
Abstract
Background
Leukocyte telomere length (LTL), an indicator of aging, is influenced by both genetic and environmental factors; however, its heritability is unknown. We determined heritability and inheritance patterns of telomere length across three generations of families.
Methods
We analyzed 287 individuals from three generations of 41 Korean families, including newborns, parents, and grandparents. LTL (the ratio of telomere repeat copy number to single gene copy number) was measured by quantitative real-time PCR. We estimated heritability using the SOLAR software maximum-likelihood variance component methods and a pedigree dataset. With adjustment for age and length of marriage, Pearson’s partial correlation was performed for spousal pairs.
Results
Heritability of LTL was high in all participants (h2 = 0.64). There were no significant differences in correlation coefficients of telomere length between paternal and maternal lines. There was a positive LTL correlation in grandfather–grandmother pairs (r = 0.25, p = 0.03) but not in father–mother pairs. After adjusting for age and length of marriage, the relationship between telomere lengths in grandfathers and grandmothers disappeared. There were inverse correlations between spousal rank differences of telomere length and length of marriage.
Conclusions
LTL is highly heritable without a sex-specific inheritance pattern and may be influenced by a shared environment.
Similar content being viewed by others


Introduction
Telomeres are repetitive sequences of DNA (TTAGGG) located at the ends of mammalian chromosomes, which play a role in maintaining genomic stability and function.1 It has been shown that telomere length is influenced by not only the genetically determined telomere length at birth,2 but also the environmental factors such as smoking, sedentary lifestyle, and psychosocial aspects.3 Determining the heritability and inheritance patterns of telomere length could be an important cornerstone in understanding the dynamics of telomere length. In previous studies, the estimated heritability of telomere length ranged from 34% to 82% in humans.4,5,6,7,8 One study showed that the rank of an individual’s telomere length did not change over time.9 The degree to which the telomere length of offspring is influenced by genetic factors is still unknown. Inheritance patterns of telomere length also remain in question. An earlier study reported that telomere length inheritance was linked to the X chromosome.10 In addition, several studies showed paternal inheritance.11,12,13 On the contrary, stronger maternal inheritance rather than paternal inheritance was suggested in a cross-sectional study14 and a meta-analysis.5 An observational study7 and another meta-analysis15 found no significant difference between father–offspring and mother–offspring telomere length correlation degree. Most of the aforementioned studies utilized Caucasian subjects. A few studies have been conducted in Asia.16,17
Therefore, the purpose of this study was to determine the telomere length heritability and inheritance patterns across three generations of Korean families, including newborns, parents, and grandparents. Furthermore, the correlation of spousal pairs’ telomere lengths was also evaluated in order to assess the influence of environment on telomere length.
Methods
Study participants
This family-based study included 287 individuals from 41 families, each family was represented by seven members. Altogether, 26 male and 15 female newborns, their parents, and grandparents were analyzed. Healthy pregnant mothers in the third trimester were recruited through an obstetrics and gynecology hospital and a university-based childbirth clinic in Seoul between October 2012 and May 2013. A questionnaire survey, dietary interview, physical examination, and blood collection were performed. Pregnant participants were excluded if they developed pre-eclampsia, eclampsia, or gestational diabetes; a congenital anomaly such as Down syndrome was suspected in the fetus by the triple test or fetal ultrasound; or the newborn was born prematurely at <37 weeks of pregnancy. At delivery, the umbilical cord blood of the newborn was collected. Other family members, including the newborn’s father and grandparents, visited a family medicine clinic of Chung-Ang University Hospital for a medical examination and interview between October 2013 and May 2014. Written informed consent was obtained from each participant and from a parent of the newborn. The study complied with the Declaration of Helsinki and the study protocol was approved by the institutional review board of Chung-Ang University Hospital, Seoul (C2012185(880)).
Questionnaires
Length of marriage, alcohol consumption, smoking status, physical exercise, current medications, and medical history were assessed using a questionnaire. Heavy alcohol consumption was defined as ≥15 drinks per week for men and ≥8 drinks per week for women. Regular exercise was defined as physical exercise performed for a period of at least 30 min >3 times per week. Quality of life was measured using the Korean version of the 36-item short form health survey (SF-36).18 Physical and mental component summary scores from 1 (lowest) to 100 (highest) were calculated based on the 8 dimensions of the SF-36. Nutritional assessment was performed using dietary intake data obtained using a 24-h recall method. Dietary data was analyzed using CAN-pro 3.0 (Korean Nutrition Society, Korea), professional software for nutrient intake calculation. Intake of protein, fat, and carbohydrates are presented as a percentage of total energy intake.
