
Abstract
Numerous studies have examined the potential use of therapeutic gases for the treatment of various neurological disorders. Hydrogen gas, a promising neuroprotective agent, has been a focus of study due to its potent antioxidative properties. In translational research into adult diseases, hydrogen has been shown to be neuroprotective in disorders such as cerebral ischemia and traumatic brain injury, and in neurodegenerative diseases such as Alzheimer’s disease. Animal and human studies have verified the safety and feasibility of molecular hydrogen. However, despite extensive research on its efficacy in adults, only a few studies have investigated its application in pediatric and neonatal medicine. Neonatal hypoxic–ischemic encephalopathy (HIE) is characterized by damage to neurons and other cells of the nervous system. One of the major contributing factors is excessive exposure to oxidative stress. Current research interest in HIE is shifting toward new neuroprotective agents, as single agents or as adjuncts to therapeutic hypothermia. Here, we review therapeutic gases, particularly hydrogen, and their potentials and limitations in the treatment of HIE in newborns.
Impact
-
Translational animal models of neonatal HIE are a current focus of research into the therapeutic usefulness of various gases.
-
Hydrogen ventilation as a single agent or in combination with therapeutic hypothermia shows short- and long-term neuroprotection in neonatal translational HIE models.
-
The optimal target severity for therapeutic interventions should be well established to improve outcomes.
Similar content being viewed by others


Hydrogen and therapeutic gases for neonatal hypoxic–ischemic encephalopathy: potential neuroprotective adjuncts in translational research
In vivo, gaseous molecules such as oxygen (O2), carbon dioxide (CO2), carbon monoxide (CO), and hydrogen sulfide (H2S) play important roles under both physiological and pathological conditions in the regulation of organ functions such as cerebrovascular resistance and energy metabolism.1 With increased understanding of the interactions of gaseous molecules in biological systems, therapeutic gases have gained attention in recent years as potential neuroprotective agents in basic, translational, and clinical research of neonatal hypoxic–ischemic encephalopathy (HIE).
Hydrogen gas (H2) became a major focus of research in neonatal medicine after the discovery of its potent antioxidative properties in vivo and in vitro for adult diseases such as cerebral ischemia.2 Other major gases of interest for neonatal HIE are argon (Ar) and xenon (Xe). In neonatal HIE, gas therapy is administered either as a single agent or as an adjunct to the current standard treatment of therapeutic hypothermia (TH).
In this literature review, we briefly discuss the pathogenesis and current clinical situation of term neonatal HIE and then review hydrogen medicine and gas therapy in neonatal animal models of HIE, as well as those of other gaseous agents. In this article, we emphasize the mechanisms of action, treatment methods, ways to evaluate effectiveness, and future direction of hydrogen gas therapy in neonatal HIE.
Neonatal HIE
Neonatal HIE is one of the major causes of neonatal death, responsible for about one in five of all neonatal deaths worldwide. In addition, neonatal HIE leads to various degrees of neurological impairments. One severe consequence of HIE is cerebral palsy with or without mental retardation.3
The pathophysiology of HIE is highly complex. After hypoxia–ischemia (HI), cells undergo both injurious and recovery phases with ongoing feedback loops. HI leads to reduced ATP production at the cellular level. Under anaerobic energy conditions, cells accumulate glutamate, the excitatory amino acid. Glutamate allows increased Ca2+ influx into the cells, which activates lipase synthase and NO synthase, damaging the mitochondria and triggering the release of free radicals. The free radicals, in turn, lead to cell death, due not only to direct HI insult, but also to ischemic reperfusion (reoxygenation), which promotes the necrosis–apoptosis continuum.3,4,5 Necrotic cell death in turn induces inflammation, which allows further release of free radicals. Furthermore, neonatal brains have a deficient antioxidative system that makes them vulnerable to HI injury.6,7 Therefore, prevention of free radical injury is vital in neonatal HIE.
In general, free radicals in mammals are reactive oxygen and nitrogen species. Some important radicals are •OH (hydroxyl radicals), O2− (superoxide), H2O2 (hydrogen peroxide), and ONOO− (peroxynitrite). Most free radicals are signaling molecules: O2− is a precursor to H2O2, H2O2 itself acts as a secondary messenger, and •OH is also thought to act as a signaling molecule through lipid peroxidation. By-products of lipid peroxidation are involved in signaling through receptors.8,9 Of the radicals, hydroxyl radical (•OH) is the most potent, reacting indiscriminately with membrane lipids and proteins.2 H2 has no known target molecules, but •OH scavenging may be one of the main ways to reduce further oxidative injury.
Therapeutic hypothermia
The current standard treatment for neonatal HIE is TH (mild cooling of 33.0–34.0 °C for 72 h) initiated within 6 h after birth. The potential benefits of TH have been studied since ancient times.10 Before TH became the standard treatment for neonatal HIE, therapeutic interventions focused on the prevention and control of cerebral edema.11 However, none of the pharmacologic interventions have been proven to be useful and the research focus eventually shifted to agents, such as free radical scavengers, calcium channel blockers, and excitatory amino acid antagonists.12 One of the potential strategies is induced hypothermia.
