
Abstract
Background
To better understand children’s adipose tissue (AT) development and distribution, longitudinal data from direct assessment methods are valuable. Previously, we reported sonographic data on abdominal subcutaneous and preperitoneal fat areas ≤1 year of age.
Methods
Sonographic measurements were annually pursued to assess the development of fat compartments in 2–5 year-old children. The effect of sex and correlations with comprehensive anthropometry (e.g., BMI percentiles, skinfold thickness (SFT) measurements, and waist circumference) are presented.
Results
Subcutaneous fat areas increased modestly and were significantly greater in females at each time point investigated. Preperitoneal fat area increased significantly over time (all P values < 0.001) with greater area in females from 3 years onward (e.g., at 3 years estimated mean difference −4.8 mm2; 95% CI: −8.6, −0.9; P = 0.016). The strongest correlations for subcutaneous fat area were consistently observed for SFT measurements. Preperitoneal fat area showed rather weak to moderate correlations, with greater correlation coefficients for SFT measurements compared to waist circumference.
Conclusion
For the first time, longitudinal ultrasound data on abdominal body fat covering preschool age are presented. Evaluation revealed a differential development of fat compartments, depending on children’s age and sex with SFT measurements as the best predictor for both fat depots.
Similar content being viewed by others


Introduction
In view of the rising rate of childhood obesity, an interest in developing new strategies to prevent excess weight gain in infancy and early childhood has intensified.1 Evidence has repeatedly shown that adiposity in childhood can persist through adolescence and into adulthood.2,3,4 A recent meta-analysis confirmed the association estimating that obese children are five times more likely to become obese adults compared to non-obese children.5 At the same time, suitable, valid, and easy-to-handle methods for the assessment of body composition and fat distribution in early infancy up to adolescence are required.6 Waist circumference is often used as an indirect and crude alternative for the assessment of body fat distribution, albeit a distinction between subcutaneous and visceral fat is thereby not possible.7 Importantly, visceral fat, located in the trunk, is considered as an independent risk factor for obesity-related complications, such as cardiovascular disease and type 2 diabetes mellitus.8,9
Two direct methods which are considered gold standards to quantify fat distribution are magnetic resonance imaging (MRI) and computer tomography (CT).10 However, ultrasonography (US) is a promising approach to assess abdominal fat compartments in pediatric populations. Clear advantages over MRI and CT include that US is inexpensive, easy to handle, and portable in field studies. With US, a distinction between fat compartments, such as subcutaneous, preperitoneal, or visceral fat is possible.11 Preperitoneal fat has been shown to be an approximation of visceral fat in children and adults.12,13
Several studies have published US data which assessed different body fat compartments in infancy younger than 1 year of age,6,14,15,16 in early childhood,6,17 and in school-aged children.13,18,19 In 2016, Vogelezang et al. provided US data from 2- to 6-year olds, to investigate the degree of tracking of abdominal fat from 2 to 6 years of age.20 However, research has mainly focused on cross-sectional analysis of body fat. To date, there is paucity of longitudinal sonographic data on abdominal AT development and distribution in preschool age. In addition, few studies have investigated whether sex mediates fat accretion in early childhood.
We previously applied the direct method of US to measure abdominal subcutaneous and preperitoneal AT development and distribution at three time points in infants aged ≤1 year (6 weeks, 4 months, and 1 year) following slight adaptions to the method described by Holzhauer and colleagues.6 The analysis suggested age- and sex-dependent development of subcutaneous and preperitoneal fat areas. Girls tended to have significantly greater subcutaneous fat areas than boys from 6 weeks onward, while preperitoneal area was not influenced by sex in the first year of life. Subcutaneous fat area showed a strong positive correlation with central skinfold thickness (SFT) measurements as well as the sum of 4 SFTs in the first year of life, while preperitoneal fat area was only weakly correlated at 6 weeks and 4 months with a slight increase in central and the sum of 4 SFTs at 1 year.16
The objective of this follow-up study is to investigate the annual development of abdominal subcutaneous and preperitoneal fat measures in preschool children aged 2, 3, 4, and 5 years. The effect of age, sex, and the correlation with comprehensive anthropometric measures are presented.