Physical examination and biochemical assay
Body weight of the participants was measured in light clothing and no shoes except for self-reported pre-pregnancy weights. Height was measured using a stadiometer. Body mass index (BMI) was calculated as weight divided by height squared (kg/m2). Grip strength was measured using a strain-gauged dynamometer (Takeii TKK 501; Scientific Instruments Co. Ltd, Tokyo, Japan). Participants performed three trials with each hand, alternating the sides. Maximal recorded grip score was used as the grip strength.19 Biochemical tests were only performed on the blood samples of parents and grandparents after overnight fasting (>12 h). Total white blood cell (WBC) count and high-sensitivity C-reactive protein (hs-CRP) were determined using the ADVIA 120 automated hematology analyzer (Siemens, Tarrytown, NY, USA) and the ADVIA 1650 chemistry analyzer (Siemens, Tarrytown, NY, USA), respectively.
Measurement of leukocyte telomere length (LTL)
Whole-blood DNA was extracted using the G-spin Genomic DNA Extraction Kit for Blood (iNtRON Biotechnology Inc., Kyungki-Do, Korea). All DNA samples were diluted to the same concentration based on ultraviolet absorbance and stored at −80 °C until time of use. LTL was measured as the ratio of telomere repeat copy number to single gene copy number (T/S ratio) by quantitative real-time PCR, as previously described.20 Real-time PCR was performed using a Light-Cycler 2.0 (Roche Diagnostic, Mannheim, Germany) and FastStart DNA Master SYBR Green I Kit (Roche Diagnostic), with a 2 mM final MgCl2 concentration. Primers for the telomere PCR were 200 nmol/l of 5′-GGTTTTTGAGGGTGAGGGTGAGGGTGAGGGTGAGGGT-3′ and 200 nmol/l of 5′-TCCCGACTATCCCTATCCCTATCCCTATCCCTATCCCTA-3′. Primers for the A-globin PCR were 300 nmol/l of 5’-GCTTCTGACACAACTGTGTTCACTAGC-3’ and 500 nmol/l of 5’-CACCAACTTCATCCACGTTCACC-3’. The thermal cycling profile for telomere amplification was 10 min at 95 °C, followed by 25 cycles of 10 s at 95 °C and 60 s at 58 °C, and for A-globin amplification the first step was 10 min at 95°C, followed by 35 cycles of 10 s at 95 °C and 15 s at 56 °C. Each sample was run in duplicate, using 25 ng of DNA per 10 µl reaction volume. A no-template control was included in each run, and the same calibrator sample was used in all runs to allow comparison of results across runs. Melting curve analysis was performed on every run to verify the specificity and identity of the PCR products. The T/S ratio of each sample was calculated from the Ct values using the following equation: T/S = 2−ΔCt (where ΔCt = Ctsingle-copy gene − Cttelomere). The coefficients of variation of the telomere, single gene, and T/S ratio duplicate assays were <4%, <3%, and <5%, respectively.
Statistical analyses
Age and LTL T/S ratios are presented as mean ± standard deviation (SD). Since the distribution of LTL T/S ratios was skewed, LTL T/S ratio was logarithmically transformed. Telomere length variability between different generations and sexes was compared by t tests or analysis of variance.
Heritability (h2) was estimated by maximum-likelihood variance component methods implemented in the Sequential Oligogenic Linkage Analysis Routines (SOLAR) software (SOLAR Eclipse version 8.1.1; http://solar-eclipse-genetics.org/) using a pedigree dataset.21 Heritability was defined as the proportion of total phenotypic variance explained by additive genetic factors over the total genetic and environmental variance.22 Heritability (h2, 95% confidence interval (CI)) was calculated with adjustment for age, sex, age × sex, age2, and age2 × sex or with adjustment of significant covariates in the best model after removal of covariates without significance (p ≥ 0.1).