The exact mechanisms underlying the neuroprotection afforded by TH in neonatal HIE are uncertain, but clearly multifactorial. After HI insult, cerebral blood flow decreases and the cells undergo anaerobic metabolism with the accumulation of lactate, which is responsible for mitochondrial dysfunction and cell death. TH reduces the lactate level in traumatic brain injury in rodents.13 In addition, 12–24 h of TH after HI insult seems to improve the status of secondary energy failure parameters in the mammalian brain.14 TH reduces the cerebral blood flow, with every degree Celsius fall in temperature reducing cerebral metabolism by 5–6%.15
In terms of oxidative stress and inflammation, TH prevents excessive release of the excitotoxic neurotransmitter glutamate by reducing glycine, which is responsible for the activation of N-methyl-d-aspartate (NMDA) receptor.16 TH significantly reduces the levels of free radicals and inflammatory cytokines.13,17
TH effectively ameliorates apoptosis, with both piglet and rat models showing fewer apoptotic cells.18,19 As an underlying mechanism, TH is partially involved in the intrinsic pathway for apoptosis through the suppression of cytochrome c release and activation of caspase-3 in neonatal rat brain. The important steps in the apoptotic pathways are activated by Fe2+ and ascorbic acid, which are both inhibited by TH.20 In traumatic brain injury animal models, TH alleviates the blood–brain barrier disruption, thereby relieving edema formation.21
Outcomes and limitations of TH
According to meta-analyses,22,23,24 TH reduces death or severe disabilities in term and late preterm infants with moderate-to-severe HIE. TH boosts the chance of survival with normal neurological function, reduces the rates of severe disability, significantly lowers electrographic seizure burden on early and prolonged continuous multichannel video electroencephalogram (EEG), and decreases the rates of cerebral palsy and a lower psychomotor index at 18 months of age. TH improves neurocognitive outcomes in middle childhood. Although not significant, academic achievements tend to be superior in TH-treated individuals and the use of special educational resources is also lower. A favorable outcome at 18 months of age is strongly associated with normal functional outcomes at school age.25,26
Despite the benefits of TH, nearly half of the infants who receive the treatment still die or are left with disabilities. To prevent one case of death or disability from HIE, seven or eight infants must be treated with TH. Thus, more work is needed to study outcomes.23
At any rate, new agents that can augment the effects of TH are required to further improve outcomes.
Hydrogen therapy: introduction
In mammals, H2 is produced by intestinal bacteria.27 H2 gas has been used in hydreliox (49% H2, 50% helium, 1% O2) to prevent decompression sickness and nitrogen narcosis in deep-sea divers for nearly three decades.28
H2 entered the spotlight as a potential therapeutic gas owing to the work of Ohsawa et al.2 from Japan in 2007. Its antioxidant, anti-inflammatory, and anti-apoptotic potential was shown both in vivo and in vitro. H2 selectively reduces •OH in cultured cells and •OH and ONOO− in cell-free systems. In the same report, H2 protected neurons and prevented further damage in a cerebral ischemic reperfusion model of adult rats. H2 inhalation also reduces edema and improves neurobehavioral functions.
The immunohistochemical results showed that H2 substantially protects cells from nuclear acid oxidation, lipid peroxidation, and microglia accumulation. In particular, microglia are involved in neuroinflammation and remodeling.2
Due to its remarkable therapeutic potential, over 300 reports have been published regarding H2 therapy in healthy normal individuals and those with various conditions, as well as in plants and animals. H2 is neuroprotective, cardioprotective, and effective in various diseases, such as sepsis, diabetes mellitus, malignancies, Alzheimer’s disease, and allergies. In the adult medical field, 19 clinical trials of H2 therapy have been published, and another 19 were registered between 2008 and 2015.29,30 However, there have been no trials in neonatal medicine.
H2 has many advantages. First and foremost, it is generally considered safe. In adult patients with post-cardiac arrest syndrome, a mixture of 4% H2 and 96% O2 inhalation was safe, but did not affect outcomes.31 The small molecular size of H2 allows it to cross biological membranes such as the blood–brain barrier. It is also effective at low concentrations (1–4%). As long as the concentration is below 4%, ignition is almost impossible. H2 is cheaper than other medical gases,2,29,30 and is thus cost-effective in clinical situations. Unlike Xe and Ar, H2 is not only neuroprotective, but also exerts protective effects in other organ systems.
In animal models, H2 can be delivered by oral ingestion, intravenous administration, inhalation/ventilation, and peritoneal injection. Inhalation/ventilation has many advantages. For example, it is the most straightforward method. In addition, for delivery to the brain, an advantage is its close proximity to the target organ. Inhalation allows H2 to reach a plateau within 10–20 min.32 In clinical practice, HIE neonates treated with TH require sedation and most babies receiving TH are managed with mechanical ventilation. In this article, inhalation and ventilation are considered to be the same.
Hydrogen ventilation in neonatal HIE animals
Neonatal rodent (e.g., rats and mice) and piglet HIE models are the most common translational models for studying the efficacy of H2 gas therapy. In rodent models, the HI insult is usually transient systemic hypoxia and permanent unilateral carotid artery ligation (Rice–Vannucci model).33 Rodent models offer better insight into molecular details, such as the effects of oxidative stress on the endoplasmic reticulum (ER), and enable assessment of neurobehavioral outcomes in relatively long-term periods, as well as showing a similar central nervous system maturation to human newborns (term human neonates are equivalent to days 10–14 in rodents).34,35 In rodents, even though the hypoxic component is systemic, the ischemic component can be unilateral, resulting, for example, in focal stroke-like lesions that do not resemble the selective neuronal necrosis pattern of brain injury in human term HIE neonates.36
Using a neonatal rat model, Cai et al.37 determined that inhalation of 2% H2 in postnatal day 7 (P7) rats effectively decreased the infarct ratio and reduced the neuronal loss in the cortex and hippocampus in a time-dependent manner. Even with initiation of H2 inhalation 30 min after ischemia–reperfusion, H2 effectively reduced the apoptosis in these brain areas and decreased caspase activity, which is an important regulator of apoptosis. In the same report, the level of caspase-12, which is specifically activated by ER stress, was also reduced. The H2 mechanism could involve the capture of free radicals, inhibiting caspases and preventing apoptotic cell death and thereby leading to morphological preservation of the brain.
However, H2 inhalation can be ineffective for moderate-to-severe HI insult. A study by Matchett et al.38 revealed that 2.9% H2 ventilation did not improve outcomes in P10 rats with severe insult. The authors stated that neuroprotection depended not only on the severity, but also on the age of the rats, with P10 rats not showing neuroprotection, unlike P7 rats. In the same report, a tendency for neuroprotection was seen in an adult rat stroke model.
