
Abstract
Vaccine-preventable infections (VPIs) are a common and serious complication following transplantation. One in six pediatric solid organ transplant recipients is hospitalized with a VPI in the first 5 years following transplant and these hospitalizations result in significant morbidity, mortality, graft injury, and cost. Immunizations are a minimally invasive, cost-effective approach to reducing the incidence of VPIs. Despite published recommendations for transplant candidates to receive all age-appropriate immunizations, under-immunization remains a significant problem, with the majority of transplant recipients not up-to-date on age-appropriate immunizations at the time of transplant. This is extremely concerning as the rate for non-medical vaccine exemptions in the United States (US) is increasing, decreasing the reliability of herd immunity to protect patients undergoing transplant from VPIs. There is an urgent need to better understand barriers to vaccinating this population of high-risk children and to develop effective interventions to overcome these barriers and improve immunization rates. Strengthened national policies requiring complete age-appropriate immunization for non-emergent transplant candidates, along with improved multi-disciplinary immunization practices and tools to facilitate and ensure complete immunization delivery to this high-risk population, are needed to ensure that we do everything possible to prevent infectious complications in pediatric transplant recipients.
Similar content being viewed by others

Introduction
Pediatric solid organ transplantation has transformed the survival rate and quality of life for patients with organ dysfunction and failure. In the past 30 years, >53,000 children have benefited from solid organ transplantation.1 Advancements in organ procurement procedures, surgical techniques, anesthetics, postoperative management, and refined immunosuppression protocols have drastically improved short-term survival; >90% of pediatric solid organ transplant recipients are alive 1-year posttransplant. There is now an increasing shift in focus on reducing morbidity from life-long immunosuppressive medications and optimizing long-term survival.
Infectious complications remain a major source of morbidity and mortality for all transplant recipients regardless of organ graft type.2,3,4 Pediatric transplant recipients are at heightened risk for infections compared to adult recipients, including vaccine-preventable infections (VPIs), as children may lack previous immunity from natural exposure and may not have had time to finish their primary immunization series by the time of transplant.5,6,7 This article provides an overview on the incidence and impact of VPIs in the pediatric solid organ transplant population and proposes policies and tools to improve immunization rates, decrease VPIs, and improve long-term outcomes in this high-risk pediatric population.
Incidence of VPIs in pediatric solid organ transplant recipients
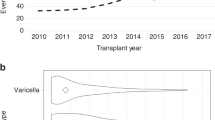
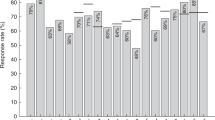
VPIs (including influenza, pneumococcus, meningococcus, Haemophilus influenzae type B, human papillomavirus, varicella, pertussis, rotavirus, measles, mumps, Hepatitis A, and Hepatitis B) are a common occurrence after pediatric solid organ transplantation.8,9,10,11,12,13,14,15,16,17 In a recent study of nearly 7000 pediatric solid organ transplant recipients from 45 tertiary care centers across the United States, 1092 (15.6%) were hospitalized with a VPI in the first 5 years posttransplant.18 The most common VPIs were influenza (40% of cases), rotavirus (19% of cases), varicella (11% of cases), pneumococcus (10% of cases), and respiratory syncytial virus (RSV) (10% of cases). The rates of hospitalization for these infections in the first year posttransplant were much greater than the expected annual rates of hospitalization in the general pediatric population (influenza 3.0% of the transplant population vs 0.06% of the general pediatric population, rotavirus 2.6% of the transplant population vs 0.03% of the general pediatric population, pneumococcus 1% of the transplant population vs 0.5% of the general pediatric population, and RSV 1.8% of the transplant population vs 0.3% of the general pediatric population). These statistics do not include those transplant recipients who had a VPI that was managed in the outpatient setting, which presumably would also occur at higher rates in pediatric transplant recipients compared to healthy children.
