
Abstract
Background
Physical activity (PA) and obesity were linked with poor cognition. Our study assessed PA interventions could improve domain-specific cognition among overweight/obese youth.
Methods
Systematically searched PubMed to identify relevant studies published up to October 2019. Standardized mean differences (SMD) of pre−post intervention were calculated in meta-analysis. The level of study heterogeneity represented by I2 was interpreted as small (I2 ≤ 25%), moderate (25% < I2 ≤ 50%), substantial (50% < I2 ≤ 75%), or considerable (I2 > 75%).
Results
Seventeen studies met the inclusion criteria; eight were included in the meta-analysis. Meta-analysis revealed that PA interventions improved core executive functions (core-EFs) (SMD = 0.301; 95% CI = 0.002−0.600; I2% = 80.6%) and non-EFs (SMD = 0.159; 95% CI = 0.029−0.289; I2% = 0.0%), but not metacognition and academic performance. Core-EFs benefited from enriched PA (SMD = 0.535; 95% CI = 0.020−1.051; I2% = 72.0%) and enhanced and enriched PA (SMD = 1.005; 95% CI = 0.017−1.993; I2% = 90.8%) interventions, while the non-EFs benefited more from enhanced PA (SMD = 0.166; 95% CI = 0.018−0.314; I2% = 0.0%). Interventions with a favorable effect on adiposity measures resulted in a significantly greater improvement in core-EFs (SMD = 0.438; 95% CI = 0.047−0.829; I2% = 58.8%) than those with no effects.
Conclusions
PA interventions can improve several domains of cognition, especially core-EFs and non-EFs, and the effects are affected by PA characteristics among overweight and obese youth.
Impact
-
Our study is the first to quantify the effect of PA interventions on CP among overweight or obese children and adolescents.
-
Physical activity interventions positively affect cognitive performance, especially core executive functions (core-EFs) and non-EFs.
-
Physical activity interventions seem to not positively affect metacognition (higher-level EFs and cognitive life skills) and academic performance.
-
Physical task characteristics could influence the effect of chronic exercise on cognitive performance.
-
Short-term physical activity programs may be particularly beneficial to affect core-EFs.
Similar content being viewed by others

Introduction
Childhood obesity has become a major public health problem worldwide. In addition to the well-established adverse effects of obesity on health, it has also been linked to poor cognitive performance (CP).1,2,3 Lack of physical activity (PA) has been recognized as an important risk factor for obesity.4 Evidence consistently supports that PA has favorable effects on cognition function, including angiogenesis, oxygen saturation, neurotransmitter levels.5,6 Another study demonstrated that PA intervention significantly enhanced CP and brain function compared with the control group.7
Over the past two decades, there have been a growing number of review studies examining the relationships between PA and CP in children and adolescents.8,9,10,11,12,13,14,15,16,17,18,19 Some reviews have focused on the characteristics of PA interventions in terms of intensity, frequency, dose, or intervention duration.8,9,10,11,12,13,14,15,16 Recently, a number of meta-analyses have been conducted to subdivide CP into core executive functions (core-EFs) (e.g., inhibition, working memory, cognitive flexibility), higher-level EFs (e.g., abstract reasoning, planning, problem solving), non-EFs (e.g., nonverbal ability, spatial ability), life skills (e.g., goal-setting, self-regulation), and academic performance (AP).19,20 The above evidence has suggested that PA intervention programs benefit multiple facets of CP in children and adolescents.
In addition to the characteristics of PA interventions and contextual factors, weight status has been recognized as an important moderator for CP. Earlier evidence indicated that overweight or obese children involved in PA interventions would benefit more in terms of CP than children and adolescents with normal weight,18 a finding supported by Pesce et al.21 Numerous studies have demonstrated that children/adolescents with obesity have poor CP, such as reduced attentional focus, greater problems in visuospatial organization and nonverbal ability, impaired working memory, and decision-making disorders.22,23,24,25,26 However, only a few reviews have evaluated the effects of PA interventions on CP in overweight and obese children and adolescents. Recently, Bustamante et al.6 reviewed the effects of PA interventions on CP in overweight and obese youth, but they did not distinguish between the CP outcomes that improved and those that did not.