Piglet models are also commonly used to study neonatal HIE. Piglets share a similar brain growth spurt near the time of birth to as human neonates.39 Piglet models have well-established data on cerebral metabolic processes.40,41,42,43,44,45,46 The neonatal HIE piglet model is also histologically similar to human HIE term neonates because the primary sensory and forebrain motor systems are preferentially damaged in neonatal HIE piglets.47 The effectiveness of TH and the new gaseous adjuncts Xe, Ar, and H2 have been studied using piglets.48,49,50,51,52,53,54,55,56,57,58,59,60
The early neuroprotective properties of H2 inhalation in a translational HIE piglet model were first reported by Nemeth et al.57 After hypoxia and reventilation, 2.1% H2 was delivered to the sedated piglets for 4 h. The piglets that received H2 therapy exhibited restored EEG function and had no electrographic seizures. Neuropathological outcomes were also improved. Immunohistochemistry of the parietal cortex 24 h after insult revealed a significant reduction in 8-hydroxy-2′-deoxyguanosine (8-OHdG), which is a biomarker of oxidative stress-induced DNA damage. The same group reported improved cerebrovascular reactivity and alleviated delayed neurovascular dysfunction with 2.1% H2 inhalation.55,58 In addition, based on a piglet model study by Varga et al.56 at 24 h after insult, H2 ventilation suppressed cyclooxygenase 2, an enzyme abundant in the cortex and hippocampus of the newborn brain that is upregulated in cerebral ischemia.
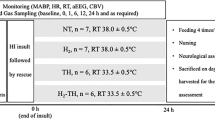
The neuroprotective effects of H2 ventilation were observed as single therapy. As an adjunct to TH, we reported its neuroprotective potential through assessment of the short-term neurological outcomes of combined therapy and histological findings in 5-day neonatal HIE piglets.59 H2 ventilation (2.1–2.7%, adjusted according to oxygen requirements) was administered for 24 h along with TH (33.0–34.0 °C). On day 3 after the insult, 83% of the piglets in the combined therapy group regained walking function. The highest neurological score was observed in the same group from days 2 to 5. Histological analysis revealed improved outcomes, particularly in the cortex. Apoptotic cells were significantly reduced with the combined therapy. Possible mechanisms could be a decrease in antioxidant levels in the early phase, as suggested by previous work. This hypothesis is supported by several studies of injurious insult to the cerebral cortex. In a model based on needlestick injury to the cerebral cortex in young rats, oxidative damage was progressively and markedly reduced over the 6-day survival period due to a self-protective response to prevent cell death.61 In a rat cerebral ischemia model, the serum 8-OHdG level peaked 24 h after reperfusion. In the early injury phase, oxidative stress and excitotoxicity triggered neuronal damage, which may have eventually promoted delayed cell death in the later phase.62
Possible neuroprotective mechanisms of H2 in developing brain
In neonatal HIE, it is important to maintain the growth and development of the developing newborn brain after hypoxic–ischemic insult. To do so, preservation of the architecture and function of the cells of the nervous system and vascular structures are important.
Unlike Xe and Ar, H2 has effectiveness in whole body, not only the central nervous system. Also, not having the single target, H2 protects the cells in multiple approaches mainly anti-oxidation, anti-inflammation, anti-apoptosis, cellular signaling, protection of organelles, and promotion of cellular survival and repair.63 In that way, H2 is assumed to be cytoprotective and neurotrophic for the developing brain after neonatal HIE.
H2 act as a potent radical scavenger, especially of •OH, which is the most potent of free radicals, formed by Fenton reaction in the mammalian cells.2 Apart from direct scavenging action, H2 plays role in enhancing endogenous antioxidative enzymes: superoxide dismutase, catalase, and glutathione peroxidase.64,65,66
Nuclear factor erythroid 2-related factor (Nrf2) is a transcription factor that regulates antioxidants which is activated under oxidative stress. H2 modulates Nrf2. Besides, Nrf2 involves in inflammation, apoptosis, autophagy, ER stress, and cellular signaling.67,68,69,70
H2 plays significant role in anti-inflammation by decreasing circulating tumor necrosis factor-α (TNF-α).71 TNF-α regulates cell survival, immune response, and apoptosis.63 H2 can alter the downstream cascades of TNF-α to alleviate inflammation. One downstream factor regulated by TNF-α is nuclear factor-κB (NF-κB). It is the major regulator of proinflammatory cytokines, which is the key factor that H2 exerts its effect.63 H2 decreased NF-κB activation and subsequent transcription of inflammatory cytokines72 and increased inhibitor of κB in the cytoplasm,66,73,74 leading to reduction of interleukins (ILs) that encourages inflammation and increase in IL-10 (anti-inflammatory cytokines).74,75,76
H2 regulates cell survival and cell death by acting as signaling molecule. H2 alters the genes involving in signaling pathways under oxidative stress.77 In recent studies, H2 is involved in modulation of autophagy, but it varies in different pathological conditions.78 H2 also exerts cytoprotective effects by reducing ER stress.79
H2 involves in repair process of neurodegenerative disorders and promotes vascular integrity. In patients with Parkinson’s disease, H2 not only reduces reactive oxygen species, but also promotes the repair of the injured cells by regeneration of mitochondria.80,81 H2 maintains vascular integrity by inhibition of activation of TNF-α and its downstream elements, such as NF-κB and ILs (e.g., IL-6), thereby restoration of the circulation to facilitate the restoration of the damaged tissues.82
In neonatal brain, more studies need to clarify the mechanisms of neuroprotection by H2 in the developing brain and whether it is harmful. Clinical studies and long-term follow-up studies are required.
Future directions of hydrogen ventilation
H2 as a therapeutic gas can exert benefits in neonatal HIE animals via complex mechanisms. Ventilation is considered to be effective because the blood and tissue levels of H2 reach saturation within 2 or 3 min of the initiation of H2 inhalation.83 The neuroprotective effects could also be due to the shorter distance of gas delivery, with the H2 concentration increasing more rapidly and saturating at a higher level in the brain than in the other organs.84 Its neuroprotective effects are well supported by histological findings from animals.