Morbidity, mortality, and costs from VPIs in pediatric solid organ transplant recipients
VPIs result in significant morbidity, morbidity, graft injury and hospitalization costs after transplant.8,9,10,11,12,13,14,15,16,17,19 In Feldman et al.’s study of >7000 children who received a solid organ transplant between 2004–2011, the overall case fatality rate for VPIs was 1.7%.18 The case fatality rate for each individual VPI was significantly higher in the transplant population than in the general pediatric population. Pediatric transplant patients compared to the generic pediatric population had 53 times greater mortality rate from RSV, 17 times greater mortality rate from pneumococcus, 23 times greater mortality rate from rotavirus, and 4 times greater mortality rate from influenza. Excluding infections that occurred during the initial transplant hospitalization during which every child would be intubated for the transplant surgery and then return to the intensive care unit (ICU) postoperatively, 8% of children with a VPI required mechanical ventilation and 17% required ICU-level care. Transplant hospitalizations complicated by a VPI were on average $120,000 more expensive and 39 days longer than transplant hospitalizations not complicated by a VPI.
VPIs can also result in vaccine-preventable cancers, which have associated morbidity, mortality, and costs. In a cohort study of >187,000 transplant recipients, 890 human papillomavirus-related cancers were observed.11 Compared to the general population, transplant recipients had a 3–20-fold increased risk for vaginal, anal, vulvar, and penile in situ cancers and a 2–7-fold increased risk for invasive cancers.
Increasing rates of vaccine hesitancy, non-medical vaccine exemptions, and VPIs across the United States
Immunization is one of the most cost-effective ways of avoiding disease. It has been estimated that vaccination prevents approximately 42,000 early deaths and 20 million cases of disease, with net savings of $13.5 billion in direct costs and $68.8 billion in total societal costs, respectively.20 Despite the proven benefits of vaccination,21,22,23,24,25 vaccine hesitancy (the reluctance or refusal to vaccinate despite the availability of vaccines) continues to threaten progress made in tackling VPIs. According to data from the 2017 National Immunization Survey, the percentage of children <24 months of age who had received no vaccines at all had risen to 1.3%, up from 0.3% in the 2001 survey.26 A study recently published by Olive et al. found an increase since 2009 in “philosophical-belief” non-medical vaccine exemptions in 12 of the 18 states that allow “philosophical-belief” exemptions and describe hot spots of significantly lower vaccine rates in certain large urban and also rural areas.27 Likewise, for the third year in a row the Center for Diseases Control and Prevention observed a rising rate of exemptions from school vaccination among children entering kindergarten.28 The number of children who receive some vaccines but refuse or delay others is much higher than these statistics indicate.
Importantly, because under-immunization and vaccine refusal tend to cluster geographically,27,29,30 vaccination rates in some areas may fall well below levels needed to maintain “herd immunity” for individual diseases, resulting in outbreaks.21,29,31 “Herd immunity” describes a concept where immunization of a significant portion of the population provides some degree of protection for those members of society who have not or cannot develop immunity (for example, people with allergies to vaccines, children who are too young to receive vaccines, or immunocompromised people who either cannot receive certain vaccines (such as live vaccines) or who cannot mount an immune response to vaccines). Vaccine refusal has been associated with outbreaks of multiple infections that are potentially vaccine-preventable including Haemophilus influenzae type b,32 varicella,25 pneumococcus,24 pertussis,33,34 and measles.34,35 World Health Organization data shows a rise in the number of cases of measles in almost every region of the world, with 30% more cases in 2017 than in 2016. In 2018, there were >370 confirmed measles cases in the US, which is the second largest number since measles was eliminated in the US in 200036; in just the first 4 months of 2019, this number has already been exceeded. The recent outbreaks of measles in Washington, Minnesota, and New York exemplify what happens when the vaccine rate is lower than required for herd immunity in geographic centers.