Methods
Subjects
Data for this study were taken from the INFAT study (impact of nutritional fatty acids during pregnancy and lactation on early human adipose tissue development). The original randomized controlled clinical trial included 208 healthy pregnant women in the Munich area, Germany, and investigated the effect of a reduced n-6/n-3 fatty acid ratio during pregnancy and lactation on offspring’s body composition up to 1 year of life,21,22 with an additional follow-up until the age of 5.23 The study population, design, and outcomes have been previously described.21,22 Approval for the study protocol was obtained from the ethical committee of the Technische Universität München, Germany (1479/06/2009/10/26). Written informed consent from both parents was received for the follow-up study with children aged 2–5 years. No significant differences in growth and body composition between intervention and the control group were observed at any age except for weight and BMI percentiles at 4 years in the unadjusted analysis.23 Thus, pooling of data was possible for this follow-up study.
Anthropometric measurements
Body composition measurement techniques, including weight, height, BMI, and SFT (triceps, biceps, subscapular, and suprailiac) measurements, were performed as explained previously.16 Measurement of waist circumference and BMI percentiles, the latter according to Kromeyer-Hauschild et al.,24 were amended for follow-up analysis. Skinfold regression equations were computed in line with Weststrate and Deurenberg25 to determine body fat mass (kg). Lean body mass (kg) was determined by subtracting fat mass (kg) from body weight (kg).
Sonographic assessment of abdominal subcutaneous and preperitoneal fat
To assess abdominal subcutaneous and preperitoneal fat areas, abdominal US measurements were performed at each visit by trained research physicians/assistants. The method was described previously.16 In brief, subcutaneous and preperitoneal fat were measured in two defined abdominal regions. To estimate subcutaneous and preperitoneal fat areas, the first measurement was performed by placing the US probe in the sagittal plane at the xiphoid process. A second measurement, taken between the xiphoid process and the navel, was performed to estimate subcutaneous fat area in the axial plane. In order to evaluate adipose tissue as fat layers measuring 1 cm in length, we started our measurements at a reference point (i.e., in the sagittal plane the xiphoid process; in the axial plane between the xiphoid process and the navel above the linea alba). Three pictures were evaluated for each area of fat mass. Means of the measured distances were computed to estimate the area of preperitoneal fat in the sagittal plane (preperitoneal areasagittal, mm2), the area of subcutaneous fat in the sagittal plane (subcutaneous areasagittal, mm2), and the area of subcutaneous fat in the axial plane (subcutaneous areaaxial, mm2). In addition, we calculated the ratio of preperitoneal to subcutaneous adipose tissue from the sagittal plane. In our pediatric population ≤1 year, this sonographic method was found to be feasible and reproducible with strong inter- and intra-observer agreements for fat areas (correlation coefficients between 0.97 and 0.99).
Statistical analysis
Sonographic data at 2–5 years are presented as mean ± SD for all, and separately for males and females, respectively. To assess changes in the sonographic fat measures over time, mixed linear models (using unstructured covariance matrices) were fitted with time as a fixed effect, including all measured time points (6 weeks–5 years). To explore how changes over time differ according to sex, sex was added as a fixed effect in the models together with an interaction between sex and time. Estimated mean differences in sex are presented for each measure at each time point, together with 95% confidence intervals. Associations between anthropometric and ultrasound variables were assessed using Spearman–Rho correlation coefficient. Statistical analyses were performed using R (version R 3.1.3; R Foundation for Statistical Computing) and PASW software (version 21, SPSS, Chicago, IL). A two-sided P value < 0.05 was considered statistically significant.