Therefore, this systematic review and meta-analysis investigated the effects of PA interventions on domain-specific CP in overweight and obese children and adolescents.
Methods
This study was performed following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)27 and the Cochrane Collaboration Handbook.28 The protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO, CRD42019127343).
Selection criteria
Studies included in the review needed to meet the following inclusion criteria: (1) were PA intervention studies, including randomized controlled trials (RCTs), non-RCTs, and controlled pre−post studies; (2) included subjects aged < 18 years; (3) used standard criteria defining overweight or obesity, e.g., used sex-age-specific body mass index (BMI) or fat mass percentage ≥ 85th percentile; (4) studies reported any type of PA programs and provided a comprehensive view of PA effects on the different facets of children’ cognition; and (5) were published in English.
Study exclusions: (1) included participants with diagnosed developmental disabilities that may have interfered with them performing exercises; (2) employed acute exercise; and (3) were conference abstracts, commentaries, and review articles.
Search strategy
PubMed was searched for relevant studies published up to October 2019. The search strings consisted of keywords related to PA and CP, child and adolescent, overweight and obesity, and intervention study. Details of the search strategies are presented in Appendix 1. In addition, we reviewed the reference lists of included papers and relevant review papers to identify more relevant studies.
After deletion of duplicate records, two authors (Y.L. and X.S.) independently conducted title scans and abstract reviewing, and reviewed the full articles to assess eligibility for inclusion according to selection criteria. They jointly determined the list of articles for the full-text review, independently reviewed the full texts of all articles in the list, and determined the final pool of articles included in the review. Any disagreements were discussed with a third reviewer (Y.W.) until a consensus was achieved.
Data extraction and study quality assessment
Each paper received a double review for data abstraction; the second reviewer checked the first reviewer’s data abstraction for completeness and accuracy. Reviewers extracted information on study characteristics, study participants, eligibility criteria, intervention components, and method of assessment and outcome measures. According to the Cochrane Collaboration Handbook,28 the mean and SD values of pre-to-post intervention difference were first extracted. For each study, we calculated the net changes as the difference in the mean changes in CP parameters (mean changes in CP parameters in the intervention group minus mean changes in the control group). The variances for net changes in CP parameters were not reported directly in some studies. Therefore, they were calculated from confidence intervals (CIs) for the intervention and control groups using standard methods. For studies that reported CP parameters data before and after the intervention, we calculated the variance in the mean changes in CP parameters using correlation coefficient methods.28
The US National Institutes of Health (NIH)’s Quality Assessment Tool for Controlled Intervention Studies (https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools) and Quality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group (https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools) were used to assess the quality of each included study. These assessment tools rate each study based on 14 criteria (controlled studies) and 12 criteria (without control). For each criterion, a score of one was assigned if “yes” was the response, whereas a score of zero was assigned otherwise (i.e., an answer of “no,” “not applicable,” “not reported,” or “cannot determine”). A study-specific global score ranging from zero to 14 or 12 was calculated by summing up scores across all criteria. This assessment measured the strength of scientific evidence, but was not used to determine the inclusion of studies. The assessment results were shown in Supplemental Table S1. Of the 17 studies, 10 were RCTs and one was a non-RCT (with obese control), in which quality was assessed using the former criteria. In general, those studies were of fairly high quality, with a mean quality score of 8.8. Seven studies included information regarding the adequacy of randomization and concealment of treatment allocation, while few studies properly described the double blinding method used. Of six studies in which quality was assessed using the 12 criteria (without control), five studies scored eight points and one study scored nine points.
Statistical analysis
Meta-analysis was performed using findings from eight of the 17 included studies, to estimate the pooled effects of PA on CP. Only those studies provided needed information for pre- and postintervention measurements and included a control group in the meta-analysis. Meta-analysis was performed for four specific CP domains, respectively: (1) core-EFs, (2) non-EFs, (3) metacognition (higher-level EFs and cognitive life skills), and (4) AP. If studies included two intervention groups, the results were analyzed as independent samples; for studies that reported multiple results on one CP task, the results of the more executive-demanding condition was included; when studies conducted two or more measurements, only the last measurement was included.19
Considering the different outcomes and units of cognitive measures used in the studies, standardized mean differences (SMD) of pre−post intervention were calculated and given weight by their inverse variance. Study heterogeneity was assessed using the I2 index. The level of heterogeneity represented by I2 was interpreted as small (I2 ≤ 25%), moderate (25% < I2 ≤ 50%), substantial (50% < I2 ≤ 75%), or considerable (I2 > 75%). In our meta-analysis, a fixed-effect model was estimated when modest to moderate heterogeneity was present, and a random-effects model was estimated when substantial to considerable heterogeneity was present.