Under-immunization of solid organ transplant candidates
As is the case with the general population, immunizations are a minimally invasive, cost-effective, and safe approach to reducing the incidence of VPIs in children who are transplant candidates. Although immunizations will likely not prevent every case of VPI in the immunosuppressed transplant recipient, they can help decrease the incidence and severity of VPIs in this population. The Infectious Diseases Society of America (IDSA) and the American Society of Transplantation (AST) recommend that “solid organ transplant candidates receive all age-appropriate vaccines based on the Centers for Disease Control (CDC’s) annual schedule for immunocompetent persons.”37,38 The North American Society for Gastroenterology, Hepatology and Nutrition (NASPGHAN), The American Association for the Study of Liver Diseases (AASLD), and the AST recommend in their joint practice guideline on evaluation of the pediatric patient for transplant that “completion of all age-appropriate vaccinations should occur prior to transplantation and ideally before the development of end-stage liver disease; and that children who have not completed the necessary vaccine schedule can receive vaccinations on an accelerated schedule.”39 It is crucial for immunizations to be maximized pretransplant as (1) vaccines are more immunogenic before immunosuppressive therapies are initiated posttransplant, (2) administration of vaccines pretransplant increases the immunogenicity of vaccines posttransplant, and (3) live vaccines are currently not recommended for the majority of transplant recipients due to the risk of causing vaccine-strain disease in an immunocompromised host.40,41
Despite these recommendations, and in spite of the fact that children with organ failure receive constant medical surveillance given their acutely ill status, the majority of transplant recipients are not up-to-date on age-appropriate immunizations at the time of transplant. In a recent study of >300 pediatric liver transplant recipients from 34 North American centers, only 29% of children were completely up-to-date for age-appropriate immunizations using the CDC’s standard immunization schedule and only 19% were up-to-date using the accelerated immunization schedule for transplant candidates.42 Under-immunization was a universal problem across all liver transplant recipients and was not associated with specific demographic or clinical factors. Live vaccines were particularly under-utilized among children aged 6–11 months, suggesting that practitioners may not be aware of the ability to accelerate live vaccines before a year of age in transplant candidates.
Ethics of immunization in the solid organ transplant population—can and should we require that all pediatric transplant candidates be fully immunized before receiving an organ?
Currently, the decision about whether to offer transplantation to a child who is under-immunized is left to the discretion of each individual transplant center. In a survey of 73 North American pediatric hepatologists, 19% stated that their program lacked any written protocols regarding pretransplant and posttransplant immunization policies.43 In a separate survey of 114 medical directors, surgical directors, and transplant coordinators from 138 pediatric heart, kidney, and liver transplant programs in the United States (US), 39% of respondents reported that their program had encountered listing decisions involving a child whose parents or caregivers refused vaccination; however, only 4% reported that their program had a written policy regarding parental vaccine refusal before transplant.44 When given a hypothetical scenario about whether they would list such a child who was not fully vaccinated due to parental refusal, 47% of respondents stated that they would still list the child for transplant.
Given the growing mismatch between the number of people in need of an organ and the number of organs available, resulting in 20 deaths on the transplant waiting list each day,45 one must ask whether the United Network of Organ Sharing should institute a national policy requiring complete age-appropriate immunization for non-emergent transplants, rather than leaving this decision to individual centers. Such a policy would prevent a patient/family from “center shopping” to find a transplant center that does not require immunizations.
Additionally, institution of a national policy regarding immunization for non-emergent transplant candidates would uphold several important ethical goals including beneficence, utilitarianism, and justice.46 According to the principle of beneficence, there is a moral obligation to maximize well-being and minimize possible harms for an individual patient.47 Vaccines are potentially lifesaving for immunocompromised patients and should be treated as such.46 All transplant recipients receive immunosuppressive medications to prevent graft rejection and therefore are at increased susceptibility for infection. Although vaccines cannot prevent all infectious complications, they decrease the probability of getting VPIs that are known to cause encephalitis, meningitis, pneumonitis, allograft rejection, and death after transplant.18,19,48 According to the principle of utilitarianism, there is an obligation to consider the best ultimate outcome for society as a whole. With vaccines, this is where the concept of “herd immunity” or “community immunity” becomes important. Immunization not only directly protects the individual vaccinee by reducing the chance of infection and possible complications but also indirectly benefits society by lowering the probability that non-immune members of society will come into contact with an infectious person and lowering the probability that the disease will circulate.49,50 Finally, according to the principle of justice there should be fair, equitable, and appropriate distribution of scarce resources. Despite advances in technology and efforts to increase organ donation awareness, there are more people in need of organs than there are organs available. If an under-immunized child loses a graft or dies posttransplant secondary to an infection that was potentially vaccine-preventable, the loss of that organ harms not only that child but every person who died on the waiting list because no organ was available.
