
Abstract
Background
The pathophysiology of tinnitus is not yet fully understood. Although there is a large amount of evidence associating traffic noise exposure with non-auditory health outcomes, there is no evidence regarding the impact of noise annoyance on auditory disorders such as tinnitus.
Objective
Thus, we aimed to investigate the association between noise annoyance due to different sources and tinnitus presence and distress in the general population.
Methods
Data of 6813 participants from a large German population-based cohort were used (Gutenberg Health Study). Participants were asked about the presence of tinnitus and how much they were bothered by it. In addition, information on annoyance from road traffic, aircraft, railways, industrial, and neighborhood noise during the day and sleep was collected through validated questionnaires.
Results
The prevalence of tinnitus was 27.3%, and the predominant sources of noise annoyance in these subjects were aircraft, neighborhood, and road traffic noise. Overall, logistic regression results demonstrated consistent positive associations between annoyance due to different noise sources and prevalent risk of tinnitus with increases in odds ratios ranging from 4 to 11% after adjustment for sex, age, and socioeconomic status. Likewise, consistent increases in odds ratios were observed for tinnitus distress in subjects with prevalent tinnitus. For instance, neighborhood noise annoyance during the sleep was associated with a 26% increase in tinnitus distress (OR 1.26, 95% CI 1.13; 1.39).
Impact
This is the first study investigating the association between noise annoyance and tinnitus presence and distress in a large cohort of the general population. Our results indicate consistent and positive associations between various sources of noise annoyance and tinnitus. These unprecedented findings are highly relevant as noise annoyance and tinnitus are widespread. The precise etiology and locus of tinnitus remain unknown, but excessive noise exposure is thought to be among the major causes. This study suggests that transportation and neighborhood noise levels thought merely to contribute to annoyance and non-auditory health effects may be sufficient to cause or exacerbate tinnitus.
Similar content being viewed by others

Introduction
The term tinnitus is defined as the conscious perception of a sound in the absence of a stimulus from an external acoustic source [1]. The pathophysiology of tinnitus is complex and multifactorial [2, 3]. Tinnitus, arising from pathological changes in the auditory pathway, often develops due to initial cochlear lesions like sudden hearing loss, noise trauma, presbyacusis, or ototoxic drug use. The association between hearing loss and tinnitus is intricate, with not all hearing-impaired individuals experiencing tinnitus, and abnormal audiograms not universally present in those with tinnitus. Additionally, partial cochlear nerve sections may not impact hearing thresholds, and tinnitus in those with normal hearing may be linked to cochlear dead regions or outer hair cell damage. Tinnitus onset can be influenced by temporomandibular joint disorders, neck injuries, emotional stress, and trauma. The multifactorial nature of tinnitus involves a combination of altered auditory and somatosensory inputs, abnormal central nervous system activity, and emotional factors, particularly evident in tinnitus following traumatic head injuries. The factors contributing to tinnitus generation may differ from those related to its persistence, as seen in cases of transient tinnitus after noise trauma [2, 3]. Exacerbating factors related to the transition from acute to chronic tinnitus may include mental stress, other psychological factors, and tinnitus-related distress [4, 5]. Interestingly, the hypothesis was put forward that stress per se may cause tinnitus [6]. In particular, it was demonstrated that stressful situations and sleep disturbances precede tinnitus onset and progression from mild to bothersome symptoms [7,8,9]. As stress and sleep disturbance are proposed key mechanisms behind the harmful health effects of environmental noise exposure [10, 11], the hypothesis was formulated that exposure to transportation noise levels—typically below the thresholds associated with hearing damage [12]—can influence the onset and discomfort caused by tinnitus. Indeed, a recent nationwide cohort study from Denmark demonstrated that residential exposure to road traffic noise may increase risk of incident tinnitus [13]. However, it remains to be established whether noise annoyance, which is regarded as an important effect modifier of the relation between noise exposure and non-auditory health outcomes including cardiovascular disease [14], is associated with tinnitus.
Noise annoyance may be an interesting indicator to investigate in this setting. Firstly, noise annoyance strongly correlates with mental stress and health outcomes such as depression and anxiety [15]. Secondly, noise annoyance is among the most significant effects in the general population caused by environmental noise exposure [10]. Moreover, the World Health Organization acknowledged in 2018 that studies investigating the association between transportation noise and hearing-related outcomes, such as tinnitus, are lacking [16].
