
Abstract
Injuries continue to be the leading cause of morbidity and mortality for children, adolescents, and young adults aged 1–24 years in industrialized countries in the twenty-first century. In this age group, injuries cause more fatalities than all other causes combined in the United States (U.S.). Importantly, many of these injuries are preventable. Annually in the U.S. there are >9 million emergency department visits for injuries and >16,000 deaths in children and adolescents aged 0–19 years. Among injury mechanisms, motor vehicle crashes, firearm suicide, and firearm homicide remain the leading mechanisms of injury-related death. More recently, poisoning has become a rapidly rising cause of both intentional and unintentional death in teenagers and young adults aged 15–24 years. For young children aged 1–5 years, water submersion injuries are the leading cause of death. Sports and home-related injuries are important mechanisms of nonfatal injuries. Preventing injuries, which potentially cause lifelong morbidity, as well as preventing injury deaths, must be a priority. A multi-pronged approach using legislation, advancing safety technology, improving the built environment, anticipatory guidance by clinical providers, and education of caregivers will be necessary to decrease and prevent injuries in the twenty-first century.
Similar content being viewed by others


Introduction
Injuries continue to be the leading cause of death and disability in children and young adults aged 1–24 years in the United States (U.S.) and other industrialized countries.1,2 In the U.S., injuries cause more deaths in children aged 1–24 years than all other causes combined (Fig. 1).2 Injuries may not be considered a “disease” in the traditional sense of other medical conditions. Nonetheless, like many medical conditions, traumatic injuries have algorithms for diagnosis and management.3,4 Most importantly, many injuries, unlike many medical conditions, are preventable. As injuries are the leading cause of death and disability in children, adolescents, and young adults, preventing injuries must be a priority for preventing “disease” in the twenty-first century.

Top 6 leading causes of death, age 0–24 years, United States 2017.2 Data abstracted from Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System. https://webappa.cdc.gov/sasweb/ncipc/leadcause.html. Accessed 26 March 2019
The field of injury prevention employs scientific principles to identify areas for intervention and best practice. The Haddon matrix is one systematic approach for developing interventions. This approach analyzes injuries by considering how the host (i.e., individual) is injured through the force of an agent (e.g., motor vehicle, firearm, etc.) in an environment in three different phases: pre-injury, during the injury event, and post-injury.5,6 Possible types of interventions include: legislation (municipal, state, federal), use of safety equipment (e.g., helmets, seat belts), improvements to the built environment (e.g., improved infrastructure with safer roadways), and education of families about safety hazards for children.7 In this review article of the most common pediatric injuries in the U.S., we describe pediatric injury epidemiology, best practices for prevention, and future directions for research and prevention.
Epidemiology of injuries in children
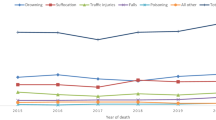
Advances in medical care have led to significant declines in death from infectious diseases and cancer in the past several decades. In contrast, injury-related deaths have been increasing in children and adolescents in the U.S. in the past decade (Fig. 2).8,9,10 Annually, there are >9 million visits to U.S. emergency departments (EDs) for injuries in children and adolescents aged 0–19 years.11 In 2017, unintentional injuries were the leading cause of death for children and youth aged 1–24 years, resulting in 16,286 fatalities.2 The cost of hospital-treated nonfatal injuries was estimated to be on average $47,000–$59,000 per injury in this age group.12 In addition to acute medical care, the costs of rehabilitation care, long-term disability care, and work-loss costs must be considered when calculating the costs for injuries. These costs do not account for the unmeasurable emotional costs to the individual and their loved ones.

Death rates for children aged 10–19 years, United States 1999–2016.10 Reproduced with permission from Curtin, S. Recent increased in injury mortality among children and adolescents aged 10–19 years in the United States: 1999–2016. (2018). https://www.cdc.gov/nchs/data/nvsr/nvsr67/nvsr67_04.pdf
Unintentional injuries
The leading causes and intents of nonfatal and fatal unintentional injury vary by age group. For unintentional nonfatal injuries, they include falls for children aged <9 years, “struck by/against” another object or person for adolescents aged 10–19 years (e.g., sports injuries), and motor vehicle crashes (MVCs) for young adults aged 20–24 years (Fig. 3). MVCs also continue to be the leading cause of unintentional fatal injury for children adolescents aged 5–19 years (Fig. 4).2 Unintentional poisoning caused the overwhelming majority of unintentional injury deaths in 2017 for young adults aged 20–24 years. Opioids and hallucinogens accounted for 50.3% of these poisoning deaths. Drowning is the leading cause of unintentional death in children aged 1–4 years. Suffocation, fires/burns, and pedestrians struck are other significant causes of death in the youngest children aged 1–4 years.2

Leading nonfatal injury mechanisms, age 0–24 years, United States 2017.2 Data abstracted from Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System. https://webappa.cdc.gov/sasweb/ncipc/leadcause.html. Accessed 26 March 2019

Leading fatal injury mechanisms, age 0–24 years, United States 2017.2 Data abstracted from Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System. https://webappa.cdc.gov/sasweb/ncipc/leadcause.html. Accessed 26 March 2019
Intentional injuries
Intentional injuries also continue to be a leading cause of death in teenagers and young adults (Fig. 4).2,13 In 2017, suicide was the second leading cause of all deaths (after unintentional injuries) in adolescents aged 10–14 years (517 deaths: 54% suffocation/hanging, 36% firearms, 7.5% poisoning) and teenagers/young adults aged 15–24 years (6252 deaths: 47% firearms, 37% suffocation/hanging, 7.4% poisoning, 3.1% falls). Homicide was the third leading cause of death for those aged 15–24 years.2
Road traffic injuries
Motor vehicle crashes
Annually in the U.S., there are >9000 deaths and >2,000,000 injuries from MVCs in children and youth aged 0–24 years. MVCs are the leading fatal injury mechanism in youth aged 1–24 years, causing 7814 deaths in 2017.2 Teenage drivers are at increased risk for MVC injuries and deaths.14 Major contributing factors to MVC injuries and deaths include vehicle speed, alcohol impairment, and distracted driving. Of these factors, speed in a MVC is possibly the most significant factor, not only for the severity of a crash but also the risk of crash. Studies have demonstrated reduced speed, by either road modification or law enforcement, can significantly reduce MVC injuries.15,16,17 Overall, alcohol-impaired driving has declined, but there remains a significant risk for child passengers of impaired drivers.18 Distracted driving has emerged as one of the most significant factors in MVC injuries for teenagers. A recent survey reported that half of U.S. high school students aged ≥16 years reported texting while driving during the past 30 days, and they were more likely to engage in additional risky motor vehicle behaviors.19
Significant improvements in vehicle safety features, the use of child safety restraint seats (CSRSs) and booster seats, and safety legislation and enforcement have resulted in decreasing injuries and deaths from MVCs in the past several decades.20,21,22,23 Vehicle design and mandated safety features (e.g., frontal airbags mandated in passenger cars in 1998) have saved >44,000 lives from 1987 to 2015.24 Legislation has influenced increasing use of CSRSs and booster seats, resulting in decreased MVC deaths.25 Since 1975, there has been a 71% reduction in MVC fatalities for infants and a 54% reduction for children aged 1–4 years.20 For children aged 4–7 years, the use of belt-positioning booster seats reduces injury risk by 45% compared to seat belt use alone.21,25,26 The most stringent Graduated Driver Licensing programs, placing restrictions on novice adolescent drivers aged <18 years, are associated with reductions of 38% and 40% in fatal and non-fatal crashes, respectively, among 16-year-old drivers.14,27