A call to action for the pediatric community
The barriers to vaccinating pediatric transplant candidates have not been well studied, but similar to vaccination in the general population they are complex and will require a multi-pronged solution. In addition to consideration of stricter policies requiring immunizations for non-emergent transplant candidates, the pediatric community must come together to develop new multi-disciplinary practice guidelines to improve immunization rates for transplant candidates who are jointly cared for by primary care providers and subspecialists so that children do not fall through the cracks. These policies must establish that the standard of care is that all patients should be as up-to-date as possible on standard vaccines by the time of transplant. The guidelines should also provide guidance to centers on catch-up vaccination in under-immunized patients who are being evaluated for transplant, acceleration of live-virus vaccines before transplant, and circumstances under which live vaccines should be reconsidered posttransplant. Transplant centers need strong national policies to guide and support their local center policies on vaccines.
In addition to standard barriers to immunization faced by healthy children (parental concern about vaccine side effects, safety, and pain; lack of access to health care; lack of insurance coverage; and moral or religious objections),51,52,53,54,55 transplant candidates face unique transplant-specific immunization barriers. These include divided care between multiple care providers, acute medical problems that may overshadow preventative care, inaccurate provider knowledge about vaccinating patients in the pretransplant period, and division of the medical home between the primary care provider and subspecialist.56 In addition, some providers are still concerned about immunizations causing graft rejection,57 although this has been disproven by multiple studies.58,59 Transplant centers may also face center-specific unique barriers and thus will need the resources (time, expertise, financial) to identify and understand their own barriers.
To overcome these barriers, novel tools are necessary to (1) educate subspecialists, primary care providers, and allied health professionals about transplant-specific immunization guidelines, (2) provide data about vaccine safety and efficacy in the transplant population to help address and overcome potential vaccine fear or hesitancy, (3) improve communication among patients and their families and a medical team that consists of multiple care providers and (4) help create automated vaccine reminders.
Health information technology (IT) solutions have been demonstrated to facilitate patient–provider communication, increase adherence to medical regimens, and improve outcomes in chronic illnesses.60,61 Digital health tools on multiple technology platforms (mobile phone, electronic medical record, and web-based) have shown to be effective for immunization-specific needs, including but not limited to creation of population-based immunization registries,62,63,64,65 implementing vaccine reminder/recall systems,66,67,68,69,70,71 providing education about vaccines for parents and providers,72 providing automated clinical decision support or “practice alerts,”73,74,75,76 reducing missed vaccine opportunities, and increasing immunization rates.53,54,72,77,78 Future cloud-based tools could be developed that are specifically tailored to the needs of the transplant population to provide (1) education about vaccine safety, efficacy, and use pretransplant and posttransplant, (2) communication portals to facilitate sharing of information between patients and multiple providers, (3) a centrally located, easily accessible vaccine record, and (4) automated vaccine reminders triggered from the accelerated schedule to assist with logistics of vaccine timing. In a recent qualitative study of 53 pediatric liver stakeholders, 94% believed that a health IT tool would be useful in increasing pretransplant immunization rates.56
Conclusions
Immunizations are one of the most important public health interventions in history and are responsible for decreasing childhood morbidity and mortality from VPIs worldwide. Each year, we invest $1.2 billion dollars in pediatric solid organ transplants79; however, we fail to protect our investment and the lives and health of our patients by not ensuring that these immunosuppressed children are fully immunized. Unfortunately, the transplant population is not the only high-risk population of children who remain under-immunized, as under-immunization is also reported in children with lupus,80,81,82,83 inflammatory bowel disease,84,85,86,87 and rheumatoid arthritis.88 As a pediatric community, we must come together to strengthen transplant immunization policies and utilize health IT tools to facilitate immunization delivery in a high-risk population that is jointly cared for by primary care providers and multiple subspecialists.
References
2019 Organ Procurement and Transplantation Network (OPTN)- National Data, Transplants in the US by Recipient Age. https://optn.transplant.hrsa.gov/data/view-data-reports/national-data/#.
Colvin, M. et al. OPTN/SRTR 2017 Annual Data Report: heart. Am. J. Transplant. 19(Suppl 2), 323–403 (2019).
Hart, A. et al. OPTN/SRTR 2017 Annual Data Report: kidney. Am. J. Transplant. 19(Suppl 2), 19–123 (2019).
Kim, W. R. et al. OPTN/SRTR 2017 Annual Data Report: liver. Am. J. Transplant. 19(Suppl 2), 184–283 (2019).