To investigate potential sources of heterogeneity, subgroup analyses were performed based on categorical variables including intervention modality (type of intervention, task characteristics), intervention time and duration, adiposity effects, and age. In this review, the type of intervention was classified as: (1) After-school PA: exercise programs that take place after school time, in or out of a school setting; (2) Curricular PA: activities in classes of physical education; (3) Integrated PA: such as active breaks, physically active academic lessons, active recess, or lunchtime PA.19 For the task characteristics, we distinguished between quantitative and qualitative characteristics of the PA intervention and divided them into three parts: (1) Enhanced PA: increasing PA time; (2) Enriched PA: increasing nonphysical-coordinative and/or cognitive demands of the PA tasks; (3) Both (enhanced and enriched PA).19
Finally, sensitivity analyses were conducted by excluding one study at a time from the meta-analysis. Publication bias was assessed by visual inspection of the funnel plot and Begg’s and Egger’s tests. All statistical analyses were conducted using the Stata software version 14 (Stata Corp., College Station, Texas, USA). All analyses used two-sided tests, and P values < 0.05 were considered statistically significant.
Results
Main study characteristics and findings
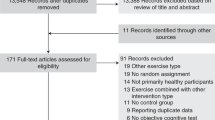
We identified 171 relevant papers, and 25 full papers were retrieved. Seventeen studies29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45 were included in this review, and eight provided adequate data for meta-analysis (Fig. 1).

Flowchart of literature search and assessment of articles.
The main characteristics and findings of the 17 studies were shown in Supplemental Table S2. They were published between 2007 and 2018. Ten studies (59%) were RCTs, seven studies (41%) were non-RCTs. These studies were conducted in 11 countries: the United States (five studies), the United Kingdom (two studies), Italy (two studies), Spain (one study), Canada (one study), France (one study), Denmark (one study), Taiwan (one study), China (one study), Belgium (one study), and Iran (one study). The studies varied in sample size, ranged from 27 to 172, with a median of 74. Mean age of the subjects included in the studies ranged from 8.0 to 16.5 years.
Nine intervention studies tested after-school PA programs, three were performed during curricular school time, and five studies developed integrated PA interventions (Supplemental Table S2). Overall, the interventions resulted in an increased PA time from 20 to 60 min per day, and/or 2−6 times of PA per week. Four studies included more than one intervention group, which differed in their exercise intensity or PA type, and five studies had no comparable control groups. The length of interventions ranged broadly from 4 weeks to 1 year; one study, however, did not report this information.
Measurements of CP and AP, and intervention effects
Nine of the 17 studies provided information about PA measurement (Supplemental Table S3); 13 studies assessed core-EFs, including inhibition control (11 studies), working memory (two studies), and cognitive flexibility (two studies). Seven studies assessed non-EFs, and eight studies assessed metacognition, including higher-level EF (three studies) and cognitive life skills (six studies). Only three studies assessed AP. Two of the 17 studies with more than one intervention group found that PA interventions and CP improvement may have dose−response relationships.
Sixteen studies reported some improvement in CP. Ten studies reported significant improvement in weight status, and the remaining seven studies reported no changes in weight status or did not report. Regarding AP, two out of three studies resulted in significant improvements in AP, while one showed no effect (Supplemental Table S3).
Meta-analysis: intervention effects on CP
As shown in Fig. 2, eight studies were included in the meta-analysis (11 for core-EFs, 10 for non-EFs, seven for metacognition). The pooled SMD of core-EFs was 0.301 (95% CI = 0.002−0.600), with large heterogeneity (I2 = 80.6%, P < 0.001). Regarding inhibition control, the pooled SMD was 0.254 (95% CI = −0.138−0.646), with large heterogeneity (I2 = 84.3%, P < 0.001); for cognitive flexibility, the pooled SMD was 0.438 (95% CI = 0.047−0.829), with medium heterogeneity (I2 = 58.8%, P = 0.088).