Bicycle/pedestrian vs. vehicle injuries
Although there have been modest improvements in pedestrian and bicycle vs. motor vehicle injuries in the past decade, these mechanisms remain uniquely important for the pediatric population.24 In 2017, fatal injuries occurred to 679 bicyclists and 6480 pedestrians, and nonfatal injuries occurred to 329,831 bicyclists and 193,866 pedestrians aged 0–24 years.2 Recent studies have shown reductions in pedestrian vs. motor vehicle injuries by: (1) reducing vehicle speeds; (2) physically separating pedestrians from vehicles (e.g., crossing cycle timing where all traffic stops to allow pedestrians to cross in any direction); and (3) increasing pedestrian visibility, especially in parking areas, which can be associated with significant risk for children.28 These changes to the built environment, defined as the human-made space in which people live, work, and recreate daily, are especially important for improving safety for children.29
Reduction in bicyclist vs. motor vehicle injuries have historically involved promoting helmet wearing and changes to the built environment to improve rider safety. Helmets decrease facial and head injuries for bicyclists, and state legislation requiring bicycle helmets for children has been associated with significant reductions in fatalities.30,31,32 Changes to the built environment, including intersection design and street width, with physically separated bicycling lanes, also mitigate the level of severity of a bicycle vs. motor vehicle injury.33,34
Strategies for preventing motor vehicle injuries in the twenty-first century
In 2018, the American Academy of Pediatrics (AAP) updated its best practice recommendations to set the standard for child passenger safety for U.S. children aged 0–13 years. They stated children should be secured in: (1) rear-facing CSRSs as long as possible; (2) forward-facing car safety seats through age at least 4 years for most children; (3) belt-positioning booster seats from the time they outgrow forward-facing seats through age at least 8 years; and (4) lap and shoulder seat belts for all who have outgrown booster seats.35 In addition, a fifth evidence-based recommendation is for children aged <13 years to ride in the vehicle rear seats.23 Owing to variations in state laws, there is no uniform enactment or enforcement of these recommendations,22,25 which if implemented and enforced in the future, would likely have a significant impact on reducing morbidity and mortality for children involved in MVCs.
Ongoing modifications to the built environment and promoting motor vehicle safety legislation to address emerging threats (e.g., autonomous vehicles, impaired driving from marijuana) will be important in preventing fatal and nonfatal injuries from MVCs, as well as pedestrian/bicyclists vs. motor vehicle collisions.36 Although legislative efforts such as texting bans have been effective in some studies, further research on legislation and technology-assisted mechanisms for reducing distracted driving are clearly needed.37 Standardization of state child passenger safety laws will make future research on their efficacy easier to interpret and policy directions clearer.22,35 For bicyclists and pedestrians, research and implementation of interventions to improve the built environment, paired with legislative efforts to require bicycle helmet use,38 will be necessary to decrease these injuries.39
Firearm injuries
In the U.S., 87 people are killed by firearms daily, equating to one firearm fatality every 17 min.40 Approximately 1300 youth aged 0–17 years die from firearms annually.41 From 1999 to 2017, >27,000 youth aged 0–17 years were killed by firearms.2 Globally, 90% of firearm deaths to children aged <15 years occur in the U.S.42 Youth firearm homicide is 36 times more likely to occur in the U.S. compared to other high-income countries.43 From 2013 to 2016 in the U.S., there was a 28% increase in firearm deaths for children aged 1–19 years, with firearm homicide increasing by 32% and firearm suicide increasing by 28%.9
The intent of firearm death varies by age group (Fig. 5). Firearm suicide is the third leading cause of death in youth aged 10–14, 15–19, and 20–24 years.2 Unintentional firearm injuries and deaths among children aged <5 years have also been increasing, with fatality rates doubling in this age group between 2006 and 2016.2 Although there has been increased attention to firearm violence in the context of multiple mass shootings, the majority of firearm deaths in children are not from mass shootings.44

Firearm deaths by intent, age 0–24 years, United States 2017.2 Data abstracted from Centers for Disease Control and Prevention. Web-based Injury Statistics Query and Reporting System. https://webappa.cdc.gov/sasweb/ncipc/leadcause.html. Accessed 26 March 2019
In addition to fatalities, >20,000 children are treated in EDs, and 7000 children are hospitalized annually from firearm injuries in the U.S.2,45 Most firearm deaths in children occur in the home.46 They often occur when children are playing with guns and less often when firearms are mistaken for toys or dropped unintentionally.41,47 This is important to understand as an estimated 22 million U.S. children live in households where firearms are kept.48
Strategies for preventing firearm injuries in the twenty-first century
Firearm-related injuries and deaths are a public health crisis,49 and strategies for preventing these injuries are essential. Legislation is one strategy, and there are >300 U.S. federal laws regulating the sales, possession, and various aspects of the handling and storage of firearms. Individual state laws allow for significant variation in the implementation of these federal laws.50 In general, stronger firearm laws are associated with decreased firearm deaths.51,52 Reviews of firearm legislation have concluded that legislation associated with decreased firearm fatalities include universal background checks prior to the purchase of firearms and ammunition as well as permits to purchase firearms.51,52,53
Some states have enacted child access protection (CAP) laws legislating safe firearm storage practices for firearm owners with children. These laws hold owners criminally liable for children’s unsupervised use of firearms and have been shown to improve firearm storage behaviors.54 They are associated with decreased youth firearm injury and death only in states with stringent penalties when a child accesses a firearm.55,56,57 CAP laws have also been associated with reduced youth suicide rates.58
In addition to legislation, another important strategy to consider for the twenty-first century is the development of “smart gun technology,” consisting of firearms that can only be operated by an authorized user. This user can be identified through fingerprints or through the use of a device (e.g., watch) that, when worn, enables the firearm to be discharged.59 Though implicitly promising, the effect of smart gun technology on firearm-related injuries and deaths has yet to be studied. One study of 117 unintentional firearm-related deaths estimated that as many as 37% of these deaths could have been prevented with the use of smart gun technology.60
Counseling on firearms during primary care provider visits is another important strategy to potentially reduce firearm-related injuries among children. Pediatricians are trained in providing anticipatory guidance for a variety of health behaviors, and the AAP recommends providers address firearm injury prevention.7,61,62 Counseling parents on firearm safety has been demonstrated to increase safe firearm storage.63 Nonetheless, most physicians do not routinely counsel patients on firearm safety.64,65 Although the majority of surveyed parents believe physicians should ask about firearms in the home, they are infrequently asked.64,65,66 Future studies focusing on the barriers and facilitators of firearm injury prevention counseling for patients and families will be important to improve counseling and decrease firearm injuries to children.