Fonseca-Aten, M. & Michaels, M. G. Infections in pediatric solid organ transplant recipients. Semin. Pediatr. Surg. 15, 153–161 (2006).
Burroughs, M. & Moscona, A. Immunization of pediatric solid organ transplant candidates and recipients. Clin. Infect. Dis. 30, 857–869 (2000).
Verma, A. & Wade, J. J. Immunization issues before and after solid organ transplantation in children. Pediatr. Transplant. 10, 536–548 (2006).
Fishman, J. A. Infection in solid-organ transplant recipients. N. Engl. J. Med. 357, 2601–2614 (2007).
Kumar, D. et al. Invasive pneumococcal disease in solid organ transplant recipients-10-year prospective population surveillance. Am. J. Transplant. 7, 1209–1214 (2007).
Apalsch, A. M., Green, M., Ledesma-Medina, J., Nour, B. & Wald, E. R. Parainfluenza and influenza virus infections in pediatric organ transplant recipients. Clin. Infect. Dis. 20, 394–399 (1995).
Madeleine, M. M., Finch, J. L., Lynch, C. F., Goodman, M. T. & Engels, E. A. HPV-related cancers after solid organ transplantation in the United States. Am. J. Transplant. 13, 3202–3209 (2013).
Olarte, L., et al. 2017 Invasive pneumococcal infections in children following transplantation in the pneumococcal conjugate vaccine era. Transpl. Infect. Dis. https://doi.org/10.1111/tid.12630 (2017).
Tran, L. et al. Invasive pneumococcal disease in pediatric organ transplant recipients: a high-risk population. Pedia. Transplant. 9, 183–186 (2005).
Kumar, D. et al. Outcomes from pandemic influenza A H1N1 infection in recipients of solid-organ transplants: a multicentre cohort study. Lancet Infect. Dis. 10, 521–526 (2010).
Fitts, S. W. et al. Clinical features of nosocomial rotavirus infection in pediatric liver transplant recipients. Clin. Transplant. 9, 201–204 (1995).
McGregor, R. S., Zitelli, B. J., Urbach, A. H., Malatack, J. J. & Gartner, J. C. Jr. Varicella in pediatric orthotopic liver transplant recipients. Pediatrics 83, 256–261 (1989).
Liu, Y. et al. Measles virus infection in pediatric liver transplantation recipients. Transplant. Proc. 47, 2715–2718 (2015).
Feldman A. G., Beaty, B. L., Curtis, D., Juarez-Colunga, E. & Kempe, A. Incidence of hospitalization for vaccine-preventable infections in children following solid organ transplant and associated morbidity, mortality, and costs. JAMA Pediatr. 173, 260–268 (2019). https://doi.org/10.1001/jamapediatrics.2018.4954.
Feldman, A. G., Sundaram, S. S., Beaty, B. L. & Kempe, A. Hospitalizations for respiratory syncytial virus and vaccine-preventable infections in the first 2 years after pediatric liver transplant. J. Pediatr. 182, 232–238 e231 (2017).
Zhou, F. et al. Economic evaluation of the routine childhood immunization program in the United States, 2009. Pediatrics 133, 577–585 (2014).
Feikin, D. R. et al. Individual and community risks of measles and pertussis associated with personal exemptions to immunization. JAMA 284, 3145–3150 (2000).
Salmon, D. A. et al. Health consequences of religious and philosophical exemptions from immunization laws: individual and societal risk of measles. JAMA 282, 47–53 (1999).
Glanz, J. M. et al. Parental refusal of pertussis vaccination is associated with an increased risk of pertussis infection in children. Pediatrics 123, 1446–1451 (2009).
Glanz, J. M. et al. Parental decline of pneumococcal vaccination and risk of pneumococcal related disease in children. Vaccine 29, 994–999 (2011).
Glanz, J. M. et al. Parental refusal of varicella vaccination and the associated risk of varicella infection in children. Arch. Pediatr. Adolesc. Med 164, 66–70 (2010).
Hill, H. A., Elam-Evans, L. D., Yankey, D., Singleton, J. A. & Kang, Y. Vaccination coverage among children aged 19–35 months — United States, 2017. MMWR Morb. Mortal. Wkly. Rep. 67, 1123–1128 (2018).