To determine the effectiveness of H2 ventilation, careful determination of the optimal target severity is also important. Thus, parameters to determine the severity should be well established. Ideally, it should be easy to monitor these parameters as soon as a baby with HIE is delivered and should be continually assessed during the therapeutic interventions.
Generally, H2 therapy is safe and does not interfere with biological processes. However, research into the safety and feasibility of H2 gas in organ systems of large-animal models and human newborns is required. In addition, in terms of HIE, studies should examine how single therapy involving H2 gas or combined therapy with TH can alter the cerebral hemodynamics of newborns.
For clinical application, the H2 gas delivery system should be specifically designed to enable constant monitoring of the H2 concentration.
Finally, the effectiveness of H2 is not completely understood because it does not act through a single target molecule. Multiple simultaneous approaches to clarify the underlying mechanisms are required when outcomes are being studied.
Other potential therapeutic gases for neonatal HIE
Xenon
Xenon (Xe) is a noble inert gas that is a natural component of air (1 in 20 million parts of air) and that is used in adults as a safe and effective inhalational anesthesia.85,86,87 Being an NMDA receptor antagonist, Xe exerts neuroprotective effects by reducing excitotoxicity.88 NMDA is involved in the calcium calmodulin-activated kinase 2 complex, in anti-apoptotic cascades, and in modulating inflammatory cascades.89,90
Due to its potential, the effectiveness of Xe has been studied in neonatal HIE animal models. In neonatal rats, Xe ventilation is neuroprotective at a subanesthetic dose (50%).91 In rat models with moderate HIE, Xe provides neuroprotection, as revealed by histopathological findings and long-term neurological outcomes, when combined with TH.51,92,93,94,95 However, Xe was not effective in a neonatal rat model with severe HIE.96 Xe is safe to use in neonatal piglets.97 Due to this potential efficacy, a Xe recirculating ventilator was designed for neonatal HI piglets to study its feasibility and safety for clinical application in human neonatal HIE.53
In human neonates with HIE, the feasibility of 50% Xe inhalation for 18 h was studied in neonates undergoing TH.98 In the same study, no adverse effect was seen in terms of cardiovascular and respiratory systems, with increased sedation and suppressed seizures. At 18 months of follow-up, no adverse effect was observed. However, current evidence surrounding the safety and efficacy of Xe combined with TH in term or late preterm HIE neonates is inconclusive and necessitates further trials reporting long-term outcomes.99,100
Argon
Another chemically inert noble gas with neuroprotective potential is Argon (Ar), the most abundant such gas in the atmosphere. Ar does not have anesthetic properties at atmospheric pressure, but exerts neuroprotective effects in both in vitro and in vivo mouse models of traumatic brain injury.101 Its potential applications in in vivo and in vitro studies include traumatic brain injury, cerebral ischemia, and HIE.100 In piglets, inhalation of up to 80% Ar in the normoxic state and 50% Ar in the hypoxic state did not alter the hemodynamic status.49 Inhalation of 40–50% Ar augmented hypothermia-induced neuroprotection in perinatal HI piglets by improving cerebral energy metabolism, amplitude-integrated EEG (aEEG) recovery, and histological assessments 48 h after insult.102 The exact mechanisms underlying the neuroprotective effects of Ar are still ambiguous.103
Comparison between hydrogen with Xe and Ar gases
Comparison of potential gaseous adjuncts of TH is summarized in Table 1. Among three gases, H2 has the smallest atomic size. Thus, it can easily cross the blood–brain barrier for neuroprotection. Unlike Xe, which is an NMDA receptor antagonist, H2 does not have single target molecule. H2 may act in multiple pathways, but its mechanisms are still unclear. On the other hand, Ar is also thought to act through γ-aminobutyric acid (GABA) receptor, but investigation is still warranted.104
According to previous reports, H2 exerts its protective effects in low concentration between 2 and 4% via ventilation, whereas Xe and Ar require concentration ~50% in neonatal HIE. Thus, H2 does not require the recirculation ventilator like in the case of Xe. In this way, H2 is easier to apply in clinical settings with lower cost. Time to reach the maximum concentration (Tmax) is not much different from each other when inhaled.32,105
Being produced by fermentation of undigested carbohydrates by intestinal flora, H2 is naturally produced in the intestines of the humans. H2 therapy may perhaps be seemed as complementing the required amount of the lost H2, which is consumed by injurious stimuli. On the other hand, remaining two inert gases are foreign to our body. The disadvantage of H2 is the risk of explosion by the rapid chain reaction if >4% H2 is present in the atmosphere.30 However, the therapeutic range is between 1 and 4%, and due to its small molecular size, it diffuses into the atmosphere easily. Thus, H2 is generally considered safe within its therapeutic range. The disadvantage of Xe is that inhalation of 50% Xe depressed aEEG background in healthy piglets, which can affect interpretation of the outcome.106 Xe is also considered safe within the therapeutic range; however, it exhibits mild respiratory depression if the concentration is >70%.92 Up to now, side effects of Ar in biological system is not clearly understood.
The most advantageous factor of H2 of all is its cheap cost compared to the remaining gases. For one liter, H2 only costs $US0.014/L (~$US100 for a 7000 L gas mixture cylinder containing 3.8% H2 and 96.2% N2, purchased from Takamatsu Teisan Ltd, Kagawa, Japan). Xe costs $US30/L even when recirculated with the designed ventilators.107 Ar is 200 times cheaper than Xe (~$US0.15/L).102 Therefore, H2 therapy may be feasible also in developing countries. According to the above comparison, H2 therapy is the most cost-effective gas, which should be the important candidate as an adjunct of TH in neonatal HIE.
Conclusion
Combined therapy involving medical gases and TH is one of the potential neuroprotective strategies for neonatal HIE. Translational animal model studies have facilitated the clinical use of therapeutic gases. To prove their potential, optimization of the treatment, including therapy concentration and duration, as well as optimal target severity, well-designed clinical trials are required. H2, Xe, and Ar are relatively safe gases, but their long-term neuroprotective results, neurological outcomes, and long-term effects on organ systems require further study.