Drowning (water submersion) injuries
Drowning is the leading cause of injury death in young children aged 0–4 years,2 resulting in approximately 2–3 deaths daily. More children aged 1–4 years die from drowning than any other cause except congenital anomalies.67 The incidence peaks in children aged 0–4 years and adolescents aged 15–19 years, with highest rates in the summer and on weekends.68 The primary location of drownings vary by age: bathtub or bucket for infants, swimming pools for young children, and natural bodies of water (e.g., lake, ocean) for adolescents.68,69
Males drown (2.0/100,000 persons) at higher rates than females (0.8/100,000 persons).67 Other demographic risk factors for drowning include younger age, epilepsy, low income, poor education, and living in a rural location.68,69,70,71,72 Racial disparities exist among drowning victims with drowning rates twice as high in American Indian/Alaskan Native children and 1.4 times as high in black children compared to white children.71
Pediatric providers must recognize the public health burden of drowning and include water safety and drowning prevention in their routine anticipatory guidance.68,69 It is estimated 85% of drownings could be prevented with adequate supervision, public education, and swimming instruction.68,70,73 Supervision is best performed by a vigilant caregiver using “touch supervision” when he/she is within arm’s reach of the child in a body of water (e.g., swimming pool).69
Strategies for preventing drowning injuries in the twenty-first century
For pediatric drowning prevention the AAP recommends: (1) enhanced adult supervision when children are in or near water (including bathtubs, pools, lakes); (2) installation of four-sided pool fences; (3) swimming and water safety lessons for adults and children; (4) parental knowledge of cardiopulmonary resuscitation; (5) personal floatation device (PFD) use on watercraft; and (6) supporting legislation for pool fences and PFD use.69 A four-sided, self-closing, and self-latching pool fence is the most studied and effective prevention strategy to prevent young children from unintentionally accessing a swimming pool and drowning.69,74 Legislation for pool fence use and inspection with enforcement is effective in decreasing pediatric drownings.69,74,75 Basic swimming and water safety lessons decrease drowning death,76,77 but parents must also understand swimming lessons cannot “drown proof” a child or replace supervision.
Home-related injuries
For the youngest children, age <5 years, the majority of unintentional injuries occur in the home.78 An important mechanism of injury-related death for infants is sudden unexplained infant death, which includes sudden infant death syndrome, accidental suffocation and strangulation in bed, and sudden unexpected postnatal collapse.79 In children aged 1–5 years, the leading causes of home-related injuries are falls (e.g., off furniture, down stairs),80,81,82 thermal injuries (e.g., burns, scalds), poisoning and foreign body ingestion, and submersion/drowning.78,83 Thermal injuries include fire-related burns and hot water scalds from overly heated bath water or hot liquids (e.g., tea, coffee).84,85 Button batteries and magnets are other potential home hazards.86,87 Children in families of lower socio-economic status are at higher risk for home injuries.83,88 In addition, one study found children in high-income families (>$100,000 annual income) were also associated with a higher number of hazards in the home compared to middle income ($30,000–< $100,000 annual) families.83
Strategies for preventing home-related injuries in the twenty-first century
Safety equipment and home safety intervention programs can be effective in decreasing home-related injuries (Table 1).78,89,90,91 These programs educate parents and caregivers who may not always be aware of potential injury hazards to children in the home or the safety equipment is available to prevent these injuries. Home safety programs are most commonly provided as face-to-face education programs in the home, often with the provision of home safety equipment.78 The cost of safety equipment or the inability to modify one’s home (e.g., rental home) are barriers to equipment use.88 A Cochrane review including 54 studies (812,715 individuals) concluded that home-based prevention programs decreased home injury rates compared to those not participating in these programs. The Cochrane review reported home safety interventions were effective for: (1) increasing homes with safe water temperature; (2) having a working smoke alarm; (3) having a fire escape plan; (4) having a fitted stair gate; and (5) having socket covers over unused electrical sockets.78 Ultimately, a multi-faceted approach is needed to prevent home injuries to young children. In addition to home safety programs, legislation is another important strategy. Legislation has been effective in decreasing window falls when mandating window guards on a structure with a second floor or higher.92 The 2014 U.S. Consumer Product Safety Commission regulatory ban of magnet set sales effectively decreased magnet ingestions among young children. In 2016, this ban was partially repealed; thus ongoing prevention efforts must continue.86,87 Anticipatory guidance for families about home hazards, the importance of supervision, and the effectiveness of safety is also important to decrease home-related injuries.7,88
Poisoning injuries
Poisonings are the sixth leading cause of death in children of all ages9 and the second leading cause of unintentional death in those aged 15–24 years.2 In those aged 15–24 years, poisonings are also the third leading cause of suicide, accounting for 463 deaths in 2017.2 Medication overdoses have exceeded household products as the leading culprit.93 The U.S. legislative landscape has been changing regarding opioid prescribing and substances like cannabis. State legislation in 2019 allows legalized cannabis use in 34 states.94 This has indirectly affected pediatric patients and demands a shift in our prevention efforts.94,95 Between 2006 and 2013, pediatric cannabis exposure rose 148% overall and 610% in states allowing medical cannabis.96,97 Additionally, opioid toxicity in children aged ≤5 years is now responsible for more hospitalizations annually than any other oral prescription drug.98
Unintentional ingestions are common, sending 1 out of every 150 2-year-old children to the ED annually.93,99 Owing to high availability, single ingredient, pediatric liquid products (e.g., acetaminophen, diphenhydramine) continue to be associated with high rates of these ingestions, despite prevention efforts.98,100 Household products (e.g., bleach, detergents) also continue to cause unintentional ingestions.99 After the introduction of laundry detergent pod packs, detergent ingestions increased 50% in 2013 compared to 2012, and they are now a focus of injury prevention efforts.101,102,103
In addition to continued pediatric poisonings from household products and pediatric over the counter (OTC) medications, the opioid epidemic has added complexity. Pediatric opioid ingestions have risen dramatically, with a nearly twofold increase in hospitalizations between 1997 and 2012 and a nearly threefold increase in mortality between 1999 and 2016.95,104,105 Approximately 60% of ingestions occur in children aged ≤5 years; however, adolescents represent a higher number of intentional ingestions and experience higher morbidity and mortality. The highest rates of pediatric opioid exposure occur in homes with non-Hispanic whites, older adults, and a higher proportion of adults. Methadone and buprenorphine overdoses have become prevalent as opioid-dependence programs have expanded.104
The Poison Prevention Packaging Act of 1970, mandating child-resistant packaging (CRP), resulted in significant declines in pediatric poisoning deaths.106 Despite these results, ED visits and calls to poison control centers continue to increase in children.99,101 Recognizing the limitations of CRP (i.e., reliance on caregivers to completely/correctly replace the cap each time) and the continued burden of pediatric poisoning, the CDC created a public-private initiative, Preventing Overdoses and Treatment Exposures Task Force (PROTECT) in 2008. PROTECT has focused on improving drug packaging, medication error prevention, and public education through the creation of the “Up and Away” campaign to educate caregivers to store medications safely.93
Strategies for preventing poisoning in the twenty-first century
Innovative packaging techniques, such as flow-restrictors (i.e., adaptors limiting the flow of liquid medication out of the bottle) and unit-dose packaging (UDP), have demonstrated promise in poisoning prevention. UDP limits access to large doses of hazardous tablet/capsule medications by packaging each dose separately. Flow-restrictors added to OTC acetaminophen suspension bottles in 2011 have limited the volume of medication toddlers can ingest.93,107 Buprenorphine–naloxone film, packaged in UDP since 2010, has resulted in lower exposure rates compared to other combination opioid formulations.108 Since 2013, UDP packing is used for 80% of combination buprenorphine products.108
A renewed sense of urgency to prevent poisonings in children has gained response from the Food and Drug Administration, CDC, and the National Academy of Medicine.109 While flow-restrictors, UDP, and other packaging techniques have been successful in reducing poisonings, these strategies deter access but do not eliminate it. Continued expansion of abuse-deterrent opioid formulations, new non-opioid options for pain, and wide-spread dispersion of reversal agents are imperative.109 In addition, as suicide is increasing in all age groups,2 there is a dire need for expansion of pediatric mental health services and provider anticipatory guidance during well-child visits to include discussion of means restriction of medications to prevent intentional overdoses. Policy-makers, clinicians, and public health advocates must refocus educational efforts, continue innovation in drug packaging, and respond to the opioid crisis, with a lens focused on decreasing poisoning injuries in children.