Olive, J. K., Hotez, P. J., Damania, A. & Nolan, M. S. The state of the antivaccine movement in the United States: a focused examination of nonmedical exemptions in states and counties. PLoS Med. 15, e1002578 (2018).
Mellerson, J. L. et al. Vaccination coverage for selected vaccines and exemption rates among children in kindergarten — United States, 2017–18 school year. MMWR Morb. Mortal. Wkly. Rep. 67, 1115–1122 (2018).
Atwell, J. E. et al. Nonmedical vaccine exemptions and pertussis in California, 2010. Pediatrics 132, 624–630 (2013).
Lieu, T. A., Ray, G. T., Klein, N. P., Chung, C. & Kulldorff, M. Geographic clusters in underimmunization and vaccine refusal. Pediatrics 135, 280–289 (2015).
Omer, S. B. et al. Geographic clustering of nonmedical exemptions to school immunization requirements and associations with geographic clustering of pertussis. Am. J. Epidemiol. 168, 1389–1396 (2008).
2009 Centers for Disease Control and Prevention (CDC). Invasive Haemophilus influenzae type B disease in 5 young children—Minnesota. MMWR Morb. Mortal. Wkly. Rep. 58, 58–60 (2008).
Omer, S. B. et al. Nonmedical exemptions to school immunization requirements: secular trends and association of state policies with pertussis incidence. JAMA 296, 1757–1763 (2006).
Phadke, V. K., Bednarczyk, R. A., Salmon, D. A. & Omer, S. B. Association between vaccine refusal and vaccine-preventable diseases in the United States: a review of measles and pertussis. JAMA 315, 1149–1158 (2016).
Majumder, M. S., Cohn, E. L., Mekaru, S. R., Huston, J. E. & Brownstein, J. S. Substandard vaccination compliance and the 2015 measles outbreak. JAMA Pediatr. 169, 494–495 (2015).
Measles cases in 2018. CDC website. https://www.cdc.gov/measles/cases-outbreaks.html.
Danziger-Isakov, L. & Kumar, D. Vaccination of solid organ transplant candidates and recipients: Guidelines from the American society of transplantation infectious diseases community of practice. Clin. Transplant. (2019).
Rubin, L. G. et al. IDSA clinical practice guideline for vaccination of the immunocompromised host. Clin. Infect. Dis. 58, e44–e100 (2013).
Squires, R. H. et al. Evaluation of the pediatric patient for liver transplantation: 2014 practice guideline by the American Association for the Study of Liver Diseases, American Society of Transplantation and the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition. Hepatology 60, 362–398 (2014).
Blumberg, E. A. et al. Immunogenicity of pneumococcal vaccine in heart transplant recipients. Clin. Infect. Dis. 32, 307–310 (2001).
L’Huillier, A. G. et al. Successful serology-based intervention to increase protection against vaccine-preventable diseases in liver-transplanted children: a 19-yr review of the Swiss national reference center. Pediatr. Transplant. 16, 50–57 (2012).
Feldman, A. G. et al. Immunization Rates at the Time of Pediatric Liver Transplant: A Prospective Multicenter Study through the Studies of Pediatric Liver Transplantation (SPLIT). Hepatology. 68 (Suppl 1), 149A (2018).
Feldman, A. G., Kempe, A., Beaty, B. L. & Sundaram, S. S., Studies of Pediatric Liver Transplantation Research Group. Immunization practices among pediatric transplant hepatologists. Pediatr. Transplant. 20, 1038–1044 (2016).
Ladd, J. M., Karkazis, K. & Magnus, D. Parental refusal of vaccination and transplantation listing decisions: a nationwide survey. Pediatr. Transplant. 17, 244–250 (2013).
2019 United Network for Organ Sharing- Transplant Trends. https://unos.org/data/transplant-trends.
Feldman, A. G., Feudtner, C. & Kempe, A. Reducing the underimmunization of transplant recipients. JAMA Pedia. 172, 111–112 (2018).
Field, R. I. & Caplan, A. L. A proposed ethical framework for vaccine mandates: competing values and the case of HPV. Kennedy Inst. Ethics J. 18, 111–124 (2008).
Campbell, A. L. & Herold, B. C. Immunization of pediatric solid-organ transplantation candidates: immunizations in transplant candidates. Pediatr. Transplant. 9, 652–661 (2005).
