creep had similar volumes for the 3 days across the fluid strata. Blood products and renal replacement fluids remained small contributors and had similar volumes across the fluid strata over the 3 days (Table 2).
Estimated hydration requirements were calculated using the Holliday–Segar “4-2-1” method.26 Patients received non-resuscitation volume in excess of this estimated hydration requirement 52% of the time: 45% of those in the <10% FO stratum, 77.5% of those in the 10–20% FO stratum, and 92.4% of those in the >20% FO stratum. Table 3 summarizes the volumes of non-resuscitation fluid in excess of hydration requirements by FO strata and the estimated potential decrease in % FO with excess maintenance fluid limitation (Supplementary Table 2 presents the same information using median volumes). This potential decrease in % FO with the limitation of excess maintenance fluid assumes a constant fluid output, which is a reasonable assumption based on the relatively stable output across strata as seen in Table 2. With excess maintenance fluid limitation, 43% patients in the 10–20% FO stratum and 51% of the >20% FO stratum would have been recategorized to a lower FO stratum. Figure 1 shows the number of patients who would have been recategorized to a lower % FO stratum after adjustment.

Percent fluid overload (% FO) was calculated as fluid balance in liter (L) divided by admission weight in kilograms (kg) × 100 for each day. The strata were divided into three cohorts <10, 10–20, and >20% FO based on the actual fluids balance on day 3 after PICU admission. We estimated the %FO decrease that would have occurred with a hypothetical limitation of only the maintenance fluid such that the patient’s continuous fluid would not exceed their estimated hydration requirements unless due to other forms of non-resuscitation fluids.
Our multivariable logistic regression analysis of FO strata and mortality found a dose-dependent effect: the 10–20% stratum had 1.8 times increased adjusted odds of death (95% confidence interval (CI): 1.3–2.4) and the >20% stratum had 2.6 times increased adjusted odds of death (95% CI: 1.7–3.8) when compared to the <10% stratum and after adjusting for confounders. Supplementary Table 3 reports the unadjusted and adjusted odds ratios for the regression models.
Excess non-resuscitation fluid and outcomes
In the unadjusted model of non-resuscitation fluid in excess of hydration requirements with mortality, every 10 mL/kg of excess non-resuscitation fluids in excess of hydration needs had 1.03 times higher odds of death (95% CI: 1.02–1.03). In the adjusted model, every 10 mL/kg excess non-resuscitation fluids had 1.01 times higher odds of death (95% CI: 1.002–1.02). This implies that every 10 mL/kg of non-resuscitation fluids in excess of hydration requirement given over the first 3 days after PICU admission to critically ill children is independently associated with a 1% increase in the odds of in-hospital mortality. Supplementary Table 4 reports the unadjusted and adjusted odds ratios for the regression model.
In the unadjusted Poisson model of non-resuscitation fluid in excess of hydration requirements with the likelihood to have a ventilator-free day, there was a 1% decrease in the likelihood of having a ventilator-free day for every 10 mL/kg (incidence rate ratio [IRR] 0.99, 95% CI: 0.99–0.99) and in the adjusted model there was a 1% decrease in the likelihood of having a ventilator-free day for every 10 mL/kg (IRR 0.99, 95% CI: 0.99–0.99).
We further performed two sensitivity analyses. The first was in the subgroup of patients who required mechanical ventilation at some point during the first 3 days after PICU admission (n = 6210) and had similar results as the full population. The second was in the subgroup of patients who received maintenance fluids on each of the first 3 days following PICU admission (n = 8558) and had similar results as the full population.
Discussion
Prior studies have demonstrated an association between conservative fluid management and improved clinical outcomes.28,29,30,31,32 However, the relative impact of conservative use of resuscitation fluids vs. a conservative use of non-resuscitation fluids is unclear. In our two-center observational study, we demonstrated that a majority of critically ill children receive non-resuscitation fluid in excess of their estimated hydration requirements. We also demonstrated that non-resuscitation fluid in excess of hydration requirements is associated with higher mortality and fewer ventilator-free days after adjusting for confounders including the severity of illness, age, resuscitation fluid volume, and fluid output volume. While the adjusted increase of 1% in the odds of death and the 1% decrease in the adjusted incidence rate of having a ventilator-free day for each 10 mL/kg of excess fluids appears like a small effect, this must be considered in context. First, some patients receive a large volume of excess fluid: the average patient in the >20% FO strata had a mean of 164.3 mL/kg of non-resuscitation fluid in excess of hydration requirements, which equates to a 16% increase in the adjusted odds of death and a 16% decrease in the adjusted incidence rate of having a ventilator-free day for the average patient in that stratum. Second, non-resuscitation fluid in excess of hydration needs is potentially a modifiable risk factor.