Sports injuries
Nearly 47 million children in the U.S. play team sports annually.110,111 While the benefits of sports participation have been well documented,112,113 participation is not without risk. An estimated 5.6 million sports-related injuries occur yearly among those aged 5–24 years, with rates varying by sport (Fig. 6).114,115,116,117 This includes 3.2 million injuries in children aged 5–14 years, the age group with the highest rate (77/100,000 persons).114 Sports injuries are responsible for 1.35 million ED visits (nearly 20% of all injury-related visits) annually and are one of the leading cause of ED visits for children aged 12–17 years.2,118 The most common injuries include: strains/sprains (40.3%), contusions (9.2%), fractures (8.9%), and concussions (24.4%).115 Overuse injuries account for nearly 50% of sports injuries and may be rising due to increases in sport specialization.119,120 Catastrophic injuries resulting in death or permanent disability are rare [18 deaths in 2016–2017 (0.023/100,000 participants)].121 Driven by concern over the long-term risk of chronic traumatic encephalopathy, concussion has drawn significant research and media attention,122 leading to increases in ED visits for sports-related concussion.115,118

Rates of high school sports-related injuries by sport and setting. Adapted with data from: Comstock, R. D., Currie, D. W. & Peirpoint, L. A. National High School Sports-Related Injury Surveillance Study: 2016–2017 School Year.115
Strategies for preventing sports injuries in the twenty-first century
Important components to decrease youth sports injuries include player, parent, and coach education123,124; changes in sport-specific techniques125; and access to certified athletic trainers.126 In addition, protective equipment for the athletes, including helmets/head protection, eye protection, and mouth guards, reduce sports injuries. In football, helmets have reduced the risk of skull fractures, intracranial hemorrhages, and head injury-associated fatalities.127 While no helmet can prevent concussion/brain injury,128 recent data suggest newer helmet technology has the potential to reduce the risk.129,130 Other examples of equipment-preventing injuries include: eye protection for ocular injuries in lacrosse,131 ice hockey,132 and field hockey133,134; headgear for auricular hematomas in wrestling135; mouth guards for dental trauma in multiple sports136; and helmets for head injuries in skiing/snowboarding.137
Perhaps the greatest impact on reducing sports injuries has been rule changes, which have decreased injuries in multiple sports.138,139,140 In football, rules penalizing hitting with the head are associated with decreased quadriplegic spine injuries.141 Rules implemented in football, including moving the location of kickoffs and limiting player full-contact practice time, have shown potential in reducing concussions.140,142 In youth, ice hockey high-sticking rules, increased penalties for illegal hits, and eliminating checking have also reduced injuries.132,143 In baseball, limiting the number of pitches thrown by youth has decreased the subsequent risk of elbow surgery.144
The future of preventing sports injuries will need to focus on prospective data collection, empiric studies of interventions/equipment, and a central body to oversee this work. Accurate, prospectively collected data at all levels of participation are needed to inform and evaluate injury prevention strategies.115,145 While clustered, randomized control trials should remain the gold standard,146 researchers can leverage natural experiments to assess the effectiveness of interventions.140,143 Finally, a multi-disciplinary, central body for reviewing sports injuries, including the evaluation of prevention strategies, and analyzing data are needed.145 It is vital that sports injury prevention be data driven, as even the most well-intentioned interventions can have potentially unforeseen consequences.147
Conclusions
Advances in injury prevention over the past several decades have resulted in decreased rates of fatal and nonfatal pediatric injuries in the U.S. Effective motor vehicle safety regulations and legislation, improvements in the built environment, enhanced safety equipment for the individual (e.g., helmets), and the environment (e.g., pool fences, child resistant packaging) all working in conjunction have been critical for successful injury prevention. Despite these advances, injuries continue to be the leading cause of death and disability for those aged 0–24 years in the U.S, now with increasing deaths from opioid overdoses, MVCs, and firearms2,8,9,10
To be successful in preventing pediatric injuries in the twenty-first century, a multi-pronged approach will be necessary to address current as well as future threats, including autonomous vehicles36 and the changing landscape of legal and illegal substance use.95,97 For motor vehicles, this includes legislation and technological advances to address distracted driving. Stronger legislation for universal background checks, permits to purchase firearms, child access prevention, and preventing firearm possession by those at risk for harming themselves or others must be considered more broadly to decrease firearm injuries.50,51,52,53,58 For preventing poisoning, effective packaging to decrease the unit dose ingested as well as strategies to combat the increasing opioid epidemic will be necessary.95,107,108,109 Promoting the use of safety equipment to prevent drowning, home-related, and sports injuries are important for decreasing these injuries. For all mechanisms of injury, pediatric providers can provide important and effective anticipatory guidance to families about injury prevention.7,66,148
Critical to advancing pediatric injury prevention in the twenty-first century is the conduct of high-quality research in the effectiveness of interventions, including for firearm injuries. Despite extant evidence for effective legislation reducing firearm injuries and deaths, the Dickey amendment, a U.S. federal law, prohibited CDC funding to be used to promote gun control. This was reinterpreted in a 2018 Congressional spending bill stating the CDC can fund gun violence research; however, gun violence research funding is still limited.149 In addition to gun violence research, supporting funding for future research evaluating the effectiveness of safety equipment and programs to promote their use will be required to decrease intentional and unintentional injuries.
Injuries are associated with high costs to individuals and to society in the forms of acute medical care, rehabilitative care, work-loss costs, and years of potential life lost,12 which does not account for the unmeasurable emotional costs to their families and loved ones. Effective interventions must be implemented and studied to decrease injuries in children, teenagers, and young adults. As injuries continue to be the leading cause of death and disability to our children, preventing injuries must be a priority for the twenty-first century.
References
Sleet, D. A. The global challenge of child injury prevention. Int. J. Environ. Res. Public Health 15, E1921 (2018).