To the best of our knowledge, there are no studies to date examining the association between noise annoyance and prevalent risk of tinnitus as well as tinnitus distress in the general population. Thus, we used data from a large population-based cohort associating noise annoyance due to different sources and tinnitus presence and distress.
Methods
Study design and sample
Data from the Gutenberg Health Study (GHS) were used for analysis. Comprehensive information on the study design and details were published previously [17, 18]. In brief, 15,010 individuals (aged 35–74 years, core cohort) underwent a standardized 5-h-long baseline-examination performed from 2007 to 2012 at the study center of the University Medical Center Mainz, Germany. These examinations included a variety of interviews and clinical examinations conducted in compliance with standard protocols. The follow-up examinations took place 5 and 10 years after enrollment, i.e., from 2012 to 2017 and from 2017 to 2022. At this 10-year follow-up (from 2017 to 2020), otologic testing was included in the study design. In addition to the core cohort, new participants aged 25–44 years (young cohort, n = 4000) and 75–85 years (senior cohort, n = 1000) were recruited. All three cohorts will be followed up in 10-year increments through 2027 [19].
All procedures conducted in the GHS were approved by the ethics committee of the Statutory Physician Board of the State Rhineland-Palatinate [reference number 837.020.07(5555)] and the local data safety commissioners and were in line with the ethical principles for medical research involving human subjects as outlined in the Declaration of Helsinki. Before inclusion in the study, written informed consent was obtained from each participant.
Noise annoyance
Noise annoyance was measured in a standardized and validated manner as reported recently [20, 21] and endorsed by the International Commission on Biological Effects of Noise (ICBEN) in 2001 [22]. Using a five-point Likert scale with distinct semantic differentiations, approximately equidistant from each other, ranging from “not at all,” over “slightly,” “moderately,” and “strongly” to “extremely,” participants were asked to rate “how annoyed have you been in the past years by … during the day/in your sleep?”. Various sources of noise annoyance including road traffic, aircraft, railway, industrial, and neighborhood noise were assessed. The calculation of overall noise annoyance involved considering the highest annoyance rating reported by participants, irrespective of the specific noise source or whether the annoyance occurred during the day or in their sleep. Overall noise annoyance represents a comprehensive measure that captures the participants’ highest reported level of annoyance, encompassing various noise sources such as road traffic, aircraft, railway, industrial, and neighborhood noise. This calculation disregards the distinction between daytime and sleep-related annoyance, focusing on the intensity of the overall experience. Additionally, source-specific overall noise annoyance narrows down the focus to the specific noise source that contributed the most to an individual’s overall noise annoyance, regardless of its impact on daytime or sleep. This approach aims to provide a more detailed understanding of how different noise sources contribute to the participants’ overall perception of annoyance. Both overall noise annoyance and source-specific overall noise annoyance can be understood as continuous variables, given that they result from the 5-point Likert scale.
Tinnitus presence and distress
During a standardized interview, participants were asked to complete a questionnaire about their auditory quality of life including standardized questions on tinnitus presence and distress [19]: “Do you suffer from ringing in the ears (tinnitus)?” with a binary answer format (yes/no) and “How much do you feel bothered by it?” with a six-level answer format and Likert scale ranging from 0 (“not stressful”) to 5 (“very stressful”).
Statistical analysis
Participants with missing data on noise annoyance were excluded from the analysis. Differences in continuous study sample characteristics, such as age and socioeconomic status, were assessed using the t-test. For dichotomous variables, such as sex, the chi-square test was employed. Binary logistic regression analysis with corresponding odds ratios (OR), 95% CI, and P values were used to determine the relationship between noise annoyance and prevalent tinnitus. Noise annoyance was treated as a continuous variable (per point increase) in all models. In those participants with prevalent tinnitus, ordinal logistic regression analysis with proportional odds assumption modeling for tinnitus distress was performed. Statistical analysis included sequential adjustment. Model 1 was adjusted for sex (binary). Model 2 was additionally adjusted for age (continuous). Model 3 was additionally adjusted for socioeconomic status (continuous). The socioeconomic status was assessed by a validated index score (ranging from 3 (lowest) to 21 (highest)), providing information about education, occupation, and household net-income [23, 24]. In the present analysis, P-values should be interpreted as a continuous measure of evidence against the null hypothesis, and they are therefore reported exactly. For descriptive reasons, P-values < 0.05 were regarded as important associations. The statistical data analyses were performed using the software R (http://www.r-project.org/).