Pooled estimated effect size for core-EFs (a), non-EFs (b), and metacognition (c). Note: Positive effect size (ES) values indicate higher score in outcomes in favor of the intervention group. EF Executive Function, IG Intervention Group, NI the number of intervention, NC the number of control, CAS Cognitive Assessment System, SCWT the Stroop Color and Word Test, SCT Social Cognitive Theory, BRIEF the Behavior Rating Inventory of Executive Function, RCFT the Rey Complex Figure Test, D-KEFS the Delis–Kaplan Executive Function System, WCST Wisconsin Card Sorting Test. IG1 and IG2 were expressed as two different intervention groups in one study.
The pooled SMD of metacognition was 0.375 (95% CI = −0.087−0.837), with large heterogeneity (I2 = 89.9%, P < 0.001). For higher-level EFs, the SMD was 0.189 (95% CI = −0.020−0.398) with small heterogeneity (I2 = 0.0%, P = 0.769). For cognitive life skills, the SMD was 0.598 (95% CI = −0.429−1.625) with large heterogeneity (I2 = 96.1%, P < 0.001). The pooled SMD of non-EFs was 0.159 (95% CI = 0.029−0.289), with small heterogeneity (I2 = 0.0%, P = 0.934) (Fig. 2). The pooled SMD of AP was 0.024 (95% CI = −0.177−0.224), with small heterogeneity (I2 = 0.0%, P = 0.914) (Supplemental Fig. S1).
Stratified analysis
In the subgroup analyses, the effect of PA interventions on EFs was significantly moderated by task characteristics, adiposity effect, intervention duration, and age (Table 1). The core-EFs benefited from enriched PA (SMD = 0.535; 95% CI = 0.020−1.051) and enhanced and enriched PA (SMD = 1.005; 95% CI = 0.017−1.993) interventions, while the non-EFs benefited from enhanced PA (SMD = 0.166; 95% CI = 0.018−0.314) interventions. Studies having a significant positive effect on adiposity measures resulted in a significantly greater improvements in core-EFs (SMD = 0.438; 95% CI = 0.047−0.829) than those which did not improve adiposity measures. The intervention duration ≤12 weeks resulted in greater improvement in core-EFs (SMD = 0.438; 95% CI = 0.047−0.829). When interventions were stratified by mean baseline age, the improvement in core-EFs was greater in children aged >12 years.
Sensitivity analysis
Two studies40,45 were major contributors to the high heterogeneity by the sensitivity analysis in core-EFs and metacognition, respectively. After excluding them, the pooled SMD of core-EFs was 0.183 (95% CI = −0.030−0.395), and heterogeneity was medium (I2 = 57.7%, P = 0.011); the pooled SMD of metacognition was 0.139 (95% CI = −0.020−0.298), and heterogeneity was small (I2 = 0.0%, P = 0.870) (Supplemental Table S4).
Publication bias
There was no indication of publication bias for core-EFs and non-EFs as indicated by funnel plots (Supplemental Fig. S2). Egger’s and Begg’s tests yielded results similar to the funnel plots: core-EFs (Egger P = 0.953; Begg P = 0.640), non-EFs (Egger P = 0.207; Begg P = 0.210), metacognition (Egger P = 0.823; Begg P = 0.548), and AP (Egger P = 0.742; Begg P = 0.308) (Supplemental Table S5).
Discussion
To our knowledge, this is the first systematic review and meta-analysis to summarize evidence regarding the effect of PA interventions on overweight/obese children and adolescents’ CP and its domains. Overall, this study shows that PA interventions are useful strategies to foster the development of CP in overweight/obese children and adolescents, especially regarding core-EFs and non-EFs. In addition, the effect of PA on core-EFs and non-EFs is moderated by intervention modality.