Covariates included in the screening model were age, sex, BMI, heavy alcohol consumption, smoking, regular exercise, medical history of hypertension and diabetes, and dietary intake including total energy, fat, and protein intake, grip strength as a measure of physical function, and hs-CRP and total WBC counts as inflammatory indices. The association between telomere length and covariates is presented as beta coefficient ± standard error (SE). In addition, to examine paternal or maternal heritability on offspring separately, we assumed that one parent and one grandparent were known. For example, only phenotypic information of fathers and paternal grandfathers was provided for the analysis of paternal heritability.7
To evaluate the pairwise relationships between telomere lengths, Pearson’s partial correlation coefficients were calculated with age adjustment. For multiple pairwise tests between a newborn and a parent or grandparent, p values were corrected using the Bonferroni method. The cut-off for the p value was 0.008 ( = 0.05/6).
We evaluated whether length of marriage in spousal pairs was associated with telomere length correlations between the husbands and wives. Pearson’s partial correlations with adjustments for age and length of marriage were performed in spousal pairs. Telomere length was ranked separately according to sex. Spearman’s rank-order correlation coefficients were calculated between spousal rank differences in telomere length and length of marriage (adjusted for age).
Pearson’s partial and Spearman’s rank-order correlations were performed using the SAS 9.1 statistics package (SAS Institute, Inc., Cary, NC, US). The cocor package (http://comparingcorrelations.org/) was used for comparing two correlations based on dependent groups with overlapping variables.23
Results
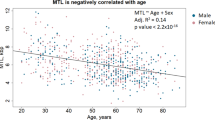
There were significant differences in the mean LTL T/S ratios of the three groups of participants (newborns: 1.65 ± 0.65, parents: 1.18 ± 0.48, and grandparents: 0.87 ± 0.32, p < 0.01). LTL T/S ratios were greater in mothers (1.34 ± 0.51) and grandmothers (0.95 ± 0.34) than in fathers (1.01 ± 0.40) and grandfathers (0.79 ± 0.29) (all p < 0.01, Fig. 1). The covariates of age × sex (p = 0.34), age2 (p = 0.33), and age2 × sex (p = 0.24) were removed from the final analytic model. LTL T/S ratios were significantly associated with age (β = −0.022 ± 0.001) and sex (β = 0.373 ± 0.088) (all p < 0.01). Age and sex-adjusted heritability of LTL T/S ratios in all family relations was 0.64 (95% CI 0.47–0.81, p < 0.01). Heritability estimates according to generation and sex are shown in Table 1. There was no difference in the heritability estimates between male (0.58, 95% CI 0.31–0.86, p < 0.01) and female newborns (0.62, 95% CI 0.35–0.89, p < 0.01) (t = 0.17, p = 0.86).

p Values were calculated by t tests or ANOVA. T/S ratio ratio of telomere repeat copy number to single gene copy number.
When we adjusted for potential confounders, significant variables included in the best model were age (β = −0.030 ± 0.003, p < 0.01), sex (β = 1.007 ± 0.156, p < 0.01), grip strength (β = 0.059 ± 0.008, p < 0.01), and dietary fat intake (β = −0.011 ± 0.003, p = 0.01) in the grandparents–parent trios. In the grandmother–parent duos, age (β = −0.027 ± 0.003, p < 0.01), grip strength (β = 0.007 ± 0.006, p < 0.01), and mental component summary score of SF-36 (β = 0.018 ± 0.006, p = 0.04) were included in the best model. In the grandfather–parent duos, age (β = −0.010 ± 0.008, p = 0.02), sex (β = 1.290 ± 0.457, p < 0.01), BMI (β = −0.029 ± 0.019, p = 0.02), grip strength (β = 0.072 ± 0.013, p < 0.01), mental component summary score of SF-36 (β = 0.005 ± 0.007, p = 0.06), dietary fat intake (β = −0.008 ± 0.007, p = 0.02), smoking status (β = −0.329 ± 0.263, p = 0.09), and hypertension (β = −0.211 ± 0.139, p = 0.01) were also included.
LTL T/S ratios of newborns were only positively associated with that of the mother (r = 0.63, p < 0.0001) (Fig. 2a). LTL T/S ratios of newborns were not correlated with paternal and maternal grandparents (Fig. 2b, c). There was a positive association between the LTL T/S ratios of grandparents and a parent (grandmother: r = 0.35, p < 0.01; grandfather r = 0.23, p = 0.04) (Fig. 2d). However, there were no significant differences in correlation coefficients of LTL T/S ratios between paternal lines and maternal lines (Table 2).