Results
Study sample characteristics
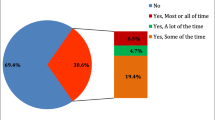
After excluding participants without information on noise annoyance, a total of N = 6,813 participants were included in the present analysis. Among these, 1,862 (27.3%) suffered from tinnitus. In participants with prevalent tinnitus, more than the half reported no (rating 0–24.7%) or little (rating 1-34.8%) suffering from tinnitus. Participants with prevalent tinnitus were more likely to be men (56.5%, P < 0.0001), were older (mean age 58.0 ± 10.8 vs. 55.8 ± 11.8, P < 0.0001), and had a slightly lower socioeconomic status (14.33 ± 4.18 vs. 14.46 ± 4.15, P = 0.27). Overall, annoyance due to aircraft (63.6%), neighborhood (46.8%), and road traffic (46.3%) noise were most frequent in participants with prevalent tinnitus.
Association between noise annoyance and prevalent tinnitus
Tables 1 and 2 show the results of the logistic regression analysis concerning the association between noise annoyance and prevalent tinnitus. In general, consistent positive associations between annoyance due to different noise sources and prevalent risk of tinnitus were observed. Increases in ORs ranged from 4 to 11% after multivariable adjustment with industrial noise annoyance during the day displaying an OR of 1.11 (95% CI 1.03; 1.19).
Association between noise annoyance and tinnitus distress
Tables 3 and 4 show the results of the logistic regression analysis regarding the association between noise annoyance and tinnitus distress in participants with prevalent tinnitus. Again, consistent positive associations between annoyance due to different noise sources and tinnitus distress were observed. Increases in ORs up to 26% after multivariable adjustment were observed. Herein, neighborhood noise annoyance during the sleep was associated with a 26% increase in tinnitus distress (OR 1.26, 95% CI 1.13; 1.39).
Discussion
To the best of our knowledge, this is the first study that observed an association between noise annoyance due to different sources and tinnitus presence and distress in a large cohort of the general population. Notably, the prevalence of tinnitus was 27.3%, being a representative estimate when comparing with previous estimates indicating a prevalence range from 9 to 28% in Europe [25]. Overall, we observed consistent and positive OR increases for the association between noise annoyance and prevalent tinnitus, which were robust to adjustment for sex, age, and socioeconomic status. No substantial OR differences between noise annoyance during the day and sleep were observed. Likewise, there was a consistent and positive association between noise annoyance and tinnitus distress in participants with prevalent tinnitus after multivariable adjustment. Our results strongly show that noise annoyance can be a reliable indicator of tinnitus presence and distress. Importantly, future studies have to investigate whether noise annoyance can also predict the onset of tinnitus.
Our results are in accordance with a recently published study from Cantuaria et al. that found a positive association between noise exposure and incident tinnitus [13]. In this nationwide cohort study including all residents from Denmark aged ≥ 30 years (40,692 were diagnosed with tinnitus at follow-up), the authors observed an increased hazard ratio of 1.06 (95% CI 1.04; 1.08) per 10 dB increase in road traffic noise exposure. Consequently, the authors concluded that road traffic noise exposure can negatively affect the auditory system. However, it is well-established that environmental noise exposure acts as a psychosocial stressor. According to the noise reaction scheme developed by Babisch [26], exposure to excessive noise levels can via an direct pathway induce hearing organ damage and sleep disturbance leading to neuroendocrine stress responses and thus to onset and progression of chronic non-communicable disease including cardiovascular disease [27, 28]. The indirect pathway refers to the exposure of lower noise levels, compatible with the exposure to traffic noise, interfering with daily activities, communication, and sleep, thus promoting stress responses and impairing health. Understanding the auditory system involves considering the pathway from the cochlea to the temporal cortex. Different points along this route could contribute to the perception of tinnitus. The primary impact of noise is typically on the outer hair cells in the cochlea, leading to noise-induced hearing loss. However, research suggests that noise exposure goes beyond causing damage to outer hair cells, it can also result in synaptopathy, affecting the synapses between inner hair cells and the spiral ganglion neuron. Thus, it is likely that a certain level of noise intensity, higher than typical environmental noise exposure levels, is necessary for these effects to occur. While environmental noise exposure is rather not likely to cause distinct cochlear damage, it is considered a potential factor in triggering tinnitus perception via the induction of neuroplastic changes in the central auditory system. The complex interplay between environmental noise, the structural integrity of the auditory system, and the intricacies of tinnitus perception highlights the multifaceted nature of the auditory response to noise exposure [2, 3]. Our results expand on the findings of Cantuaria et al. [13] by indicating that also non-traffic noise annoyance such as neighborhood and industrial noise annoyance associate with tinnitus presence as well as distress. These findings are in line with the evidence that stress may play a major role in the development, maintenance, and worsening of tinnitus [7, 29].