The available evidences have indicated that PA interventions may have a favorable effect on CP in children and adolescents.8,9,10,11,12,13,14,15,16,17,18,19 In a systematic review, Alvarez-Bueno et al.19 showed that PA improves several domains of CP in youth, including non-EFs, core-EFs, and metacognition, without giving a specific indication of the youths’ overweight status. PA has been demonstrated to have a small but significant effect on inhibition control, which was moderated by BMI.18 Crova et al.36 also found the relationship between PA and CP was contradictory between normal and overweight children. Although they tend to be closely related with various aspects of cognitive impairments compared with those having normal weight,23,24 a few studies have focused on overweight or obese children and adolescents. Our studies have found that PA intervention programs have a significant positive effect on non-EFs and core-EFs, especially in terms of cognitive flexibility. Furthermore, we also observed in the subgroup analysis that core-EFs benefit more from PA if they are accompanied by a significant improvement in adiposity. Our findings extend a 2018 systematic review published by Bustamante et al.6 In that study they only focused on the qualitative description of PA programs on CP, without further investigation about specific CP domains.
In our study, the core-EFs benefited from enriched PA, and enhanced and enriched PA interventions, while non-EFs were improved mostly in enhanced PA interventions. Our results are supported by Alvarez-Bueno et al.19 Developmental evidence concerning the beneficial effects of PA interventions on CP has been growing during the last decades. However, not all exercise produces the same results. Animal studies have shown that complex and random activities result in greater neural growth in the hippocampus, cerebellum, and cerebral cortices than simple and repetitive actions.46 Best et al.47 reported that PA requiring complex, controlled, and adaptive cognition and movement have a greater impact on EFs. Based on the current evidence, a clear conclusion could not be drawn. It suggests enriched or mixed PA programs with flexible cognitive-oriented tasks making greater coordinative and cognitive demands appear to improve children’s core-EFs better than enhanced PA only programs.
Some clinical studies have shown that short duration and moderately intense exercise may influence cognition due to feedback from the vagus nerve to the nucleus of the solitary tract, inducing synthesis and release of noradrenaline from the locus coeruleus.48 Our study found that PA intervention duration was a moderator, especially for core-EFs, while metacognition was not moderated by any of the intervention modalities in our review. One potential explanation may be the limited number of studies dealing with metacognition. It should also be noted that the beneficial effect of PA on CP after a longer period postintervention remains unclear; there is a lack of follow-up studies measuring outcomes after intervention cessation.
It seems study participants’ age might modify the intervention effects on core-EFs: those >12 years old had more benefits from PA interventions than those ≤12 years. Previous studies indicated that PA might have different influences on CP at different ages,11 but findings were mixed. This was because almost all of these studies used age as a confounding factor in their analysis. Furthermore, in our review, 10 of the 17 studies reported the mean age of participants was >12 years old, which may impact the reliability of our results.
While a number of studies evaluated the PA interventions on CP, three of 17 studies reported the AP. Systematic reviews revealed that there is strong evidence for beneficial effects of PA interventions on AP.13,17 Although the achievement in AP is closely related with the improvement in CP,49 in the present study no effect of PA interventions on AP was observed, which may be attributed to the limited studies conducted on overweight or obese children and adolescents.
Our study has several main strengths. First, this review includes intervention studies and excludes observational or longitudinal studies. Second, our study is the first to quantify the effect of PA interventions on CP among overweight or obese children and adolescents. Third, this study takes into consideration the role of various key moderators such as the type of intervention, task characteristics, and intervention length and duration.
This study has some limitations. First, it includes various CP tasks, which may have led to the high heterogeneity in this review. Second, we only include articles published in English. Third, publication bias is possible, though no evidence for this is identified. Fourth, the included studies use different study designs, eligibility criteria, follow-up times, and intervention approaches. Fifth, the fact that no gold standard measurement of CPs was used in the included studies thus far may have led to a moderate-to-large amount of heterogeneity in the CP outcomes, but measurements were standardized by calculating the ES. Furthermore, a relatively small number of studies are available and included in our review. Thus, caution in generalizing these results is advisable.
In conclusion, our study shows that physical activity interventions affect cognitive performance of overweight/obese children and adolescents. Physical activity interventions are a promising way to promote the development of cognitive performance, especially core-EFs and non-EFs. Moreover, physical activity interventions implemented with enriched physical activity and short-term physical activity programs may be particularly beneficial to affect core-EFs among overweight/obese children and adolescents.