References
Kajimura, M. et al. Gas biology: tiny molecules controlling metabolic systems. Respir. Physiol. Neurobiol. 184, 139–148 (2012).
Ohsawa, I. et al. Hydrogen acts as a therapeutic antioxidant by selectively reducing cytotoxic oxygen radicals. Nat. Med. 13, 688–694 (2007).
Volpe, J. J. Neurology of the Newborn 6th edn (Elsevier, 2018).
Kriz, J. Inflammation in ischemic brain injury: timing is important. Crit. Rev. Neurobiol. 18, 145–157 (2006).
Hassell, K. J., Ezzati, M., Alonso-Alconada, D., Hausenloy, D. J. & Robertson, N. J. New horizons for newborn brain protection: enhancing endogenous neuroprotection. Arch. Dis. Child Fetal Neonatal Ed. 100, F541–F552 (2015).
Robles, R., Palomino, N. & Robles, A. Oxidative stress in the neonate. Early Hum. Dev. 65(Suppl.), S75–S81 (2001).
Ferriero, D. M. Neonatal brain injury. N. Engl. J. Med. 351, 1985–1995 (2004).
Forman, H. J., Maiorino, M. & Ursini, F. Signaling functions of reactive oxygen species. Biochemistry 49, 835–842 (2010).
Bauer, G. Signaling and proapoptotic functions of transformed cell-derived reactive oxygen species. Prostaglandins Leukot. Essent. Fatty Acids 66, 41–56 (2002).
Gunn, A. J. et al. Therapeutic hypothermia translates from ancient history in to practice. Pediatr. Res. 81, 202–209 (2017).
Hill, A. Pharmacologic considerations in the management of the asphyxiated newborn. Clin. Invest. Med. 8, 355–359 (1985).
Palmer, C. & Vannucci, R. C. Potential new therapies for perinatal cerebral hypoxia–ischemia. Clin. Perinatol. 20, 411–432 (1993).
Jiang, J. Y., Liang, Y. M., Luo, Q. Z. & Zhu, C. Effect of mild hypothermia on brain dialysate lactate after fluid percussion brain injury in rodents. Neurosurgery 54, 713–717 (2004). discussion 717–718.
Erecinska, M., Thoresen, M. & Silver, I. A. Effects of hypothermia on energy metabolism in Mammalian central nervous system. J. Cereb. Blood Flow Metab. 23, 513–530 (2003).
Hagerdal, M., Harp, J., Nilsson, L. & Siesjo, B. K. The effect of induced hypothermia upon oxygen consumption in the rat brain. J. Neurochem. 24, 311–316 (1975).
Kvrivishvili, G. Glycine and neuroprotective effect of hypothermia in hypoxic–ischemic brain damage. NeuroReport 13, 1995–2000 (2002).
Xiong, M., Yang, Y., Chen, G. Q. & Zhou, W. H. Post-ischemic hypothermia for 24h in P7 rats rescues hippocampal neuron: association with decreased astrocyte activation and inflammatory cytokine expression. Brain Res. Bull. 79, 351–357 (2009).
Edwards, A. D. et al. Specific inhibition of apoptosis after cerebral hypoxia–ischaemia by moderate post-insult hypothermia. Biochem. Biophys. Res. Commun. 217, 1193–1199 (1995).
Ohmura, A. et al. Prolonged hypothermia protects neonatal rat brain against hypoxic–ischemia by reducing both apoptosis and necrosis. Brain Dev. 27, 517–526 (2005).
Hasegawa, M., Ogihara, T., Tamai, H. & Hiroi, M. Hypothermic inhibition of apoptotic pathways for combined neurotoxicity of iron and ascorbic acid in differentiated PC12 cells: reduction of oxidative stress and maintenance of the glutathione redox state. Brain Res. 1283, 1–13 (2009).
Truettner, J. S., Alonso, O. F. & Dietrich, W. D. Influence of therapeutic hypothermia on matrix metalloproteinase activity after traumatic brain injury in rats. J. Cereb. Blood Flow Metab. 25, 1505–1516 (2005).
Edwards, A. D. et al. Neurological outcomes at 18 months of age after moderate hypothermia for perinatal hypoxic ischaemic encephalopathy: synthesis and meta-analysis of trial data. BMJ 340, c363 (2010).
Jacobs, S. E. et al. Cooling for newborns with hypoxic–ischaemic encephalopathy. Cochrane Database Syst. Rev. CD003311, https://doi.org/10.1002/14651858.CD003311.pub3 (2013).
Low, E. et al. Cooling and seizure burden in term neonates: an observational study. Arch. Dis. Child Fetal Neonatal Ed. 97, F267–F272 (2012).
Azzopardi, D. et al. Effects of hypothermia for perinatal asphyxia on childhood outcomes. N. Engl. J. Med. 371, 140–149 (2014).
Guillet, R. et al. Seven- to eight-year follow-up of the CoolCap trial of head cooling for neonatal encephalopathy. Pediatr. Res. 71, 205–209 (2012).
Ohta, S. Molecular hydrogen is a novel antioxidant to efficiently reduce oxidative stress with potential for the improvement of mitochondrial diseases. Biochim. Biophys. Acta 1820, 586–594 (2012).
Gardette, B. & Delauze, H. G. Techniques of underwater intervention: means, methods, research and outlook. Bull. Acad. Natl Med. 180, 975–983 (1996).
Ichihara, M. et al. Beneficial biological effects and the underlying mechanisms of molecular hydrogen—comprehensive review of 321 original articles. Med. Gas Res. 5, 12 (2015).
Ohta, S. Molecular hydrogen as a preventive and therapeutic medical gas: initiation, development and potential of hydrogen medicine. Pharm. Ther. 144, 1–11 (2014).
Tamura, T., Hayashida, K., Sano, M., Onuki, S. & Suzuki, M. Efficacy of inhaled HYdrogen on neurological outcome following BRain Ischemia During post-cardiac arrest care (HYBRID II trial): study protocol for a randomized controlled trial. Trials 18, 488 (2017).