Centers for Disease Control and Prevention. Web-based injury statistics query and reporting system https://webappa.cdc.gov/sasweb/ncipc/leadcause.html (2019).
Holmes, J. F. et al. Identifying children at very low risk of clinically important blunt abdominal injuries. Ann. Emerg. Med. 62, 107–116.e2 (2013).
Kuppermann, N. et al. Identification of children at very low risk of clinically-important brain injuries after head trauma: a prospective cohort study. Lancet 374, 1160–1170 (2009).
Haddon, W. A logical framework for categorizing highway safety phenomena and activity. J. Trauma 12, 193–207 (1972).
Runyan, C. W. Using the haddon matrix: introducing the third dimension. Inj. Prev. 21, 126–130 (2015).
The American Academy of Pediatrics. TIPP–The Injury Prevention Program https://patiented.solutions.aap.org/handout-collection.aspx?categoryid=32033 (2019).
Lee, L. K. & Mannix, R. Increasing fatality rates from preventable deaths in teenagers and young adults. JAMA [Internet] 02115, 1–2 (2018).
Cunningham, R. M., Walton, M. A. & Carter, P. M. The major causes of death in children and adolescents in the United States. N. Engl. J. Med. 379, 2468–2475 (2018).
Curtin, S. Recent increases in injury mortality among children and adolescents aged 10–19 years in the United States: 1999–2016 https://www.cdc.gov/nchs/data/nvsr/nvsr67/nvsr67_04.pdf (2018).
Borse, N. et al. CDC Childhood Injury Report: patterns of unintentional inuries among 0-19 year olds in the United States, 2000-2006 https://www.cdc.gov/safechild/child_injury_data.html (2008).
Zonfrillo, M. R., Spicer, R. S., Lawrence, B. A. & Miller, T. R. Incidence and costs of injuries to children and adults in the United States. Inj. Epidemiol. 5, 4–9 (2018).
Xu, J., Murphy, S. L., Kochanek, K. D., Bastian, B. & Arias. E. Deaths: final data for 2016. Natl. Vital Stat. Rep. 67, 1–76 (2018)
Alderman, E. M. & Johnston, B. D. The teen driver. Pediatrics 142, e20182163 (2018).
Aarts, L. & Van Schagen, I. Driving speed and the risk of road crashes: a review. Accid. Anal. Prev. 38, 215–224 (2006).
Ewing, R. & Dumbaugh, E. The built environment and traffic safety: a review of empirical evidence. J. Plan. Lit. 23, 347–367 (2009).
Staton, C. et al. Road traffic injury prevention initiatives: a systematic review and metasummary of effectiveness in low and middle income countries. PLoS ONE 11, e0144971 (2016).
Quinlan, K., Shults, R. A. & Rudd, R. A. Child passenger deaths involving alcohol-impaired drivers. Pediatrics 133, 9966–9972 (2014).
Olsen, E. O., Shults, R. A. & Eaton, D. K. Texting while driving and other risky motor vehicle behaviors among US high school students. Pediatrics 131, e1708–e1715 (2013).
Kahane, C. J. Lives saved by vehicle safety technologies and associated Federal Motor Vehicle Safety Standards, 1960 to 2012 - passenger cars and LTVs https://crashstats.nhtsa.dot.gov/Api/Public/ViewPublication/812069 (2015).
Arbogast, K. B., Jermakian, J. S., Kallan, M. J. & Durbin, D. R. Effectiveness of belt positioning booster seats: an updated assessment. Pediatrics 124, 1281–1286 (2009).
Bae, J. Y., Anderson, E., Silver, D. & Macinko, J. Child passenger safety laws in the United States, 1978-2010: policy diffusion in the absences of strong federal intervention. Soc. Sci. Med. 100, 30–37 (2014).
Durbin, D. R. & Committee on Injury, Violence and Poison Prevention. Technical Report–child passenger. safety. Pediatrics 27, e1050–e1066 (2011).
U.S. Department of Transportation National Highway Safety Transportation Administration. Road Safety, 2018 https://www.nhtsa.gov/road-safety (2019).
Mannix, R. et al. Booster seat laws and fatalities in children 4 to 7 years of age. Pediatrics 130, 996–1002 (2012).
Sauber-Schatz, E. K., West, Ba & Bergen, G. Vital signs: restraint use and motor vehicle occupant death rates among children aged 0-12 years - United States, 2002-2011. MMWR Morb. Mortal. Wkly. Rep. 63, 113–118 (2014).
Baker, S. P., Chen, L.-H. & Li, G. Nationwide review of Graduated Driver Licensing https://aaafoundation.org/nationwide-review-graduated-driver-licensing/ (2007).
Retting, R. A., Ferguson, S. A. & McCartt, A. T. A review of evidence-based traffic engineering measures designed to reduce pedestrian-motor vehicle crashes. Am. J. Public Health 93, 1456–1463 (2003).
To, T., Rothman, L., Buliung, R., Macarthur, C. & Howard, A. Motor vehicle-pedestrian collisions and walking to school: the role of the built environment. Pediatrics 133, 776–784 (2014).
Bambach, M. R., Mitchell, R. J., Grzebieta, R. H. & Olivier, J. The effectiveness of helmets in bicycle collisions with motor vehicles: a case-control study. Accid. Anal. Prev. 53, 78–88 (2013).
Meehan, W. P., Lee, L. K., Fischer, C. M. & Mannix, R. C. Bicycle helmet laws are associated with a lower fatality rate from bicycle-motor vehicle collisions. J. Pediatr. 163, 726–729 (2013).
Thompson, D. C., Rivara, F. & Thompson, R. Helmets for preventing head and facial injuries in bicyclists. Cochrane Database Syst. Rev. CD001855 (2000)
Asgarzadeh, M., Verma, S., Mekary, R. A., Courtney, T. K. & Christiani, D. C. The role of intersection and street design on severity of bicycle-motor vehicle crashes. Inj. Prev. 23, 179–185 (2017).
Chen, P. & Shen, Q. Built environment effects on cyclist injury severity in automobile-involved bicycle crashes. Accid. Anal. Prev. 86, 239–246 (2016).
Durbin, D. R., Hoffman, B. D. & Council on Injury, Violence and Poison Prevention. Child passenger safety: policy statement. Pediatrics 142, e20182461 (2018).
Favarò, F. M., Nader, N., Eurich, S. O., Tripp, M. & Varadaraju, N. Examining accident reports involving autonomous vehicles in California. PLoS ONE 12, 1–20 (2017).
Ferdinand, A. O. et al. The impact of texting bans on motor vehicle crash-related hospitalizations. Am. J. Public Health 105, 859–865 (2015).
Macpherson, A. & Spinks, A. Bicycle helmet legislation for the uptake of helmet use and prevention of head injuries. Cochrane Database Syst. Rev. CD005401 (2008).
Embree, T. E. et al. Risk factors for bicycling injuries in children and adolescents: a systematic review. Pediatrics 138, e20160282 (2016).
NBC News. Just the facts: gun violence in America http://usnews.nbcnews.com/_news/2013/01/16/16547690-just-the-facts-gun-violence-in-america?lite (2013).