References
Torrijos-Nino, C. et al. Physical fitness, obesity, and academic achievement in schoolchildren. J. Pediatr. 165, 104–109 (2014).
Ishihara, T. et al. Direct and indirect relationships of physical fitness, weight status, and learning duration to academic performance in Japanese schoolchildren. Eur. J. Sport Sci. 18, 286–294 (2018).
Tandon, P., Thompson, S., Moran, L. & Lengua, L. Body mass index mediates the effects of low income on preschool children’s executive control, with implications for behavior and academics. Child Obes. 11, 569–576 (2015).
Steinbeck, K. S. The importance of physical activity in the prevention of overweight and obesity in childhood: a review and an opinion. Obes. Rev. 2, 117–130 (2001).
Chaddock, L. et al. A functional MRI investigation of the association between childhood aerobic fitness and neurocognitive control. Biol. Psychol. 89, 260–268 (2012).
Bustamante, E. E., Williams, C. F. & Davis, C. L. Physical activity interventions for neurocognitive and academic performance in overweight and obese youth: a systematic review. Pediatr. Clin. North Am. 63, 459–480 (2016).
Hillman, C. H. et al. Effects of the FITKids randomized controlled trial on executive control and brain function. Pediatrics 134, e1063–e1071 (2014).
Santana, C. C. A. et al. Physical fitness and academic performance in youth: a systematic review. Scand. J. Med. Sci. Sports 27, 579–603 (2017).
Jackson, W. M., Davis, N., Sands, S. A., Whittington, R. A. & Sun, L. S. Physical activity and cognitive development: a meta-analysis. J. Neurosurg. Anesthesiol. 28, 373–380 (2016).
Marques, A., Santos, D. A., Hillman, C. H. & Sardinha, L. B. How does academic achievement relate to cardiorespiratory fitness, self-reported physical activity and objectively reported physical activity: a systematic review in children and adolescents aged 6-18 years. Br. J. Sports Med. 52, 1039 (2018).
Fedewa, A. L. & Ahn, S. The effects of physical activity and physical fitness on children’s achievement and cognitive outcomes: a meta-analysis. Res. Q. Exerc. Sport 82, 521–535 (2011).
Lees, C. & Hopkins, J. Effect of aerobic exercise on cognition, academic achievement, and psychosocial function in children: a systematic review of randomized control trials. Prev. Chronic Dis. 10, E174 (2013).
Singh, A. S. et al. Effects of physical activity interventions on cognitive and academic performance in children and adolescents: a novel combination of a systematic review and recommendations from an expert panel. Br. J. Sports Med. 53, 640–647 (2019).
Vazou, S., Pesce, C., Lakes, K. & Smiley-Oyen, A. More than one road leads to Rome: meta-analysis of physical activity interventions on cognition in children. Int. J. Sport Exerc. Psychol. 17, 153–178 (2019).
Donnelly, J. E. et al. Physical activity, fitness, cognitive function, and academic achievement in children: a systematic review. Med. Sci. Sports Exerc. 48, 1223–1224 (2016).
Rasberry, C. N. et al. The association between school-based physical activity, including physical education, and academic performance: a systematic review of the literature. Prev. Med. 52, S10–S20 (2011).
de Greeff, J. W., Bosker, R. J., Oosterlaan, J., Visscher, C. & Hartman, E. Effects of physical activity on executive functions, attention and academic performance in preadolescent children: a meta-analysis. J. Sci. Med. Sport 21, 501–507 (2018).
Xue, Y., Yang, Y. & Huang, T. Effects of chronic exercise interventions on executive function among children and adolescents: a systematic review with meta-analysis. Br. J. Sports Med. 53, 1397–1404 (2019).
Alvarez-Bueno, C. et al. The effect of physical activity interventions on children’s cognition and metacognition: a systematic review and meta-analysis. J. Am. Acad. Child Adolesc. Psychiatry 56, 729–738 (2017).