Ono, H. et al. A basic study on molecular hydrogen (H2) inhalation in acute cerebral ischemia patients for safety check with physiological parameters and measurement of blood H2 level. Med. Gas Res. 2, 21 (2012).
Rice, J. E. 3rd, Vannucci, R. C. & Brierley, J. B. The influence of immaturity on hypoxic–ischemic brain damage in the rat. Ann. Neurol. 9, 131–141 (1981).
Lingam, I., Avdic-Belltheus, A. & Robertson, N. J. Using animal models to improve care of neonatal encephalopathy. Arch. Dis. Child Educ. Pract. Ed. 101, 271–276 (2016).
Thornton, C., Baburamani, A. A., Kichev, A. & Hagberg, H. Oxidative stress and endoplasmic reticulum (ER) stress in the development of neonatal hypoxic–ischaemic brain injury. Biochem. Soc. Trans. 45, 1067–1076 (2017).
Koehler, R. C., Yang, Z. J., Lee, J. K. & Martin, L. J. Perinatal hypoxic–ischemic brain injury in large animal models: relevance to human neonatal encephalopathy. J. Cereb. Blood Flow Metab. 38, 2092–2111 (2018).
Cai, J. et al. Hydrogen therapy reduces apoptosis in neonatal hypoxia–ischemia rat model. Neurosci. Lett. 441, 167–172 (2008).
Matchett, G. A. et al. Hydrogen gas is ineffective in moderate and severe neonatal hypoxia–ischemia rat models. Brain Res. 1259, 90–97 (2009).
Dobbing, J. & Sands, J. Comparative aspects of the brain growth spurt. Early Hum. Dev. 3, 79–83 (1979).
Kusaka, T. et al. Relationship between cerebral oxygenation and phosphorylation potential during secondary energy failure in hypoxic–ischemic newborn piglets. Pediatr. Res. 65, 317–322 (2009).
Cady, E. B., Iwata, O., Bainbridge, A., Wyatt, J. S. & Robertson, N. J. Phosphorus magnetic resonance spectroscopy 2 h after perinatal cerebral hypoxia–ischemia prognosticates outcome in the newborn piglet. J. Neurochem. 107, 1027–1035 (2008).
Iwata, O. et al. Supra- and sub-baseline phosphocreatine recovery in developing brain after transient hypoxia–ischaemia: relation to baseline energetics, insult severity and outcome. Brain 131, 2220–2226 (2008).
Moroz, T., Banaji, M., Robertson, N. J., Cooper, C. E. & Tachtsidis, I. Computational modelling of the piglet brain to simulate near-infrared spectroscopy and magnetic resonance spectroscopy data collected during oxygen deprivation. J. R. Soc. Interface 9, 1499–1509 (2012).
Moroz, T. et al. Modelling blood flow and metabolism in the piglet brain during hypoxia–ischaemia: simulating brain energetics. Adv. Exp. Med. Biol. 789, 339–344 (2013).
Robertson, N. J. et al. Methyl-isobutyl amiloride reduces brain Lac/NAA, cell death and microglial activation in a perinatal asphyxia model. J. Neurochem. 124, 645–657 (2013).
Bainbridge, A. et al. Brain mitochondrial oxidative metabolism during and after cerebral hypoxia–ischemia studied by simultaneous phosphorus magnetic-resonance and broadband near-infrared spectroscopy. Neuroimage 102(Part 1), 173–183 (2014).
Martin, L. J., Brambrink, A., Koehler, R. C. & Traystman, R. J. Primary sensory and forebrain motor systems in the newborn brain are preferentially damaged by hypoxia–ischemia. J. Comp. Neurol. 377, 262–285 (1997).
Tooley, J. R., Satas, S., Porter, H., Silver, I. A. & Thoresen, M. Head cooling with mild systemic hypothermia in anesthetized piglets is neuroprotective. Ann. Neurol. 53, 65–72 (2003).
Alderliesten, T. et al. Neuroprotection by argon ventilation after perinatal asphyxia: a safety study in newborn piglets. PLoS ONE 9, e113575 (2014).
Chakkarapani, E. et al. A closed-circuit neonatal xenon delivery system: a technical and practical neuroprotection feasibility study in newborn pigs. Anesth. Analg. 109, 451–460 (2009).
Chakkarapani, E., Thoresen, M., Liu, X., Walloe, L. & Dingley, J. Xenon offers stable haemodynamics independent of induced hypothermia after hypoxia–ischaemia in newborn pigs. Intens. Care Med. 38, 316–323 (2012).
Faulkner, S. et al. Xenon augmented hypothermia reduces early lactate/N-acetylaspartate and cell death in perinatal asphyxia. Ann. Neurol. 70, 133–150 (2011).
Faulkner, S. D. et al. A xenon recirculating ventilator for the newborn piglet: developing clinical applications of xenon for neonates. Eur. J. Anaesthesiol. 29, 577–585 (2012).
Foster, K. A. et al. An improved survival model of hypoxia/ischaemia in the piglet suitable for neuroprotection studies. Brain Res. 919, 122–131 (2001).
Domoki, F. et al. Hydrogen is neuroprotective and preserves cerebrovascular reactivity in asphyxiated newborn pigs. Pediatr. Res. 68, 387–392 (2010).
Varga, V. et al. Molecular hydrogen alleviates asphyxia-induced neuronal cyclooxygenase-2 expression in newborn pigs. Acta Pharm. Sin. 39, 1273–1283 (2018).
Nemeth, J. et al. Molecular hydrogen affords neuroprotection in a translational piglet model of hypoxic–ischemic encephalopathy. J. Physiol. Pharm. 67, 677–689 (2016).
Olah, O., Toth-Szuki, V., Temesvari, P., Bari, F. & Domoki, F. Delayed neurovascular dysfunction is alleviated by hydrogen in asphyxiated newborn pigs. Neonatology 104, 79–86 (2013).