Fowler, K. A., Dahlberg, L. L., Haileyesus, T., Gutierrez, C. & Bacon, S. Childhood firearm injuries in the United States. Pediatrics 140, 1–11 (2017).
Grinshteyn, E. & Hemenway, D. Violent death rates: the US compared with other high-income OECD countries, 2010. Am. J. Med. 129, 266–273 (2016).
Richardson, E. G. & Hemenway, D. Homicide, suicide, and unintentional firearm fatality: comparing the United States with other high-income countries, 2003. J. Trauma Inj. Infect. Crit. Care 70, 238–243 (2011).
Gun Violence Archive. Mass shootings http://www.gunviolencearchive.org/mass-shooting (2019).
Leventhal, J. M., Gaither, J. R. & Sege, R. Hospitalizations due to firearm injuries in children and adolescents. Pediatrics 133, 219–225 (2014).
Centers for Disease Control and Prevention. National Violent Death Reporting System https://www.cdc.gov/violenceprevention/nvdrs/index.html (2019).
Barber, C. & Hemenway, D. Too many or too few unintentional firearm deaths in official U.S. mortality data? Accid. Anal. Prev. 43, 724–731 (2011).
Azrael, D., Cohen, J., Salhi, C. & Miller, M. Firearm storage in gun-owning households with children: results of a 2015 National Survey. J. Urban Heal 95, 295–304 (2018).
Winker, M., Abbasi, K. & Rivara, F. P. Unsafe and understudied: the US gun problem. BMJ 10, i578 (2016).
Safavi, A. et al. Children are safer in states with strict firearm laws: a National Inpatient Sample Study. J. Trauma Acute Care Surg. 76, 146–150 (2014). Discussion 150–151.
Santaella-Tenorio, Julian, Cerda, Magdalena, Vellaveces, Andres & Galea, S. What do we know about the assocation between firearm legislation and firearm-related injuries? Epidemiol. Rev. 38, 140–157 (2016).
Fleegler, E. W., Lee, L. K., Monuteaux, M. C., Hemenway, D. & Mannix, R. Firearm legislation and firearm-related fatalities in the United States. JAMA Intern. Med. 173, 732–740 (2013).
Lee, L. K. et al. Firearm laws and firearm homicides. JAMA Intern. Med. 02115, 1–14 (2016).
Prickett, K., Martin-Storey, A. & Crosnoe, R. State firearm laws, firearm ownership, and safety practices among families of preschool-aged children. Am. J. Public Health 104, 1080–1086 (2014).
Hahn, R. et al. Firearms laws and the reduction of violence: a systematic review. Am. J. Prev. Med. 28, 40–71 (2005).
Hepburn, L., Azrael, D., Miller, M. & Hemenway, D. The effect of child access prevention laws on unintentional child firearm fatalities, 1979-2000. J. Trauma 61, 423–428 (2006).
Webster, D. & Starnes, M. Reexamining the association between child access prevention gun laws and unintentional shooting deaths of children. Pediatrics 106, 1466–1469 (2000).
Webster, D., Vernick, J., Zeoli, A. & Manganello, J. Association between youth-focused firearm laws and youth suicides. JAMA 292, 594–601 (2004).
Simonetti, J., Rowhani-Rahbar, A. & FP, R. The road ahead for personalized firearms. JAMA Intern. Med. 177, 9–10 (2017).
Vernick, J. S. et al. Unintentional and undetermined firearm related deaths: a preventable death analysis for three safety devices. Inj. Prev. 9, 307–311 (2003)
Crossen, E. J., Lewis, B. & Hoffman, B. D. Preventing gun injuries in children. Pediatr. Rev. 36, 43–51 (2015).
American Academy of Pediatrics Council on Injury, Violence and Poison Prevention. Firearm-related injuries affecting the pediatric population. Pediatrics 130, e1416–e1423 (2012).
Barkin, S. L. et al. Is office-based counseling about media use, timeouts, and firearm storage effective? Results from a cluster-randomized, controlled trial. Pediatrics 122, e15–e25 (2008).
Butkus, R. & Weissman, A. Internists’ attitudes toward prevention of firearm injury. Ann. Intern. Med. 160, 821–827 (2014).
Solomon, B. S., Duggan, A. K., Webster, D. & Serwint, J. R. Pediatric residents’ attitudes and behaviors related to counseling adolescents and their parents about firearm safety. Arch. Pediatr. Adolesc. Med. 156, 769–775 (2002).
Garbutt, J. M., Bobenhouse, N., Dodd, S., Sterkel, R. & Strunk, R. C. What are parents willing to discuss with their pediatrician about firearm safety? A parental survey. J. Pediatr. 179, 166–171 (2016).
Centers for Disease Control and Prevention (CDC). Centers for Disease Control: Child Safety and Injury Prevention, Drowning (2019).
Conover, K. & Romero, S. Drowning prevention in pediatrics. Pediatr. Ann. 47, e112–e117 (2018).
Denny, S. A. et al. Prevention of drowning. Pediatrics 143, e20190850 (2019).
Szpilman, D., Joost, J., Bierens, M., Handley, A. & Orlowski, J. P. Drowning. N. Engl. J. Med 366, 2109–2110 (2012).
Gilchrist, J. & Parker, E. M. Centers for Disease Control and Prevention (CDC). Racial/ethnic disparities in fatal unintentional drowning among persons aged ≤29 years - United States, 1999-2010. MMWR Morb. Mortal. Wkly. Rep. 63, 421–426 (2014).
Franklin, R. C., Pearn, J. H. & Peden, A. E. Drowning fatalities in childhood: the role of pre-existing medical conditions. Arch. Dis. Child. 102, 888–893 (2017).
Quan, L., Bennett, E. E. & Branche, C. M. in Handbook of Injury and Violence Prevention (eds Doll, L., Hass, E., Bonzo, S., Sleet, D. & Mercy, J.) 81–96 (Springer US, New York City, 2007).
Thompson, D. C. & Rivara, F. P. Pool fencing for preventing drowning in children. Cochrane Database Syst. Rev. CD001047 (1998).
van Weerdenburg, K., Mitchell, R. & Wallner, F. Backyard swimming pool safety inspections: a comparison of management approaches and compliance levels in three local government areas in NSW. Health Promot. J. Aust. 17, 37–42 (2018).
World Health Organization. Global report on drowning: preventing a leading killer http://apps.who.int/iris/bitstream/10665/143893/1/9789241564786_eng.pdf?ua=1&ua=1%0Ahttp://www.who.int/violence_injury_prevention/global_report_drowning/en/ (2014).
Brenner, R. A. et al. Association between swimming lessons and drowning in childhood: a case-control study. Arch. Pediatr. Adolesc. Med. 163, 203–210 (2009).
Kendrick, D. et al. Home safety education and provision of safety equipment for injury prevention. Cochrane Database Syst. Rev. CD005014 (2012)
Bass, J. L., Gartley, T., Lyczkowski, D. A. & Kleinman, R. Trends in the incidence of sudden unexpected infant death in the newborn: 1995-2014. J. Pediatr. 196, 104–108 (2018).
Young, B., Wynn, P. M., He, Z. & Kendrick, D. Preventing childhood falls within the home: overview of systematic reviews and a systematic review of primary studies. Accid. Anal. Prev. 60, 158–171 (2013).