On a more mechanistic level, increased stress hormone levels may negatively affect the limbic, reticular, and auditory systems, thereby initiating or aggravating tinnitus [30]. An increase in stress hormone levels is likely accompanied by inflammatory and oxidative stress processes. A series of human and animal studies conducted by our research group demonstrated that traffic noise exposure could increase stress hormone levels, disturb sleep, and increase inflammation and oxidative stress, leading to vascular endothelial dysfunction (for overview see [27]). Indeed, there is evidence showing a close relationship between oxidative stress, nitric oxide, endothelial dysfunction, and tinnitus [31]. Study results from Neri et al. suggested that in acute tinnitus patients, levels of oxidative stress are increased and nitric oxide production is reduced being able to induce cerebrovascular endothelial dysfunction, which in turn induce a dysfunction of the microcirculation of the inner ear [31]. However, it is important to note that chronic tinnitus associated with long-term stress may not have a direct correlation with the microcirculation of the inner ear. The relationship between chronic stress and tinnitus likely involves intricate interactions across neural and psychological factors, necessitating further research for a comprehensive understanding [6, 9].
Disturbed sleep by noise exposure may also constitute an important underlying mechanism, as studies not only demonstrated impaired sleep in tinnitus patients but also sleep disturbance to precede tinnitus distress [32]. In support of this, we have recently demonstrated that noise annoyance can predict the onset of sleep disturbance in the GHS [15]. In this setting, a vicious cycle can be triggered in which sleep disturbance would worsen tinnitus symptoms and more bothersome symptoms would lead to impaired sleep [33]. In favor of this, tinnitus was shown to be louder and more distressing during the night and in the early morning [34]. Thus, it can be hypothesized that noise-induced stress and annoyance during the night along with fragmentation of sleep, may increase tinnitus patients’ awareness of tinnitus and subsequent level of distress when they try to resume sleep [13].
The present study has strengths and potential limitations. Strengths of the present study include the underlying large dataset from a large population-representative sample from Germany. Some important limitations, however, need to be considered. First, the observational and cross-sectional nature of the study does not allow for causal inferences. Noise annoyance and the outcomes of interest were assessed by personal interviews and partly validated questionnaires only that largely depend on the individual compliance. Specifically, we did not include the duration of tinnitus or differentiate between intermittent and continuous symptoms in our questionnaire. Unlike common definitions that specify sounds lasting for more than five minutes, our questionnaire did not set a minimum duration for tinnitus symptoms. These factors may influence the prevalence and characterization of tinnitus in our study, potentially affecting the comparability of our findings with research that uses different tinnitus definitions. However, diagnosing tinnitus is complicated as there is no objective test or a single organic correlate to confirm the occurrence of the disorder. Furthermore, there is likely a bidirectional relationship between noise annoyance and tinnitus (distress), which we did not analyze. However, it is important to note that evidence of a bidirectional association does not necessarily negate causal explanations in one or both directions of an association.
To the best of our knowledge, this is the first study investigating the association between noise annoyance and tinnitus presence and distress in a large cohort of the general population. Our results indicate consistent and positive associations between various sources of noise annoyance and the outcomes of interest. Potential mechanisms underlying these relationships refer to the noise reaction scheme. However, large prospective studies providing deep mechanistic insight are needed to confirm the proposed mechanisms.
Data availability
The analysis presents clinical data of a large-scale population-based cohort with ongoing follow-up examinations. This project constitutes a major scientific effort with high methodological standards and detailed guidelines for analysis and publication to ensure scientific analyses on the highest level. Therefore, data are not made available for the scientific community outside the established and controlled workflows and algorithms. To meet the general idea of verification and reproducibility of scientific findings, we offer access to data at the local database in accordance with the ethics vote on request at any time. The GHS steering committee, which comprises a member of each involved department and the head of the GHS, convenes once a month. The steering committee decides on internal and external access of researchers and use of the data and biomaterials based on a research proposal to be supplied by the researcher. Interested researchers make their requests to the head of the GHS (Philipp S. Wild, philipp.wild@unimedizin-mainz.de).