Htun, Y. et al. Hydrogen ventilation combined with mild hypothermia improves short-term neurological outcomes in a 5-day neonatal hypoxia–ischaemia piglet model. Sci. Rep. 9, 4088 (2019).
Thoresen, M., Simmonds, M., Satas, S., Tooley, J. & Silver, I. A. Effective selective head cooling during posthypoxic hypothermia in newborn piglets. Pediatr. Res. 49, 594–599 (2001).
Purushothuman, S. & Stone, J. The reaction of cerebral cortex to a nearby lesion: damage, survival, self-protection. Brain Res. 1601, 52–63 (2015).
Won, M. H. et al. The alterations of N-methyl-d-aspartate receptor expressions and oxidative DNA damage in the CA1 area at the early time after ischemia–reperfusion insult. Neurosci. Lett. 301, 139–142 (2001).
Tao, G., Song, G. & Qin, S. Molecular hydrogen: current knowledge on mechanism in alleviating free radical damage and diseases. Acta Biochim. Biophys. Sin. (Shanghai) 51, 1189–1197 (2019).
Huang, Y. et al. Beneficial effects of hydrogen gas against spinal cord ischemia-reperfusion injury in rabbits. Brain Res. 1378, 125–136 (2011).
Xin, H. G. et al. Consumption of hydrogen-rich water alleviates renal injury in spontaneous hypertensive rats. Mol. Cell. Biochem. 392, 117–124 (2014).
Shi, Q. et al. Hydrogen-rich saline attenuates acute renal injury in sodium taurocholate-induced severe acute pancreatitis by inhibiting ROS and NF-kappaB pathway. Mediat. Inflamm. 2015, 685043 (2015).
Song, G. et al. Molecular hydrogen stabilizes atherosclerotic plaque in low-density lipoprotein receptor-knockout mice. Free Radic. Biol. Med. 87, 58–68 (2015).
Gold, R. et al. Placebo-controlled phase 3 study of oral BG-12 for relapsing multiple sclerosis. N. Engl. J. Med. 367, 1098–1107 (2012).
Ma, Q. Role of nrf2 in oxidative stress and toxicity. Annu. Rev. Pharm. Toxicol. 53, 401–426 (2013).
Liu, L. et al. Inhalation of hydrogen gas attenuates brain injury in mice with cecal ligation and puncture via inhibiting neuroinflammation, oxidative stress and neuronal apoptosis. Brain Res. 1589, 78–92 (2014).
Gharib, B. et al. Anti-inflammatory properties of molecular hydrogen: investigation on parasite-induced liver inflammation. C. R. Acad. Sci. III 324, 719–724 (2001).
Tian, Y. et al. Effects of hydrogen-rich saline on hepatectomy-induced postoperative cognitive dysfunction in old mice. Mol. Neurobiol. 54, 2579–2584 (2017).
Shao, A. et al. Hydrogen-rich saline attenuated subarachnoid hemorrhage-induced early brain injury in rats by suppressing inflammatory response: possible involvement of NF-kappaB pathway and NLRP3 pnflammasome. Mol. Neurobiol. 53, 3462–3476 (2016).
Zhang, G. et al. The anti-inflammatory effect of hydrogen on lung transplantation model of pulmonary microvascular endothelial cells during cold storage period. Transplantation 102, 1253–1261 (2018).
Chen, L. et al. Hydrogen treatment protects mice against chronic pancreatitis by restoring regulatory T cells loss. Cell. Physiol. Biochem. 44, 2005–2016 (2017).
Lin, C. P., Chuang, W. C., Lu, F. J. & Chen, C. Y. Anti-oxidant and anti-inflammatory effects of hydrogen-rich water alleviate ethanol-induced fatty liver in mice. World J. Gastroenterol. 23, 4920–4934 (2017).
Iuchi, K. et al. Molecular hydrogen regulates gene expression by modifying the free radical chain reaction-dependent generation of oxidized phospholipid mediators. Sci. Rep. 6, 18971 (2016).
Jiang, X. et al. FoxO1-mediated autophagy plays an important role in the neuroprotective effects of hydrogen in a rat model of vascular dementia. Behav. Brain Res. 356, 98–106 (2019).
Gao, Y. et al. Hydrogen gas attenuates myocardial ischemia–reperfusion injury independent of postconditioning in rats by attenuating endoplasmic reticulum stress-induced autophagy. Cell. Physiol. Biochem. 43, 1503–1514 (2017).
Ishibashi, T. Therapeutic efficacy of molecular hydrogen: a new mechanistic insight. Curr. Pharm. Des. 25, 946–955 (2019).
Yoritaka, A. et al. Pilot study of H(2) therapy in Parkinson’s disease: a randomized double-blind placebo-controlled trial. Mov. Disord. 28, 836–839 (2013).
Sakai, T. et al. Consumption of water containing over 3.5 mg of dissolved hydrogen could improve vascular endothelial function. Vasc. Health Risk Manag. 10, 591–597 (2014).
Hayashida, K. et al. Inhalation of hydrogen gas reduces infarct size in the rat model of myocardial ischemia–reperfusion injury. Biochem. Biophys. Res. Commun. 373, 30–35 (2008).
Yamamoto, R., Homma, K., Suzuki, S., Sano, M. & Sasaki, J. Hydrogen gas distribution in organs after inhalation: real-time monitoring of tissue hydrogen concentration in rat. Sci. Rep. 9, 1255 (2019).
Rossaint, R. et al. Multicenter randomized comparison of the efficacy and safety of xenon and isoflurane in patients undergoing elective surgery. Anesthesiology 98, 6–13 (2003).
Cullen, S. C. & Gross, E. G. The anesthetic properties of xenon in animals and human beings, with additional observations on krypton. Science 113, 580–582 (1951).
Cullen, S. C. & Pittinger, C. B. Clinical and laboratory observations of the use of xenon for anesthesia. Surg. Forum. 38th Congress 361–366 (1953).
Franks, N. P., Dickinson, R., de Sousa, S. L., Hall, A. C. & Lieb, W. R. How does xenon produce anaesthesia? Nature 396, 324 (1998).