Identification of volume and sources of fluid may be important to reduce the non-essential fluid burden. Since non-resuscitation fluid encompasses multiple fluid sources: blood products, fluid creep, maintenance fluid, and so on, we evaluated these sources across FO strata to compare the volumes from each source. Notably, the volume from each source was higher with increasing FO strata, including maintenance. Thus, the most fluid overloaded patients received the most maintenance fluid. In fact, our data showed that about half of the patients in both the 10–20 and >20% FO strata would have been reclassified into a lower % FO stratum with the elimination of the excess maintenance fluid.
Previous literature has shown that maintenance fluid represents a significant volume burden. Van Regenmortel et al.2 found that maintenance fluid accounted for 25% of mean daily total fluid volume while resuscitation accounted for <7% in the first week of admission in critically ill adults. Maes et al.33 demonstrated that maintenance fluids accounted for 49% and 71% of total fluid received on days 1 and 2, respectively, among adults following coronary artery bypass surgery. Pediatric studies, although smaller in size, have demonstrated a similar trend in the volume burden associated with maintenance fluids.14,15 Maintenance fluids are primarily used to prevent dehydration and to provide a source of glucose to prevent starvation ketosis. However, our data demonstrate that maintenance fluids are frequently given to patients with fluid in excess of hydration requirements and this practice may represent iatrogenic harm. If glucose or caloric needs are met with the administration of other fluids (e.g., enteral nutrition, dextrose-containing medication solutions, etc.), limitation of maintenance fluid beyond hydration needs could represent a relatively simple way of reducing potential FO and its sequelae. It is possible that certain patients benefited from the additional volume, but based on our outcome analyses we conclude that, on balance, most patients who receive non-resuscitation fluid in excess of hydration requirements are being harmed by it.
Critically ill children have complex physiology with variable urine output, insensible losses, and losses from drainage devices, and there is a need for frequent readjustment of the continuous intravenous fluids given to balance their needs. Our current use of maintenance fluids suggests that we are not considering all forms of continuous intravenous fluids when evaluating the patients’ actual maintenance needs. Future studies should investigate if limiting continuous intravenous fluids and specifically maintenance fluids, possibly through a total continuous fluid order, would lead to improved clinical outcomes.
Our study has several strengths and limitations. Our cohort is a large heterogeneous population of patients collected from two different institutions, which increases the generalizability of our findings. There are, however, several important limitations that warrant discussion. First, our data are retrospective and observational, and we are only able to establish associations and not causality. Second, although our study size is large, the results could be subject to a selection bias due to the types of critically ill children admitted to urban pediatric hospitals. Third, the % FO assessment we used is based on admission weight, and in patients who are admitted with significant dehydration, we may be overestimating their degree of FO. Fourth, the FO assessment is based on fluid balance and does not account for insensible fluid loss. Fifth, it is possible that some of the sicker patients were given a purposefully increased volume of continuous intravenous fluids as part of their resuscitation effort and this would not be reflected as resuscitation fluid but as non-resuscitation fluids. Sixth, we included intravenous and enteral fluid volumes as equivalent. It is possible that enteral volume does not have the same physiologic effect as intravenous volumes in critically ill children, particularly in children who have decreased enteral absorption. Seventh, our estimated hydration requirements were based on the Holliday–Segar “4-2-1” method. This method was derived in healthy children and may not be an accurate reflection of the daily hydration requirements of critically ill children. It was chosen because of its frequent use in pediatrics and its conservative estimation of hydration requirements.27 The authors are not endorsing its use in critically ill children. Eighth, our estimated % FO changes with limitation of maintenance fluids may not be accurate due to potential changes in urine output with reduction in fluid input. However, the cumulative total fluid output among the three FO strata were clinically similar, suggesting that on average fluid output tends to remain relatively stable in critically ill children regardless of volume input. Finally, we only included common, observed confounders in our adjusted analyses. Unobserved confounders, such as the degree of capillary leak, renal tubular dysfunction, or myocardial dysfunction, may affect the relationship between fluids and outcomes; however, these cannot be easily measured or adjusted for using retrospective observational data.