Correlations of telomere lengths between newborns and parents (a), between newborns and paternal grandparents (b), between newborns and maternal grandparents (c), between parents and grandparents (d), and between husbands and wives (e). Pearson’s partial correlation coefficients were calculated with age adjustment. For multiple tests, significant level was corrected using the Bonferroni method 0.008 ( = 0.05/6) (a–c).
Figure 2e shows the association between the LTL T/S ratios of husbands and wives by generation. After age adjustment, there was a positive association between the LTL T/S ratios of all husbands and wives (r = 0.20, p = 0.03). By generation, there was a positive association only between the LTL T/S ratios of grandfathers and grandmothers (r = 0.25, p = 0.03). After adjustment for age and marriage length, the association between the LTL T/S ratios of grandfathers and grandmothers was not significant (r = 0.20, p = 0.07). There were inverse correlations between spousal rank differences in LTL T/S ratios and marriage length after age adjustment (all ρ = −0.50, p < 0.01; grandparents ρ = −0.66, p < 0.01; parents ρ = −0.39, p < 0.01).
Discussion
This three-generation (including newborns) family-based study demonstrated a high estimated telomere length heritability of 0.64, without a sex-specific inheritance pattern. Length of marriage seemed to affect the relationship between the telomere lengths of husbands and wives.
Several studies have shown a wide range of estimated heritability and an inconsistent inheritance pattern of telomere length. Paternal inheritance of telomere length was reported among the independent duos or trios selected from 2 to 5 generation of families (12–102 years).11 Another study of 132 healthy individuals including 32–42-year-old offspring and their 52–86-year-old parents also suggested paternal inheritance of telomere length.12 Similarly, a third study also showed paternal inheritance among individuals with low bone mineral density or history of fracture, their spouse, and all first-degree relatives (age 18–92 years; mean age of 49 ± 17 years).13 The latter study reported a relatively low estimated heritability of 0.44. The other studies did not report an estimated heritability. On the contrary, a meta-analysis of six large, independent cohort studies with a total of 19,173 participants aged 15–99 years concluded a high heritability of 0.70 with a maternal inheritance pattern.5 Possible explanations for these dominant sex-specific parental effects on telomere length inheritance have been suggested.24,25
However, recently it has been revealed that heritability of telomere length between paternal lines and maternal lines are not different, which is also in line with the results of this study. A meta-analysis within a population of European descendants showed no significant differences between mother–offspring and father–offspring correlation of telomere length.15 A large study of long-lived families showed an overall heritability of 0.54 between long-lived elderly and their offspring (mean age of 61.7 years) adjusted for multiple demographic and environmental factors. Heritability of telomere length was not different between male parent to offspring and female parent to offspring groups.7 These results suggest that telomere length of newborns may be determined by genetic factors rather than by epigenetic or non-genetic (maternal environment) factors.
There is also a race/ethnic difference in the telomere length.26 In a study where the majority of mothers were White (56%) and Hispanic (29%), newborn LTL is more strongly correlated with the mother’s LTL than with the fathers’ LTL.14 In a study of Arabs, heritability between a single parent and their offspring (n = 42) was estimated at 0.64, as in our result, but offspring telomere length was more highly correlated with paternal telomere length than with maternal telomere length.16 Longer maternal telomere lengths predicted longer offspring telomere lengths in the Philippines.17 However, the heritability estimates of these studies did not take into consideration additive genetic and parental effects because the estimates were calculated using a parent–offspring regression model.14,16,17 The latter study17 did not report an association between paternal and offspring telomere lengths.
Two previous studies have shown conflicting results in telomere length correlation of spouses. One study reported no significant association between spouses aged 52–86 years.12 Another study reported a significant association between spouses that was stronger in older couples (mean age ≥55 years) than in younger couples (mean age <55 years).5 We also found a significant association between the telomere lengths of husbands and wives in their sixties, whereas the telomere lengths of young couples in their early thirties were not correlated. Overall, telomere length is more correlated between spouses with longer relationships, regardless of generation. It has also been suggested that telomere length may be influenced by environmental factors.3
To our knowledge, the current study is the first to identify the heritability and inheritance patterns of telomere length across three generations of families, including newborns. The inclusion of newborns was necessary to minimize the environmental influence for a more precise estimation of heritability and inheritance patterns of telomere length. Only a few studies of telomere length measured at childbirth showed some association between maternal or paternal and newborn telomere length.14,27,28 Our study also included the evaluation of various confounding factors affecting telomere attrition such as anthropometric measurements, grip strength, inflammatory markers, psychological factor, health behaviors, medical history, and nutritional intake.