Kim, T. H., Johnstone, J. & Loeb, M. Vaccine herd effect. Scand. J. Infect. Dis. 43, 683–689 (2011).
2004 Centers for Disease Control and Prevention (CDC). Epidemiology of measles—United States, 2001. MMWR Morb. Mortal. Wkly. Rep. 53, 713–716 (2003).
Kao, C. M., Schneyer, R. J. & Bocchini, J. A. Jr. Child and adolescent immunizations: selected review of recent US recommendations and literature. Curr. Opin. Pediatr. 26, 383–395 (2014).
Temoka, E. Becoming a vaccine champion: evidence-based interventions to address the challenges of vaccination. S. D. Med. Spec no.: 68–72 (2013).
Sharts-Hopko, N. C. Issues in pediatric immunization. MCN Am. J. Matern. Child Nurs. 34, 80–88 (2009). quiz 89–90.
Anderson, E. L. Recommended solutions to the barriers to immunization in children and adults. Mol. Med. 111, 344–348 (2014).
Esposito, S., Principi, N., Cornaglia, G. & Group, E. V. S. Barriers to the vaccination of children and adolescents and possible solutions. Clin. Microbiol. Infect. 20(Suppl 5), 25–31 (2014).
Feldman, A., Marsh, R., Kempe, A. & Morris, M. Barriers to Pre-transplant Immunization: A Qualitative Study of Pediatric Liver-transplant Stakeholders (American Transplant Congress, Boston, MA, 2019).
Restivo, V. et al. Determinants of influenza vaccination among solid organ transplant recipients attending Sicilian reference center. Hum. Vaccin. Immunother. 13, 346–350 (2017).
Kumar, D. et al. Influenza vaccination in the organ transplant recipient: review and summary recommendations. Am. J. Transplant. 11, 2020–2030 (2011). Practice ASTIDCo.
White-Williams, C. et al. Improving clinical practice: should we give influenza vaccinations to heart transplant patients? J. Heart Lung Transplant. 25, 320–323 (2006).
Krishna, S. & Boren, S. A. Diabetes self-management care via cell phone: a systematic review. J. Diabetes Sci. Technol. 2, 509–517 (2008).
Scherr, D. et al. Effect of home-based telemonitoring using mobile phone technology on the outcome of heart failure patients after an episode of acute decompensation: randomized controlled trial. J. Med. Internet Res. 11, e34 (2009).
Wilson, K., Atkinson, K. M., Deeks, S. L. & Crowcroft, N. S. Improving vaccine registries through mobile technologies: a vision for mobile enhanced Immunization information systems. J. Am. Med. Inf. Assoc. 23, 207–211 (2016).
Wilson, K., Atkinson, K. M. & Penney, G. Development and release of a national immunization app for Canada (ImmunizeCA). Vaccine 33, 1629–1632 (2015).
Wilson, K., Atkinson, K. M. & Westeinde, J. Apps for immunization: Leveraging mobile devices to place the individual at the center of care. Hum. Vaccin. Immunother. 11, 2395–2399 (2015).
Groom, H. et al. Immunization information systems to increase vaccination rates: a community guide systematic review. J. Public Health Manag. Pract. 21, 227–248 (2015).
Szilagyi, P. G. et al. Effect of patient reminder/recall interventions on immunization rates: a review. JAMA 284, 1820–1827 (2000).
Stockwell, M. S. et al. Effect of a text messaging intervention on influenza vaccination in an urban, low-income pediatric and adolescent population: a randomized controlled trial. JAMA 307, 1702–1708 (2012).
Jacobson Vann, J. C., Jacobson, R. M., Coyne-Beasley, T., Asafu-Adjei, J. K. & Szilagyi, P. G. Patient reminder and recall interventions to improve immunization rates. Cochrane Database Syst. Rev. CD003941 (2018).
Briss, P. A. et al. Reviews of evidence regarding interventions to improve vaccination coverage in children, adolescents, and adults. The Task Force on Community Preventive Services. Am. J. Prev. Med. 18, 97–140 (2000).
Szilagyi, P. G. et al. A randomized trial of the effect of centralized reminder/recall on immunizations and preventive care visits for adolescents. Acad. Pediatr. 13, 204–213 (2013).