Conclusions
Non-resuscitation fluid in excess of hydration requirements is associated with increased morbidity and mortality in critically ill children. Maintenance fluid is a significant contributor to this excess volume. The current practice of maintenance fluids administration may represent an easily modifiable iatrogenic harm. Fluid-restrictive strategies focusing on the reduction of excess maintenance fluids warrant further study.
References
Rhodes, A. et al. Surviving sepsis campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intens. Care Med. 43, 304–377 (2017).
Van Regenmortel, N., Verbrugghe, W., Roelant, E., Van den Wyngaert, T. & Jorens, P. G. Maintenance fluid therapy and fluid creep impose more significant fluid, sodium, and chloride burdens than resuscitation fluids in critically ill patients: a retrospective study in a tertiary mixed ICU population. Intens. Care Med. 44, 409–417 (2018).
Alobaidi, R. et al. Association between fluid balance and outcomes in critically ill children: a systematic review and meta-analysis. JAMA Pediatr. 172, 257–268 (2018).
Malbrain, M. L. et al. Fluid overload, de-resuscitation, and outcomes in critically ill or injured patients: a systematic review with suggestions for clinical practice. Anaesthesiol. Intens. Ther. 46, 361–380 (2014).
Sutherland, S. M. et al. Fluid overload and mortality in children receiving continuous renal replacement therapy: the prospective pediatric continuous renal replacement therapy registry. Am. J. Kidney Dis. 55, 316–325 (2010).
Arikan, A. A. et al. Fluid overload is associated with impaired oxygenation and morbidity in critically ill children. Pediatr. Crit. Care Med. 13, 253–258 (2012).
Valentine, S. L. et al. Pediatric Acute Lung I, Sepsis Investigator’s N, Acute Respiratory Distress Syndrome Clinical Research N. Fluid balance in critically ill children with acute lung injury. Crit. Care Med. 40, 2883–2889 (2012).
Goldstein, S. L. et al. Outcome in children receiving continuous venovenous hemofiltration. Pediatrics 107, 1309–1312 (2001).
Goldstein, S. L. et al. Pediatric patients with multi-organ dysfunction syndrome receiving continuous renal replacement therapy. Kidney Int. 67, 653–658 (2005).
Flori, H. R., Church, G., Liu, K. D., Gildengorin, G. & Matthay, M. A. Positive fluid balance is associated with higher mortality and prolonged mechanical ventilation in pediatric patients with acute lung injury. Crit. Care Res. Pract. 2011, 854142 (2011).
Gillespie, R. S., Seidel, K. & Symons, J. M. Effect of fluid overload and dose of replacement fluid on survival in hemofiltration. Pediatr. Nephrol. 19, 1394–1399 (2004).
Abulebda, K. et al. Post-ICU admission fluid balance and pediatric septic shock outcomes: a risk-stratified analysis. Crit. Care Med. 42, 397–403 (2014).
Linden-Sonderso, A. et al. Survey of non-resuscitation fluids administered during septic shock: a multicenter prospective observational study. Ann. Intens. Care 9, 132 (2019).
Bulfon, A. F. et al. Intravenous fluid prescription practices in critically ill children: a shift in focus from natremia to chloremia? J. Pediatr. Intens. Care 8, 218–225 (2019).
Al-Lawati, Z. H., Sur, M., Kennedy, C. E. & Akcan Arikan, A. Profile of fluid exposure and recognition of fluid overload in critically ill children. Pediatr. Crit. Care Med. 21, 760–766 (2020).
Kahn, M. G. et al. A harmonized data quality assessment terminology and framework for the secondary use of electronic health record data. EGEMS 4, 1244 (2016).