Results
Participants
We analyzed data from 111 children (n = 48 girls, n = 63 boys) at 2 years (median 23.3 months), 103 children (n = 50 girls, n = 53 boys) at 3 years (median 36.3 months), 95 children (n = 44 girls, n = 51 boys) at 4 years (median 48.2 months), and 98 children (n = 48 girls, n = 50 boys) at 5 years of age (median 60.3 months). A flowchart of all participants is given in Supplemental Figure S1. Most listed dropout reasons were a lack of time or relocation of the participating families. No significant differences between individuals who completed the sonographic assessment at 5 years of age from the remaining individuals in socio-demographic and clinical variables were detected (data not shown).
Anthropometric measurements
Anthropometric measurements for all participants divided by age groups are presented in Table 1. Girls showed significant higher values for suprailiac skinfolds from 2 years onward. Significant higher fat mass (calculated from the sum of 4 SFTs) was observed for the first time at 4 years of age with a mean difference of 400 g (95% CI −0.6, −0.1; P = 0.003). In contrast, boys sustained to have significantly more lean body mass between 2 and 5 years of age.
Development of abdominal subcutaneous and preperitoneal fat areas
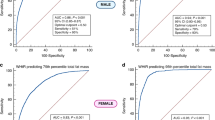
Differences between boys and girls in the development of subcutaneous and preperitoneal fat areas persisted up to 5 years of age with a considerable variation between the sexes in all age groups (Table 2). In addition, Fig. 1 illustrates the effect of age (1a) and sex (1b–d) on subcutaneous and preperitoneal fat measures from previous16 and current findings. Preperitoneal fat area increased significantly from 2 to 5 years of age (all P values < 0.001). Comparatively, subcutaneous fat area modestly increased with significant changes in the axial plane from 2 to 3 years (areaaxial, P = 0.021) and 3 to 4 years (areaaxial, P = 0.030) and from 3 to 4 years in the sagittal plane, respectively (areasagittal, P = 0.033). Subcutaneous fat measurements were significantly higher in females at each time point investigated. While there was no evidence of a difference between sexes in regard to preperitoneal fat area up to the second year of life, data showed significant differences from 3 years onward, with greater area in females (preperitoneal areasagittal at 3 years: estimated mean difference −4.8 mm2; 95% CI: −8.6, −0.9; P = 0.016).

In continuation of a previously published figure (6 wk–1 y),16 the effect of age and sex on abdominal subcutaneous and preperitoneal fat tissue compartments by ultrasound is given (6 wk–5 y), stratified by the time point of investigation. a Comparison of areas of subcutaneous and preperitoneal fat in 6-wk-, 4-mo-, and 1-, 2-, 3-, 4-, and 5-y-old infants/children. b–d Effect of sex on area of subcutaneous fat in the axial plane (b), area of subcutaneous fat in the sagittal plane (c), and area of preperitoneal fat in the sagittal plane (d), stratified by sex. The estimated means and 95% confidence intervals from a mixed linear model with time, sex, and an interaction between sex and time as fixed effects are presented
Correlations of abdominal fat measures with anthropometric outcomes
Table 3 presents Spearman correlation coefficients between abdominal adipose tissue measurements and anthropometric measurements from 2 to 5 years of age. Weak positive correlations were observed between the preperitoneal area and both the suprailiac SFT and the sum of 4 SFTs up to 5 years. We observed similar correlations between the preperitoneal fat area and waist circumference, which was the strongest at 5 years (rs = 0.326, P = 0.001). Estimates for correlation coefficients between the preperitoneal area and other anthropometric measures were similar with the first-year results with the exception of triceps measurements at 3 years (rs = 0.315, P = 0.002) and biceps measurements at 4 years (rs = 0.349, P = 0.001). Subcutaneous fat areas from both the sagittal and axial planes and weight, BMI/BMI percentiles, and skinfolds were moderately to highly correlated, with the highest correlations between subcutaneous fat in the axial plane and suprailiac SFT (at 5 years: rs = 0.809, P value < 0.001). Furthermore, relatively strong correlations were observed between waist circumference and subcutaneous fat areas (subcutaneous areasagittal at 5 years: rs = 0.593; subcutaneous areaaxial at 5 years: rs = 0.577, both P values < 0.001). The ratio of preperitoneal to subcutaneous fat and anthropometric measures were consistently negatively correlated in all age groups.