Kendrick, D. et al. Risk and protective factors for falls on stairs in young children: multicentre case-control study. Arch. Dis. Child. 101, 909–916 (2016).
Kendrick, D. et al. Risk and protective factors for falls from furniture in young children multicenter case-control study. JAMA Pediatr. 169, 145–153 (2015).
Mayes, S., Roberts, M. C. & Stough, C. O. Risk for household safety hazards: socioeconomic and sociodemographic factors. J. Saf. Res. 51, 87–92 (2014).
Miller, P. et al. Preventing childhood scalds within the home: overview of systematic reviews and a systematic review of primary studies. Burns 41, 907–924 (2015).
Shields, W. C., McDonald, E. M., Pfisterer, K. & Gielen, A. C. Scald burns in children under 3 years: an analysis of NEISS narratives to inform a scald burn prevention program. Inj. Prev. 21, 296–300 (2015).
Reeves, P. T., Nylund, C. M., Krishnamurthy, J., Noel, R. A. & Abbas, M. I. Trends of magnet ingestion in children, an ironic attraction. J. Pediatr. Gastroenterol. Nutr. 66, e116–e121 (2018).
Bolton, S. M., Saker, M. & Bass, L. M. Button battery and magnet ingestions in the pediatric patient. Curr. Opin. Pediatr. 30, 653–659 (2018).
Smithson, J., Garside, R. & Pearson, M. Barriers to, and facilitators of, the prevention of unintentional injury in children in the home: a systematic review and synthesis of qualitative research. Inj. Prev. 17, 119–126 (2011).
Phelan, K. J. et al. A randomized controlled trial of home injury hazard reduction: the HOME Injury Study. Arch. Pediatr. Adolesc. Med. 165, 339–345 (2011).
Ingram, J. C. et al. Identifying facilitators and barriers for home injury prevention interventions for pre-school children: a systematic review of the quantitative literature. Health Educ. Res. 27, 258–268 (2012).
Falcone, R. A. et al. Volunteer driven home safety intervention results in significant reduction in pediatric injuries: a model for community based injury reduction. J. Pediatr. Surg. 51, 1162–1169 (2015).
Toprani, A., Robinson, M., Middleton Iii, J. K., Hamade, A. & Merrill, T. New York City’s window guard policy: four decades of success. Inj. Prev. 24(Suppl 1), i14–i18 (2018).
Budnitz, D. S. & Salis, S. Preventing medication overdoses in young children: an opportunity for harm elimination. Pediatrics 127, e1597–e1599 (2011).
National Conference of State Legislatures. State Medical Marijuana Laws http://www.ncsl.org/research/health/state-medical-marijuana-laws.aspx (2019).
Gaither, J. R., Shabanova, V. & Leventhal, J. M. US national trends in pediatric deaths from prescription and illicit opioids, 1999-2016. JAMA Netw. Open 1, e186558 (2018).
Boadu, O., Gombolay, G. Y., Caviness, V. S. & El Saleeby, C. M. Intoxication from accidental marijuana ingestion in pediatric patients. Pediatr. Emerg. Care 00, 1 (2018).
Richards, J. R., Smith, N. E. & Moulin, A. K. Unintentional cannabis ingestion in children: a systematic review. J. Pediatr. 190, 142–152 (2017).
Lovegrove, M. C. et al. Emergency hospitalizations for unsupervised prescription medication ingestions by young children. Pediatrics 134, e1009–e1016 (2014).
Gummin, D. D. et al. 2016 Annual Report of the American Association of Poison Control Centers’ National Poison Data System (NPDS): 34th Annual Report. Clin. Toxicol. 55, 1072–1252 (2017).
Green, J. L. et al. Safety profile of cough and cold medication use in pediatrics. Pediatrics 139, e20163070 (2017).
Lee, V. R., Connolly, M. & Calello, D. P. Pediatric poisoning by ingestion: developmental overview and synopsis of national trends. Pediatr. Ann. 46, e443–e448 (2017).
Yin, S., Colvin, J. & Behrman, A. Single-use laundry detergent pack exposures in children under 6 years: a prospective study at U.S. Poison Control Centers. J. Emerg. Med. 55, 354–365 (2018)
Swain, T. A., McGwin, G. & Griffin, R. Laundry pod and non-pod detergent related emergency department visits occurring in children in the USA. Inj. Prev. 22, 396–399 (2016).
Patel, A. M. et al. Prevalence and characteristics of pediatric opioid exposures and poisonings in the United States. J. Pediatr. 206, 148–155.e4 (2019).
Gaither, J. R., Leventhal, J. M., Ryan, S. A. & Camenga, D. R. National trends in hospitalizations for opioid poisonings among children and adolescents, 1997 to 2012. JAMA Pediatr. 170, 1195 (2016).
Rodgers, G. B. Safety effects of child-resistant packaging for oral prescription drugs two decades of experience. JAMA 275, 1661–1665 (1996).
Lovegrove, M. C. et al. Efficacy of flow restrictors in limiting access of liquid medications by young children. J. Pediatr. 163, 1134–1139.e1 (2013).
Wang, G. S., Severtson, S. G., Bau, G. E., Dart, R. C. & Green, J. L. Unit-dose packaging and unintentional buprenorphine-naloxone exposures. Pediatrics 141, e20174232 (2018).
Califf, R. M., Woodcock, J. & Ostroff, S. A proactive response to prescription opioid abuse. N. Engl. J. Med. 374, 1480–1485 (2016).
Aspen Institute. State of play 2018: trends and developments. https://assets.aspeninstitute.org/content/uploads/2018/10/StateofPlay2018_v4WEB_2-FINAL.pdf?_ga=2.157367802.113701632.1555172075-1194653383.1555172075 (2018).
National Federation of High School Associations. 2017-18 High School Athletics Participation Survey (National Federation of High School Associations, Indianapolis, IN, 2018).
Beets, M. W. & Pitetti, K. H. Contribution of physical education and sport to health-related fitness in high school students. J. Sch. Health 75, 25–30 (2005).
Zahl, T., Steinsbekk, S. & Wichstrøm, L. Physical activity, sedentary behavior, and symptoms of major depression in middle childhood. Pediatrics 139, e20161711 (2017).
Sheu, Y., Chen, L.-H. & Hedegaard, H. Sports- and recreation-related injury episodes in the United States, 2011-2014. Natl. Health Stat. Report 1–12 (2016).
Comstock, D. R., Currie, D. W. & Pierpoint, L. A. National High School Sports-Related Injury Surveillance Study: 2015-2016 School Year (Aurora, CO, 2017).
O’Connor, K. L. et al. Epidemiology of sport-related concussions in high school athletes: National Athletic Treatment, Injury and Outcomes Network (NATION), 2011–2012 through 2013–2014. J. Athl. Train. 52, 175–185 (2017).
Zuckerman, S. L. et al. Epidemiology of sports-related concussion in NCAA athletes from 2009-2010 to 2013-2014: incidence, recurrence, and mechanisms. Am. J. Sports Med. 43, 2654–2662 (2015).