Alvarez-Bueno, C. et al. Association of physical activity with cognition, metacognition and academic performance in children and adolescents: a protocol for systematic review and meta-analysis. BMJ Open 6, e011065 (2016).
Pesce, C. et al. Deliberate play and preparation jointly benefit motor and cognitive development: mediated and moderated effects. Front. Psychol. 7, 349 (2016).
Cserjesi, R., Molnar, D., Luminet, O. & Lénárd, L. Is there any relationship between obesity and mental flexibility in children? Appetite 49, 675–678 (2007).
Li, Y., Dai, Q., Jackson, J. C. & Zhang, J. Overweight is associated with decreased cognitive functioning among school-age children and adolescents. Obesity 16, 1809–1815 (2008).
Martin, A. et al. Associations between obesity and cognition in the pre-school years. Obesity 24, 207–214 (2016).
Coppin, G., Nolan-Poupart, S., Jones-Gotman, M. & Small, D. M. Working memory and reward association learning impairments in obesity. Neuropsychologia 65, 146–155 (2014).
Brogan, A., Hevey, D., O’Callaghan, G., Yoder, R. & O’Shea, D. Impaired decision making among morbidly obese adults. J. Psychosom. Res. 70, 189–196 (2011).
Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G., PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6, e1000097 (2009).
Higgins, J. P. & Green, S. Cochrane handbook for systematic reviews of interventions version 5.1.0. Naunyn-Schmiedebergs Arch. f.ür. experimentelle Pathologie und Pharmakologie 5, S38 (2011).
Davis, C. L. et al. Effects of aerobic exercise on overweight children’s cognitive functioning: a randomized controlled trial. Res. Q. Exerc. Sport 78, 510–519 (2007).
Davis, C. L. et al. Exercise improves executive function and achievement and alters brain activation in overweight children: a randomized, controlled trial. Health Psychol. 30, 91–98 (2011).
Delgado-Rico, E. et al. Effects of a multicomponent behavioral intervention on impulsivity and cognitive deficits in adolescents with excess weight. Behav. Pharm. 23, 609–615 (2012).
Goldfield, G. S., Adamo, K. B., Rutherford, J. & Murray, M. The effects of aerobic exercise on psychosocial functioning of adolescents who are overweight or obese. J. Pediatr. Psychol. 37, 1136–1147 (2012).
Staiano, A. E., Abraham, A. A. & Calvert, S. L. Competitive versus cooperative exergame play for African American adolescents’ executive function skills: short-term effects in a long-term training intervention. Dev. Psychol. 48, 337–342 (2012).
Vanhelst, J., Beghin, L., Fardy, P. S., Bui-Xuan, G. & Mikulovic, J. A conative educational model for an intervention program in obese youth. BMC Public Health 12, 416 (2012).
Bock, D. E. et al. The Health Initiative Program for Kids (HIP Kids): effects of a 1-year multidisciplinary lifestyle intervention on adiposity and quality of life in obese children and adolescents—a longitudinal pilot intervention study. BMC Pediatr. 14, 296 (2014).
Crova, C. et al. Cognitively challenging physical activity benefits executive function in overweight children. J. Sports Sci. 32, 201–211 (2014).
Krafft, C. E. et al. Improved frontoparietal white matter integrity in overweight children is associated with attendance at an after-school exercise program. Dev. Neurosci. 36, 1–9 (2014).
Krafft, C. E. et al. An 8-month randomized controlled exercise trial alters brain activation during cognitive tasks in overweight children. Obesity 22, 232–242 (2014).
Kulendran, M. et al. Neuropsychological assessment as a predictor of weight loss in obese adolescents. Int. J. Obes. 38, 507–512 (2014).
Gallotta, M. C. et al. Impacts of coordinative training on normal weight and overweight/obese children’s attentional performance. Front. Hum. Neurosci. 9, 577 (2015).
Huang, T. et al. Effects of an obesity intervention program on cognitive function in children: a randomized controlled trial. Obesity 23, 2101–2108 (2015).
Chen, S. R., Tseng, C. L., Kuo, S. Y. & Chang, Y. K. Effects of a physical activity intervention on autonomic and executive functions in obese young adolescents: a randomized controlled trial. Health Psychol. 35, 1120–1125 (2016).