Several limitations should also be noted. First, this study is not a population-based study but a small, ethnically homogeneous selected study that can limit the generalization of the results. Second, the relatively small sample size may limit the ability to uncover the differences between heritability estimates of different sexes or generations. Third, we could not adjust telomere length based on the WBC count because analysis of newborns’ WBC counts was not performed. Recent studies showed that telomere length is positively associated with WBC counts.29 It should also be noted that the blood samples of the parents were collected at different times. The blood of the mothers in the study was collected during pregnancy but that of the fathers was collected after the birth of a child. These factors could influence the estimation of the mother–newborn telomere length association level. Finally, we did not examine certain demographic factors, such as educational level, residential area, and occupation. Recent studies reported that toxic metals,28 residential traffic exposure,30 and maternal education level31 were associated with telomere length at birth. These demographic factors can be significant environmental components of the heritability estimate of telomere length.
In conclusion, it appears that telomere length has high heritability and does not show a sex-specific inheritance pattern. Given the differences in the telomere length variability between spousal pairs from different generations, it seems that telomere length can also be influenced by environmental factors. Further studies of East Asian populations are needed to clarify these heritability and inheritance patterns of telomere length and to further identify the factors that influence them.
References
Eisenberg, D. T. An evolutionary review of human telomere biology: the thrifty telomere hypothesis and notes on potential adaptive paternal effects. Am. J. Hum. Biol. 23, 149–167 (2011).
Armanios, M. Telomeres and age-related disease: how telomere biology informs clinical paradigms. J. Clin. Invest. 123, 996–1002 (2013).
Huda, N., Tanaka, H., Herbert, B. S., Reed, T. & Gilley, D. Shared environmental factors associated with telomere length maintenance in elderly male twins. Aging Cell 6, 709–713 (2007).
Bischoff, C. et al. The heritability of telomere length among the elderly and oldest-old. Twin Res. Hum. Genet. 8, 433–439 (2005).
Broer, L. et al. Meta-analysis of telomere length in 19,713 subjects reveals high heritability, stronger maternal inheritance and a paternal age effect. Eur. J. Hum. Genet. 21, 1163–1168 (2013).
Hjelmborg, J. B. et al. The heritability of leucocyte telomere length dynamics. J. Med. Genet. 52, 297–302 (2015).
Honig, L. S. et al. Heritability of telomere length in a study of long-lived families. Neurobiol. Aging 36, 2785–2790 (2015).
Jeanclos, E. et al. Telomere length inversely correlates with pulse pressure and is highly familial. Hypertension 36, 195–200 (2000).
Benetos, A. et al. Tracking and fixed ranking of leukocyte telomere length across the adult life course. Aging Cell 12, 615–621 (2013).
Nawrot, T. S., Staessen, J. A., Gardner, J. P. & Aviv, A. Telomere length and possible link to X chromosome. Lancet 363, 507–510 (2004).
Nordfjall, K., Svenson, U., Norrback, K. F., Adolfsson, R. & Roos, G. Large-scale parent-child comparison confirms a strong paternal influence on telomere length. Eur. J. Hum. Genet. 18, 385–389 (2010).
Nordfjall, K., Larefalk, A., Lindgren, P., Holmberg, D. & Roos, G. Telomere length and heredity: Indications of paternal inheritance. Proc. Natl Acad. Sci. USA 102, 16374–16378 (2005).
Njajou, O. T. et al. Telomere length is paternally inherited and is associated with parental lifespan. Proc. Natl Acad. Sci. USA 104, 12135–12139 (2007).
Factor-Litvak, P. et al. Leukocyte telomere length in newborns: implications for the role of telomeres in human disease. Pediatrics 137, e20153927 (2016).
Eisenberg, D. T. Inconsistent inheritance of telomere length (TL): is offspring TL more strongly correlated with maternal or paternal TL? Eur. J. Hum. Genet. 22, 8–9 (2014).