Petzelt, C. P., Kodirov, S., Taschenberger, G. & Kox, W. J. Participation of the Ca(2+)-calmodulin-activated Kinase II in the control of metaphase–anaphase transition in human cells. Cell Biol. Int. 25, 403–409 (2001).
Ma, D. et al. Xenon preconditioning reduces brain damage from neonatal asphyxia in rats. J. Cereb. Blood Flow Metab. 26, 199–208 (2006).
Dingley, J., Tooley, J., Porter, H. & Thoresen, M. Xenon provides short-term neuroprotection in neonatal rats when administered after hypoxia–ischemia. Stroke 37, 501–506 (2006).
Dingley, J., Hobbs, C., Ferguson, J., Stone, J. & Thoresen, M. Xenon/hypothermia neuroprotection regimes in spontaneously breathing neonatal rats after hypoxic–ischemic insult: the respiratory and sedative effects. Anesth. Analg. 106, 916–923 (2008), table of contents.
Liu, X., Dingley, J., Scull-Brown, E. & Thoresen, M. Adding 5 h delayed xenon to delayed hypothermia treatment improves long-term function in neonatal rats surviving to adulthood. Pediatr. Res. 77, 779–783 (2015).
Thoresen, M., Hobbs, C. E., Wood, T., Chakkarapani, E. & Dingley, J. Cooling combined with immediate or delayed xenon inhalation provides equivalent long-term neuroprotection after neonatal hypoxia-ischemia. J. Cereb. Blood Flow Metab. 29, 707–714 (2009).
Hobbs, C. et al. Xenon and hypothermia combine additively, offering long-term functional and histopathologic neuroprotection after neonatal hypoxia/ischemia. Stroke 39, 1307–1313 (2008).
Sabir, H., Osredkar, D., Maes, E., Wood, T. & Thoresen, M. Xenon combined with therapeutic hypothermia is not neuroprotective after severe hypoxia–ischemia in neonatal rats. PLoS ONE 11, e0156759 (2016).
Chakkarapani, E. et al. Xenon enhances hypothermic neuroprotection in asphyxiated newborn pigs. Ann. Neurol. 68, 330–341 (2010).
Dingley, J. et al. Xenon ventilation during therapeutic hypothermia in neonatal encephalopathy: a feasibility study. Pediatrics 133, 809–818 (2014).
Ruegger, C. M., Davis, P. G. & Cheong, J. L. Xenon as an adjuvant to therapeutic hypothermia in near-term and term newborns with hypoxic–ischaemic encephalopathy. Cochrane Database Syst. Rev. 8, CD012753 (2018).
Hollig, A. et al. Argon: systematic review on neuro- and organoprotective properties of an “inert” gas. Int. J. Mol. Sci. 15, 18175–18196 (2014).
Loetscher, P. D. et al. Argon: neuroprotection in in vitro models of cerebral ischemia and traumatic brain injury. Crit. Care 13, R206 (2009).
Broad, K. D. et al. Inhaled 45–50% argon augments hypothermic brain protection in a piglet model of perinatal asphyxia. Neurobiol. Dis. 87, 29–38 (2016).
Koziakova, M. et al. Noble gas neuroprotection: xenon and argon protect against hypoxic–ischaemic injury in rat hippocampus in vitro via distinct mechanisms. Br. J. Anaesth. 123, 601–609 (2019).
Ben-Ari, Y., Khalilov, I., Kahle, K. T. & Cherubini, E. The GABA excitatory/inhibitory shift in brain maturation and neurological disorders. Neuroscientist 18, 467–486 (2012).
Katz, I., Murdock, J., Palgen, M., Pype, J. & Caillibotte, G. Pharmacokinetic analysis of the chronic administration of the inert gases Xe and Ar using a physiological based model. Med. Gas Res. 5, 8 (2015).
Sabir, H. et al. Xenon depresses aEEG background voltage activity whilst maintaining cardiovascular stability in sedated healthy newborn pigs. J. Neurol. Sci. 363, 140–144 (2016).
Amer, A. R. & Oorschot, D. E. Xenon combined with hypothermia in perinatal hypoxic–ischemic encephalopathy: a noble gas, a noble mission. Pediatr. Neurol. 84, 5–10 (2018).
Acknowledgements
This study was financially supported by Grants-in-Aid for Scientific Research (KAKENHI) from the Japan Society for the Promotion of Science (number 16K10092 to T.K., and numbers 19K08253, 16H06276, 16K19685, and 15KK0311 to S.N.), grants from the Kagawa University Faculty of Medicine School of Medicine Alumni Association Sanjukai Research Aid (numbers R1-1 and 25-2), and a scholarship from the Honjo International Scholarship Foundation (to Y.H.).
Author information
Authors and Affiliations
Contributions
Y.H. and T.K. designed the study and drafted the article. Y.H., S.N., and T.K. revised it critically and contributed to the final approval of the version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Htun, Y., Nakamura, S. & Kusaka, T. Hydrogen and therapeutic gases for neonatal hypoxic–ischemic encephalopathy: potential neuroprotective adjuncts in translational research. Pediatr Res 89, 753–759 (2021). https://doi.org/10.1038/s41390-020-0998-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-020-0998-z
This article is cited by
-
Hydrogen gas can ameliorate seizure burden during therapeutic hypothermia in asphyxiated newborn piglets
Pediatric Research (2024)
-
Impact of hydrogen gas inhalation during therapeutic hypothermia on cerebral hemodynamics and oxygenation in the asphyxiated piglet
Scientific Reports (2023)
-
Conflicting findings on the effectiveness of hydrogen therapy for ameliorating vascular leakage in a 5-day post hypoxic-ischemic survival piglet model
Scientific Reports (2023)
-
Molecular Hydrogen: an Emerging Therapeutic Medical Gas for Brain Disorders
Molecular Neurobiology (2023)
-
Emerging therapies and management for neonatal encephalopathy—controversies and current approaches
Journal of Perinatology (2021)