Xie, C., Wang, X., Zhou, C., Xu, C. & Chang, Y. K. Exercise and dietary program-induced weight reduction is associated with cognitive function among obese adolescents: a longitudinal study. PeerJ 5, e3286 (2017).
Augustijn, M. et al. Weight loss, behavioral change, and structural neuroplasticity in children with obesity through a multidisciplinary treatment program. Hum. Brain Mapp. 40, 137–150 (2019).
Bagherniya, M. et al. Assessment of the efficacy of physical activity level and lifestyle behavior interventions applying social cognitive theory for overweight and obese girl adolescents. J. Res. Health Sci. 18, e00409 (2018).
Carey, J. R., Bhatt, E. & Nagpal, A. Neuroplasticity promoted by task complexity. Exerc. Sport Sci. Rev. 33, 24–31 (2005).
Best, J. R. Effects of physical activity on children’s executive function: contributions of experimental research on aerobic exercise. Dev. Rev. 30, 331–551 (2010).
Mcmorris, T., Turner, A., Hale, B. J. & John, S. in Exercise-Cognition Interaction: Neuroscience Perspectives (ed. McMorris, T.) 65−103 (Elsevier Academic Press, San Diego, CA, 2016).
Theokas, C. D. S., Hodge, K., Heke, I. & Forneris, T. in Positive Youth Development Through Sport (ed. Holt, N. L.) 49−60 (Routledge, New York, NY, 2008).
Acknowledgements
The study was funded in part by the US National Institutes of Health (NIH, U54 HD070725) and by the Xi’an Jiaotong University. The U54 project (U54 HD070725) is funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) and the Office of the Director, National Institutes of Health (OD). Y.W. is the principal investigator of the study. The content of the paper is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
Author information
Authors and Affiliations
Contributions
X.S. and Y.L.: contributed to the study design, literature search, data screening and extraction, conducted all statistical analyses, and wrote the first draft of the manuscript and integration of all comments of the coauthors before submission. L.C.: contributed to the design of the study, literature search, data screening, data interpretation and critical revisions of the first draft. Y.W.: contributed to the study design, literature search, statistical analysis, and critically revised the manuscript. All authors have revised and approved the final manuscript for submission.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Search terms
Search terms
Search algorithm includes all possible combinations of keywords from the following four groups:
-
A.
“physical activity” OR “athletic participation” OR “exercise” OR “active*” OR “training” OR “sport*” OR “physical education” OR “fitness” OR “aerobic”
-
B.
“overweight” OR “obes*” OR “adiposity”
-
C.
“child*” OR “adolescen*” OR “juvenile*” OR “youth*” OR “teen*” OR “kid*” OR “student*” OR “pupil*” OR “preschool*” OR “school age*” OR “school child*”
-
D.
“academic achievement” OR “academic performance” OR “academic attainment” OR “academic skills” OR “academic ability” OR “performance at school” OR “cognit*” OR “brain”
-
E.
“intervention stud*” OR “randomized controlled” OR “longitudinal stud*”OR “cohort stud*” OR “prospective”
Rights and permissions
About this article

Cite this article
Sun, X., Li, Y., Cai, L. et al. Effects of physical activity interventions on cognitive performance of overweight or obese children and adolescents: a systematic review and meta-analysis. Pediatr Res 89, 46–53 (2021). https://doi.org/10.1038/s41390-020-0941-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-020-0941-3
This article is cited by
-
Exercise Reshapes the Brain: Molecular, Cellular, and Structural Changes Associated with Cognitive Improvements
Molecular Neurobiology (2023)
-
Effects of Exercise Training on Executive Functioning in Adults with Depression: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Sports Medicine (2023)
-
Effect of physical activity interventions on children's academic performance: a systematic review and meta-analysis
European Journal of Pediatrics (2023)
-
Effects of Movement Behaviors on Overall Health and Appetite Control: Current Evidence and Perspectives in Children and Adolescents
Current Obesity Reports (2022)
-
The Role of Chronic Physical Activity in Alleviating the Detrimental Relationship of Childhood Obesity on Brain and Cognition
Journal of Cognitive Enhancement (2022)

{kind=link}
{kind=link}