Safe Kids Worldwide. Game Changers: Stats, Stories and What Communities Are Doing to Protect Young Athletes (Safe Kids Worldwide, Washington, D.C., 2013).
Post, E. G. et al. The association of sport specialization and training volume with injury history in youth athletes. Am. J. Sports Med. 45, 1405–1412 (2017).
Valovich McLeod, T. C. et al. National Athletic Trainers’ Association position statement: prevention of pediatric overuse injuries. J. Athl. Train. 46, 206–220 (2011).
Yau, R. K., Kucera, K. L., Thomas, L. C., Price, H. M. & Cantu, R. C. Catastrophic Sports Injury Research: Fall 1982–Spring 2017 Report (National Center for Catastrophic Sports Injury Research, Chapel Hill, NC, 2018).
Mannix, R., Meehan, W. P. & Pascual-Leone, A. Sports-related concussions-media, science and policy. Nat. Rev. Neurol. 12, 486–490 (2016).
Rivara, F. P. et al. The effect of coach education on reporting of concussions among high school athletes after passage of a concussion law. Am. J. Sports Med. 42, 1197–1203 (2014).
Chrisman, S. P., Schiff, M. A., Chung, S. K., Herring, S. A. & Rivara, F. P. Implementation of concussion legislation and extent of concussion education for athletes, parents, and coaches in Washington State. Am. J. Sports Med. 42, 1190–1196 (2014).
Tokish, J. M. et al. Heads up football training decreases concusson rates in high school football players (Abstract). Orthop J. Sports Med. 5, 2325967117S00131 (2017).
McGuine, T. A. et al. The influence of athletic trainers on the incidence and management of concussions in high school athletes. J. Athl. Train. 53, 1017–1024 (2018).
Cantu, R. C. & Mueller, F. O. Brain injury-related fatalities in American football, 1945-1999. Neurosurgery 52, 846–852 (2003). Discussion 852–853.
Daneshvar, D. H., Nowinski, C. J., McKee, A. C. & Cantu, R. C. The epidemiology of sport-related concussion. Clin. Sports Med. 30, 1–17 (2011).
Collins, M., Lovell, M. R., Iverson, G. L., Ide, T. & Maroon, J. Examining concussion rates and return to play in high school football players wearing newer helmet technology: a three-year prospective cohort study. Neurosurgery 58, 275–286 (2006). discussion275-86.
Rowson, S. et al. Can helmet design reduce the risk of concussion in football? J. Neurosurg. 120, 919–922 (2014).
Lincoln, A. E. et al. Effectiveness of the women’s lacrosse protective eyewear mandate in the reduction of eye injuries. Am. J. Sports Med. 40, 611–614 (2012).
Biasca, N., Wirth, S. & Tegner, Y. The avoidability of head and neck injuries in ice hockey: an historical review. Br. J. Sports Med. 36, 410–427 (2002).
Kriz, P. K. et al. Eye protection and risk of eye injuries in high school field hockey. Pediatrics 136, 521–527 (2015).
Kriz, P. K. et al. Effectiveness of protective eyewear in reducing eye injuries among high school field hockey players. Pediatrics 130, 1069–1075 (2012).
Schuller, D. E., Dankle, S. K., Martin, M. & Strauss, R. H. Auricular injury and the use of headgear in wrestlers. Arch. Otolaryngol. Head. Neck Surg. 115, 714–717 (1989).
Knapik, J. J. et al. Mouthguards in sport activities: history, physical properties and injury prevention effectiveness. Sports Med. 37, 117–144 (2007).
Sulheim, S., Holme, I., Ekeland, A. & Bahr, R. Helmet use and risk of head injuries in alpine skiers and snowboarders. JAMA 295, 919–924 (2006).
Nichols, E. H. & Richardson, F. L. Football injuries of the Harvard squad for three years under the revised rules. 1909. Clin. Orthop. Relat. Res. 3–10 (2003).
Kriz, P. K. et al. Effect of penalty minute rule change on injuries and game disqualification penalties in high school ice hockey. Am. J. Sports Med. 47, 438–443 (2019).
Wiebe, D. J., D’Alonzo, B. A., Harris, R., Putukian, M. & Campbell-McGovern, C. Association between the experimental kickoff rule and concussion rates in Ivy League Football. JAMA 320, 2035–2036 (2018).
Rihn, J. A. et al. Cervical spine injuries in American football. Sports Med. 39, 697–708 (2009).
Broglio, S. P., Williams, R. M., O’Connor, K. L. & Goldstick, J. Football players’ head-impact exposure after limiting of full-contact practices. J. Athl. Train. 51, 511–518 (2016).
Trofa, D. P. et al. The impact of body checking on youth ice hockey injuries. Orthop. J. Sport Med. 5, 2325967117741647 (2017).
Erickson, B. J., Chalmers, P. N., Axe, M. J. & Romeo, A. A. Exceeding pitch count recommendations in Little League Baseball increases the chance of requiring Tommy John surgery as a professional baseball pitcher. Orthop. J. Sport Med. 5, 2325967117695085 (2017).
Herriman, M., Schweitzer, M. E. & Volpp, K. G. The need for an intervention to prevent sports injuries: beyond “rub some dirt on it.”. JAMA Pediatr. 173, 215–216 (2019).
Olsen, O.-E., Myklebust, G., Engebretsen, L., Holme, I. & Bahr, R. Exercises to prevent lower limb injuries in youth sports: cluster randomised controlled trial. BMJ 330, 449 (2005).
Westermann, R. W., Kerr, Z. Y., Wehr, P. & Amendola, A. Increasing lower extremity injury rates across the 2009-2010 to 2014-2015 seasons of National Collegiate Athletic Association Football: an unintended consequence of the “targeting” rule used to prevent concussions? Am. J. Sports Med. 44, 3230–3236 (2016).
Chen, J., Kresnow, M.-j, Simon, T. R. & Dellinger, A. Injury-prevention counseling and behavior among US children: results from the second injury control and risk survey. Pediatrics 119, e958–e965 (2007).
Jamison, P. The federal government isn’t funding gun-violence research. Should the District? Washington Post https://www.washingtonpost.com/local/dc-politics/the-federal-government-isnt-funding-gun-violence-research-should-the-district/2019/02/06/8453b93c-2a40-11e9-b011-d8500644dc98_story.html?utm_term=.790ddb28be1c (2019).
Author information
Authors and Affiliations
Consortia
Contributions
K.D., C.A.F., T.W.L. and L.K.L. made substantial contributions to the conception and design. All authors made substantial contributions to acquisition of data, drafting of the articles, and revising it critically for important intellectual content. All authors approved the final version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dorney, K., Dodington, J.M., Rees, C.A. et al. Preventing injuries must be a priority to prevent disease in the twenty-first century. Pediatr Res 87, 282–292 (2020). https://doi.org/10.1038/s41390-019-0549-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-019-0549-7
This article is cited by
-
Children’s injury database: development of an injury surveillance system in a pediatric emergency department
Injury Epidemiology (2023)
-
Comparison of the stair safety awareness in different target groups by applying the VASMA-C methodology
Archives of Civil and Mechanical Engineering (2022)
-
All is not well
Indian Pediatrics (2020)