Discussion
This is the first study that provides a longitudinal overview of fat development throughout both infancy and early childhood up to the 5th year of life. Additionally, these findings give insight into the differences in fat development between boys and girls during early life stages.
Following our cohort up to preschool age, we observed that the preperitoneal fat area steadily increased in mass. Conversely, subcutaneous fat decreased from the first to second year of life, with a slight increase noted from 2 to 5 years of age. Our data showed that subcutaneous fat areas in girls were significantly larger than those observed in boys up to 5 years. In contrast, there was no significant difference in preperitoneal fat areas between infant girls and boys up to 2 years. Notably, from 3 years onward, we observed greater accretion of preperitoneal fat mass in young girls. The relationships between anthropometry and US measurements from 2 to 5 years were similar to the results observed in our cohort of infants ≤ 1 year. Of note, the suprailiac skinfold measure and the sum of 4 SFTs most accurately estimated subcutaneous fat areas, while the relationships between anthropometry and preperitoneal fat areas were rather weak.
A significant increase of 45% of preperitoneal fat area was detected in a cohort of 210 children from the age of 1 to 2 years by Holzhauer et al.6 These results are similar to the 33% average increase of preperitoneal fat which we observed in our population (preperitoneal areasagittal at 1 year: 17.8 mm2, at 2 years: 23.7 mm2; P < 0.001). These results are also in line with a review,26 which concludes that visceral fat accumulation starts early in life. However, in regard to subcutaneous fat, we have seen a significant decrease of the areas in the sagittal and axial planes from 1 to 2 years by 34 and 23% (both P < 0.001), respectively, while Holzhauer et al.6 observed an increase of 1% (P = 0.78). The discordance of findings may be explained by heterogeneity between studies. Notably, our study design was longitudinal and investigated a smaller study population. In contrast, Holzhauer and colleagues’ approach was cross-sectional and examined different children for the two measurement time points. From the ages of 2–5, subcutaneous fat areas remained relatively stable for boys and girls combined. Literature provides evidence that a reduction in fat percentage is observed between 2 and 5 years,7 with a minimum of body fat at 5–7 years, before body fatness increases into adulthood, referred to as adiposity rebound.27,28
Convincing evidence demonstrates sex-specific differences in adipose tissue depots in adults with higher volumes of subcutaneous fat in women, and higher visceral fat volumes in men.29 Existing data on gender differences in early infancy through childhood are limited and have not yet been clearly identified, as inconsistencies across studies exist.30,31 In contrast to those in adults, several studies have shown significantly higher rates of intraabdominal AT growth in girls compared to boys, yet the age at which point the shift happens differs between studies.6,18,19,32,33 Shen et al. investigated subcutaneous AT depots by MRI in a cohort of 499 children and adults aged 5–88 years. The results from this cross-sectional study suggest that subcutaneous AT volumes are larger in females of all ages. Of note, the total visceral AT volume was also greater in females until 12 years, at which point males were observed to have larger visceral AT volumes.34 The Generation R study examined fat depots in 199 boys and 194 girls at 2 and 6 years. They observed that a larger area of subcutaneous fat was already present in 2-year-old girls, and that preperitoneal fat area was considerably larger in girls at 6, but not at 2 years.20 Our data confirm these results, suggesting that sex-differential adipose tissue expansion develops very early in childhood. In contrast, higher volumes of visceral fat, measured by US, has been observed in boys compared to girls at 12 months (n = 258 boys, n = 237 girls; P = 0.04), but not at 3 months (n = 254 boys, n = 233 girls; P = 0.9), while subcutaneous volumes did not differ significantly at both