Al-Attas, O. S. et al. Circulating leukocyte telomere length is highly heritable among families of Arab descent. BMC Med. Genet. 13, 38 (2012).
Eisenberg, D. T., Hayes, M. G. & Kuzawa, C. W. Delayed paternal age of reproduction in humans is associated with longer telomeres across two generations of descendants. Proc. Natl Acad. Sci. USA 109, 10251–10256 (2012).
Han, C. W., Lee, E. J., Iwaya, T., Kataoka, H. & Kohzuki, M. Development of the Korean version of short-form 36-item health survey: Health related QOL of healthy elderly people and elderly patients in Korea. Tohoku J. Exp. Med. 203, 189–194 (2004).
Roberts, H. C. et al. A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age Ageing 40, 423–429 (2011).
Cawthon, R. M. Telomere length measurement by a novel monochrome multiplex quantitative PCR method. Nucleic Acids Res. 37, e21 (2009).
Almasy, L. & Blangero, J. Multipoint quantitative-trait linkage analysis in general pedigrees. Am. J. Hum. Genet. 62, 1198–1211 (1998).
Koran, M. E. et al. Impact of family structure and common environment on heritability estimation for neuroimaging genetics studies using Sequential Oligogenic Linkage Analysis Routines. J. Med. Imaging (Bellingham) 1, 014005 (2014).
Diedenhofen, B. & Musch, J. cocor: a comprehensive solution for the statistical comparison of correlations. PLoS ONE 10, e012194 (2015).
De Meyer, T. et al. A non-genetic, epigenetic-like mechanism of telomere length inheritance? Eur. J. Hum. Genet. 22, 10–11 (2014).
De Meyer, T. & Eisenberg, D. T. A. Possible technical and biological explanations for the ‘parental telomere length inheritance discrepancy' enigma. Eur. J. Hum. Genet. 23, 3–4 (2015).
Brown, L., Needham, B. & Ailshire, J. Telomere length among older U.S. adults: differences by race/ethnicity, gender, and age. J. Aging Health 29, 1350–1366 (2017).
Akkad, A. et al. Telomere length in small-for-gestational-age babies. BJOG 113, 318–323 (2006).
Herlin, M. et al. Exploring telomere length in mother-newborn pairs in relation to exposure to multiple toxic metals and potential modifying effects by nutritional factors. BMC Med. 17, 77 (2019).
Neuner, B. et al. Telomere length is not related to established cardiovascular risk factors but does correlate with red and white blood cell counts in a German blood donor population. PLoS ONE 10, e0139308 (2015).
Bijnens, E. et al. Lower placental telomere length may be attributed to maternal residential traffic exposure; a twin study. Environ. Int. 79, 1–7 (2015).
Wojcicki, J. M. et al. Cord blood telomere length in Latino infants: relation with maternal education and infant sex. J. Perinatol. 36, 235–241 (2016).
Acknowledgements
This work was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, Information and Communications Technology (ICT) & Future Planning (No. 2012R1A1A2041924 to J.-H.K.).
Author information
Authors and Affiliations
Contributions
This manuscript is based on the first author’s doctoral dissertation from the Graduate School of Yonsei University. J.-H. Kim was a major contributor toward acquiring the data and writing the manuscript. C.M.N. contributed to statistical analyses and revised the manuscript critically for important intellectual content. D.-C.L., J.-H. Ko, H.B., and I.L. contributed to laboratory analyses and revised the manuscript critically for important intellectual content. G.J.K. was involved with data collection and revised the manuscript critically for important intellectual content. B.W.K. revised the manuscript critically for important intellectual content. D.-C.L. was responsible for the study conception and design, as well as for intellectual content of the paper. All authors read and approved the final version of manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Kim, JH., Nam, C.M., Lee, D. et al. Heritability of telomere length across three generations of Korean families. Pediatr Res 87, 1060–1065 (2020). https://doi.org/10.1038/s41390-019-0699-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-019-0699-7
This article is cited by
-
A comparison of feature selection methodologies and learning algorithms in the development of a DNA methylation-based telomere length estimator
BMC Bioinformatics (2023)
-
Genetically determined telomere length and multiple myeloma risk and outcome
Blood Cancer Journal (2021)
-
Shortening of the leucocytes’ telomeres length in T2DM independent of age and telomerase activity
Acta Diabetologica (2020)