Malbrain, M. et al. Principles of fluid management and stewardship in septic shock: it is time to consider the four D’s and the four phases of fluid therapy. Ann. Intens. Care 8, 66 (2018).
Vincent, J. L. Fluid management in the critically ill. Kidney Int. 96, 52–57 (2019).
Pollack, M. M., Patel, K. M. & Ruttimann, U. E. PRISM III: an updated Pediatric Risk of Mortality score. Crit. Care Med. 24, 743–752 (1996).
Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin. Pract. 120, c179–c184 (2012).
Hessey, E. et al. Evaluation of height-dependent and height-independent methods of estimating baseline serum creatinine in critically ill children. Pediatr. Nephrol. 32, 1953–1962 (2017).
Hoste, L. et al. A new equation to estimate the glomerular filtration rate in children, adolescents and young adults. Nephrol. Dial. Transplant. 29, 1082–1091 (2014).
Modem, V., Thompson, M., Gollhofer, D., Dhar, A. V. & Quigley, R. Timing of continuous renal replacement therapy and mortality in critically ill children*. Crit. Care Med. 42, 943–953 (2014).
Diaz, F., Benfield, M., Brown, L. & Hayes, L. Fluid overload and outcomes in critically ill children: a single center prospective cohort study. J. Crit. Care 39, 209–213 (2017).
Muttath, A. et al. Adverse outcomes due to aggressive fluid resuscitation in children: a prospective observational study. J. Pediatr. Intens. Care 8, 64–70 (2019).
Holliday, M. A. & Segar, W. E. The maintenance need for water in parenteral fluid therapy. Pediatrics 19, 823–832 (1957).
Hassinger, A. B. & Valentine, S. L. Self-reported management of IV fluids and fluid accumulation in children with acute respiratory failure. Pediatr. Crit. Care Med. 19, e551–e554 (2018).
Silversides, J. A., Perner, A. & Malbrain, M. Liberal versus restrictive fluid therapy in critically ill patients. Intens. Care Med. 45, 1440–1442 (2019).
Evans, R. G. & Naidu, B. Does a conservative fluid management strategy in the perioperative management of lung resection patients reduce the risk of acute lung injury? Interact. Cardiovasc. Thorac. Surg. 15, 498–504 (2012).
Famous, K. R. et al. Acute respiratory distress syndrome subphenotypes respond differently to randomized fluid management strategy. Am. J. Respir. Crit. Care Med. 195, 331–338 (2017).
Wiedemann, H. P. et al. Comparison of two fluid-management strategies in acute lung injury. N. Engl. J. Med. 354, 2564–2575 (2006).
Maitland, K. et al. Mortality after fluid bolus in African children with severe infection. N. Engl. J. Med. 364, 2483–2495 (2011).
Maes, T. et al. Impact of maintenance, resuscitation and unintended fluid therapy on global fluid load after elective coronary artery bypass surgery. J. Crit. Care 49, 129–135 (2019).
Author information
Authors and Affiliations
Contributions
M.F.B.: study design, analysis, and first draft of the manuscript. D.N., G.C., and R.K.B.: study design and review of the manuscript. L.N.S.-P.: study design, analysis, and review of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Barhight, M.F., Nelson, D., Chong, G. et al. Non-resuscitation fluid in excess of hydration requirements is associated with higher mortality in critically ill children. Pediatr Res 91, 235–240 (2022). https://doi.org/10.1038/s41390-021-01456-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-021-01456-z
This article is cited by
-
Fluid assessment, fluid balance, and fluid overload in sick children: a report from the Pediatric Acute Disease Quality Initiative (ADQI) conference
Pediatric Nephrology (2024)
-
Fluid balance in critically ill children with lower respiratory tract viral infection: a cohort study
Journal of Anesthesia, Analgesia and Critical Care (2023)
-
A quality initiative to improve recognition of fluid overload among pediatric ICU patients requiring continuous kidney replacement therapy: preliminary results
Pediatric Nephrology (2023)
-
An update on the role of fluid overload in the prediction of outcome in acute kidney injury
Pediatric Nephrology (2023)
-
Medication and Fluid Management of Pediatric Sepsis and Septic Shock
Pediatric Drugs (2022)