time points.14 Higher volumes of intraabdominal, abdominal, and subcutaneous AT were observed by Benfield et al.32 in a group of 74 13-year-old girls compared to a sample of 96 male counterparts. In addition, they reported a significantly higher ratio of preperitoneal to subcutaneous fat areas in teenage boys, which, they suggest, may indicate the beginning of sexual dimorphism in fat patterning. However, we observed a significantly higher ratio in boys for the first time at 3 years of age, and others have seen this pattern appear between 2 and 7 years of age, which suggests more AT deposited intra-abdominally.17,20,35 Research indicates that the shift in visceral fat most likely emerges during the pubertal/early postpubertal period, with sexual maturation and hormone secretion as important determinants for this change. Longitudinal studies in early childhood could elucidate our understanding of the differences in growth patterns of subcutaneous and preperitoneal/intraabdominal fat development between boys and girls.31 It is particularly interesting that when employing indirect methods to measure AT (via SFT measurement), significant sex differences in fat mass were first detectable at 4 years.
The best indirect predictor of intraabdominal fat mass in adolescents between 7 and 16 years is waist circumference measurement, which accounts for 64.8% of the variance in visceral AT.36 This measurement has also been used to estimate abdominal fat mass in young children,7 although a validation study indicated that waist circumference as a predictor of visceral fat in newborns is likely to be unreliable in early life, showing almost no relationship to visceral AT volume measured by MRI (r = 0.08, P > 0.05). Conversely, visceral AT assessed by US and visceral AT measured by MRI were significantly positively correlated (r = 0.48, P < 0.05).14 Our results also showed rather weak correlations between preperitoneal fat areas and waist circumference with the highest value at 5 years (r = 0.326, P = 0.001) and confirm previous findings. Comparatively, SFT measurements, especially the suprailiac skinfold, was more strongly associated.
Admittedly, our study has some limitations. As we have made small adaptations to a published sonographic technique,6 our study is lacking a gold standard for validation. Further, we have a defined cohort of healthy, mostly normal-weight German children of Caucasian origin with a small sample size that is decreasing by study duration. All aspects combined results in conclusions that cannot be generalized. Nevertheless, this follow-up study is unique, as it presents for the first time longitudinal US data for children from birth until 1 year,16 with a follow-up to 5 years of age. Further, the study offers an extensive set of direct and indirect methods for the assessment of body composition, which enables comparisons between the different methods.
In conclusion, this is the first time that longitudinal US data spanning the first 5 years of life starting in early infancy until early childhood are presented. In this follow-up study from 2 to 5 years of life, the evaluation revealed a differential development of abdominal subcutaneous and preperitoneal fat, depending on children’s age and sex. Thus, our results strongly suggest to use direct techniques such as US for future prospective studies of AT development and fat distribution. In addition, it is crucial in this context to consider both sex- as well as fat depot-specific differences in AT growth trajectories in early childhood.
References
Ahrens, W. et al. Prevalence of overweight and obesity in European children below the age of 10. Int. J. Obes. 2014(Suppl 2), S99–S107 (2005). 38.
Whitaker, R. C., Wright, J. A., Pepe, M. S., Seidel, K. D. & Dietz, W. H. Predicting obesity in young adulthood from childhood and parental obesity. N. Engl. J. Med. 337, 869–873 (1997).
Durmus, B. et al. Growth in foetal life and infancy is associated with abdominal adiposity at the age of 2 years: the generation R study. Clin. Endocrinol. 72, 633–640 (2010).
Peneau, S. et al. Body size and growth from birth to 2 years and risk of overweight at 7–9 years. Int. J. Pediatr. Obes. 6, e162–e169 (2011).