Kempe, A. et al. Population-based versus practice-based recall for childhood immunizations: a randomized controlled comparative effectiveness trial. Am. J. Public Health 103, 1116–1123 (2013).
Fadda, M., Galimberti, E., Fiordelli, M. & Schulz, P. J. Evaluation of a mobile phone-based intervention to increase parents’ knowledge about the measles-mumps-rubella vaccination and their psychological empowerment: mixed-method approach. JMIR Mhealth Uhealth 6, e59 (2018).
Shojania, K. G., et al. The effects of on-screen, point of care computer reminders on processes and outcomes of care. Cochrane Database Syst Rev. CD001096 (2009).
Fiks, A. G. et al. Effectiveness of decision support for families, clinicians, or both on HPV vaccine receipt. Pediatrics 131, 1114–1124 (2013).
Stockwell, M. S. et al. Registry-linked electronic influenza vaccine provider reminders: a cluster-crossover trial. Pediatrics 135, e75–e82 (2015).
Perkins, R. B. et al. Effectiveness of a provider-focused intervention to improve HPV vaccination rates in boys and girls. Vaccine 33, 1223–1229 (2015).
Kelly, J. S., Zimmerman, L. A., Reed, K. & Enger, K. S. Immunization information systems national research and evaluation agenda. J. Public Health Manag. Pract. 13, 35–38 (2007).
Dempsey, A. F. & Zimet, G. D. Interventions to improve adolescent vaccination: what may work and what still needs to be tested. Vaccine 33(Suppl 4), D106–D113 (2015).
Bentley, T. S. & Phillips, S. J. 2017 U.S. Organ and Tissue Transplant Cost Estimates and Discussion. Milliman Research Report (Milliman, Seattle, WA, 2018).
Lawson, E. F., Trupin, L., Yelin, E. H. & Yazdany, J. Reasons for failure to receive pneumococcal and influenza vaccinations among immunosuppressed patients with systemic lupus erythematosus. Semin. Arthritis Rheum. 44, 666–671 (2015).
Harris, J. G., Maletta, K. I., Ren, B. & Olson, J. C. Improving pneumococcal vaccination in pediatric rheumatology patients. Pediatrics 136, e681–e686 (2015).
Grein, I. H., Groot, N., Lacerda, M. I., Wulffraat, N. & Pileggi, G. HPV infection and vaccination in Systemic Lupus Erythematosus patients: what we really should know. Pediatr. Rheumatol. Online J. 14, 12 (2016).
Yazdany, J. et al. Provision of preventive health care in systemic lupus erythematosus: data from a large observational cohort study. Arthritis Res. Ther. 12, R84 (2010).
Lu, Y. & Bousvaros, A. Immunizations in children with inflammatory bowel disease treated with immunosuppressive therapy. Gastroenterol. Hepatol. (N. Y) 10, 355–363 (2014).
Waszczuk, K., Waszczuk, E., Mulak, A., Szenborn, L. & Paradowski, L. A ‘cocoon immunization strategy’ among patients with inflammatory bowel disease. Eur. J. Gastroenterol. Hepatol. 27, 249–253 (2015).
Soon, I. S., deBruyn, J. C. & Wrobel, I. Immunization history of children with inflammatory bowel disease. Can. J. Gastroenterol. 27, 213–216 (2013).
Selby, L. et al. Receipt of preventive health services by IBD patients is significantly lower than by primary care patients. Inflamm. Bowel Dis. 14, 253–258 (2008).
Kremers, H. M. et al. Preventive medical services among patients with rheumatoid arthritis. J. Rheumatol. 30, 1940–1947 (2003).
Acknowledgements
A.G.F. was funded by a Children’s Hospital Colorado Research Institute Research Scholar Award and an NIH/NCATS Colorado CTSA KL2 TR002534.
Author information
Authors and Affiliations
Contributions
All authors made substantial contributions to conception and design, drafting the article, revising the article, and approving the final version to be published.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Feldman, A.G., Curtis, D.J., Moore, S.L. et al. Under-immunization of pediatric transplant recipients: a call to action for the pediatric community. Pediatr Res 87, 277–281 (2020). https://doi.org/10.1038/s41390-019-0507-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-019-0507-4
This article is cited by
-
Vaccination of immune compromised children—an overview for physicians
European Journal of Pediatrics (2021)