Simmonds, M. et al. The use of measures of obesity in childhood for predicting obesity and the development of obesity-related diseases in adulthood: a systematic review and meta-analysis. Health Technol. Assess. 19, 1–336 (2015).
Holzhauer, S. et al. Sonographic assessment of abdominal fat distribution in infancy. Eur. J. Epidemiol. 24, 521–529 (2009).
Toro-Ramos, T., Paley, C., Pi-Sunyer, F. X. & Gallagher, D. Body composition during fetal development and infancy through the age of 5 years. Eur. J. Clin. Nutr. 69, 1279–1289 (2015).
Kissebah, A. H. & Krakower, G. R. Regional adiposity and morbidity. Physiol. Rev. 74, 761–811 (1994).
Demerath, E. W. et al. Visceral adiposity and its anatomical distribution as predictors of the metabolic syndrome and cardiometabolic risk factor levels. Am. J. Clin. Nutr. 88, 1263–1271 (2008).
Wells, J. C. Body composition in infants: evidence for developmental programming and techniques for measurement. Rev. Endocr. Metab. Disord. 13, 93–101 (2012).
Horan, M., Gibney, E., Molloy, E. & McAuliffe, F. Methodologies to assess paediatric adiposity. Ir. J. Med. Sci. 184, 53–68 (2015).
Suzuki, R. et al. Abdominal wall fat index, estimated by ultrasonography, for assessment of the ratio of visceral fat to subcutaneous fat in the abdomen. Am. J. Med. 95, 309–314 (1993).
Mook-Kanamori, D. O. et al. Abdominal fat in children measured by ultrasound and computed tomography. Ultrasound Med. Biol. 35, 1938–1946 (2009).
De Lucia Rolfe, E. et al. Ultrasound estimates of visceral and subcutaneous-abdominal adipose tissues in infancy. J. Obes. 2013, 951954 (2013).
Uebel, K. et al. Effect of maternal obesity with and without gestational diabetes on offspring subcutaneous and preperitoneal adipose tissue development from birth up to year-1. BMC Pregnancy Childbirth 14, 138 (2014).
Brei, C. et al. Sonographic assessment of abdominal fat distribution during the first year of infancy. Pediatr. Res. 78, 342–350 (2015).
Gruszfeld, D. et al. Association of early protein intake and pre-peritoneal fat at five years of age: Follow-up of a randomized clinical trial. Nutr. Metab. Cardiovasc Dis. 26, 824–832 (2016).
Gishti, O. et al. Fetal and infant growth patterns associated with total and abdominal fat distribution in school-age children. J. Clin. Endocrinol. Metab. 99, 2557–2566 (2014).
Santos, S. et al. Associations of infant subcutaneous fat mass with total and abdominal fat mass at school-age: The Generation R Study. Paediatr. Perinat. Epidemiol. 30, 511–520 (2016).
Vogelezang, S. et al. Tracking of abdominal subcutaneous and preperitoneal fat mass during childhood. The Generation R Study. Int. J. Obes. 2016, 595–600 (2005).
Hauner, H. et al. The impact of nutritional fatty acids during pregnancy and lactation on early human adipose tissue development. Rationale and design of the INFAT study. Ann. Nutr. Metab. 54, 97–103 (2009).
Hauner, H. et al. Effect of reducing the n-6:n-3 long-chain PUFA ratio during pregnancy and lactation on infant adipose tissue growth within the first year of life: an open-label randomized controlled trial. Am. J. Clin. Nutr. 95, 383–394 (2012).
Brei, C. et al. Reduction of the n-6:n-3 long-chain PUFA ratio during pregnancy and lactation on offspring body composition: follow-up results from a randomized controlled trial up to 5 y of age. Am. J. Clin. Nutr. 103, 1472–1481 (2016).
Kromeyer-Hauschild, K. et al. Percentiles of body mass index in children and adolescents evaluated from different regional German studies. Mon. Kinderheilkd. 8, 807–819 (2001).
Weststrate, J. & Deurenberg, P. Body composition in children: proposal for a method for calculating body fat percentage from total body density or skinfold thickness measurements. Am. J. Clin. Nutr. 50, 1104–1115 (1989).
Samara, A., Ventura, E. E., Alfadda, A. A. & Goran, M. I. Use of MRI and CT for fat imaging in children and youth: what have we learned about obesity, fat distribution and metabolic disease risk? Obes. Rev. 13, 723–732 (2012).
Hughes, A. R., Sherriff, A., Ness, A. R. & Reilly, J. J. Timing of adiposity rebound and adiposity in adolescence. Pediatrics 134, e1354–e1361 (2014).
Rolland-Cachera, M. F. & Peneau, S. Growth trajectories associated with adult obesity. World Rev. Nutr. Diet. 106, 127–134 (2013).
Taylor, R. W., Grant, A. M., Williams, S. M. & Goulding, A. Sex differences in regional body fat distribution from pre- to postpuberty. Obesity 18, 1410–1416 (2010).
Staiano, A. E. & Katzmarzyk, P. T. Ethnic and sex differences in body fat and visceral and subcutaneous adiposity in children and adolescents. Int. J. Obes. 2012, 1261–1269 (2005).
Staiano, A. E., Broyles, S. T., Gupta, A. K. & Katzmarzyk, P. T. Ethnic and sex differences in visceral, subcutaneous, and total body fat in children and adolescents. Obesity 21, 1251–1255 (2013).
Benfield, L. L. et al. Magnetic resonance imaging of abdominal adiposity in a large cohort of British children. Int. J. Obes. 2008, 91–99 (2005).
Gruszfeld D., et al. Leptin and adiponectin serum levels from infancy to school age: factors influencing tracking. Childhood Obesity. 12, 178–187 (2016).
Shen, W. et al. Sexual dimorphism of adipose tissue distribution across the lifespan: a cross-sectional whole-body magnetic resonance imaging study. Nutr. Metab. 6, 17 (2009).
Liem, E. T. et al. Measuring abdominal adiposity in 6 to 7-year-old children. Eur. J. Clin. Nutr. 63, 835–841 (2009).
Brambilla, P. et al. Crossvalidation of anthropometry against magnetic resonance imaging for the assessment of visceral and subcutaneous adipose tissue in children. Int. J. Obes. 2006, 23–30 (2005).
Acknowledgements
We thank all families, willing to participate in the study and our colleagues D.M. Meyer, U. Amann-Gassner, C. Spier, E. Heimberg, V. Schulte, K. Pusch, J.S. Bauer, and E. Rummeny. The content of this manuscript is partly published in the PhD thesis of Christina Brei (http://nbn-resolving.de/urn/resolver.pl?urn:nbn:de:bvb:91-diss-20171130-1360854-1-3). Supported by grants from the Else Kröner-Fresenius Foundation, Bad Homburg; the International Unilever Foundation, Hamburg; the European Union-funded Early Nutrition Programming Project (EARNEST) consortium (FOOD-CT-2005-007036); the German Ministry of Education and Research via the Competence Network Obesity (Kompetenznetz Adipositas, 01GI0842); and Danone Research-Centre for Specialised Nutrition, Friedrichsdorf, Germany. There was no intervention from any sponsor with any of the research aspects of the study, including study design, intervention, data collection, analysis, and interpretation, or writing of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
About this article

Cite this article
Brei, C., Much, D., Brunner, S. et al. Longitudinal sonographic assessment of abdominal fat distribution from 2 to 5 years of age. Pediatr Res 84, 677–683 (2018). https://doi.org/10.1038/s41390-018-0147-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41390-018-0147-0
This article is cited by
-
Mid-pregnancy weight gain is associated with offspring adiposity outcomes in early childhood
Pediatric Research (2021)