References
Baguley D, McFerran D, Hall D. Tinnitus. Lancet. 2013;382:1600–7.
Haider HF, Bojic T, Ribeiro SF, Paco J, Hall DA, Szczepek AJ. Pathophysiology of Subjective Tinnitus: Triggers and Maintenance. Front Neurosci. 2018;12:866.
Langguth B, Kreuzer PM, Kleinjung T, De Ridder D. Tinnitus: causes and clinical management. Lancet Neurol. 2013;12:920–30.
Wallhausser-Franke E, D’Amelio R, Glauner A, Delb W, Servais JJ, Hormann K, et al. Transition from Acute to Chronic Tinnitus: Predictors for the Development of Chronic Distressing Tinnitus. Front Neurol. 2017;8:605.
Biehl R, Boecking B, Brueggemann P, Grosse R, Mazurek B. Personality Traits, Perceived Stress, and Tinnitus-Related Distress in Patients With Chronic Tinnitus: Support for a Vulnerability-Stress Model. Front Psychol. 2019;10:3093.
Patil JD, Alrashid MA, Eltabbakh A, Fredericks S. The association between stress, emotional states, and tinnitus: a mini-review. Front Aging Neurosci. 2023;15:1131979.
Betz LT, Muhlberger A, Langguth B, Schecklmann M. Stress Reactivity in Chronic Tinnitus. Sci Rep. 2017;7:41521.
Rauschecker JP, Leaver AM, Muhlau M. Tuning out the noise: limbic-auditory interactions in tinnitus. Neuron. 2010;66:819–26.
Mazurek B, Boecking B, Brueggemann P. Association Between Stress and Tinnitus-New Aspects. Otol Neurotol. 2019;40:e467–73.
Hahad O, Kroller-Schon S, Daiber A, Munzel T. The Cardiovascular Effects of Noise. Dtsch Arztebl Int. 2019;116:245–50.
Hahad O, Prochaska JH, Daiber A, Muenzel T. Environmental Noise-Induced Effects on Stress Hormones, Oxidative Stress, and Vascular Dysfunction: Key Factors in the Relationship between Cerebrocardiovascular and Psychological Disorders. Oxid Med Cell Longev. 2019;2019:4623109.
Fink DJ. What Is a Safe Noise Level for the Public? Am J Public Health. 2017;107:44–5.
Cantuaria ML, Pedersen ER, Poulsen AH, Raaschou-Nielsen O, Hvidtfeldt UA, Levin G, et al. Transportation Noise and Risk of Tinnitus: A Nationwide Cohort Study from Denmark. Environ Health Perspect. 2023;131:27001.
Babisch W, Pershagen G, Selander J, Houthuijs D, Breugelmans O, Cadum E, et al. Noise annoyance-a modifier of the association between noise level and cardiovascular health? Sci Total Environ. 2013;452-453:50–7.
Beutel ME, Brahler E, Ernst M, Klein E, Reiner I, Wiltink J, et al. Noise annoyance predicts symptoms of depression, anxiety and sleep disturbance 5 years later. Findings from the Gutenberg Health Study. Eur J Public Health. 2020;30:516–21.
Environmental Noise Guidelines for the European Region: World Health Organization; 2018. Available from: https://www.who.int/europe/publications/i/item/9789289053563.
Hahad O, Wild PS, Prochaska JH, Schulz A, Hermanns I, Lackner KJ, et al. Endothelial Function Assessed by Digital Volume Plethysmography Predicts the Development and Progression of Type 2 Diabetes Mellitus. J Am Heart Assoc. 2019;8:e012509.
Hahad O, Arnold N, Prochaska JH, Panova-Noeva M, Schulz A, Lackner KJ, et al. Cigarette Smoking Is Related to Endothelial Dysfunction of Resistance, but Not Conduit Arteries in the General Population-Results From the Gutenberg Health Study. Front Cardiovasc Med. 2021;8:674622.
Hackenberg B, Doge J, O’Brien K, Bohnert A, Lackner KJ, Beutel ME, et al. Tinnitus and Its Relation to Depression, Anxiety, and Stress-A Population-Based Cohort Study. J Clin Med. 2023;12:1169.
Hahad O, Beutel ME, Gilan DA, Chalabi J, Schuster AK, Gianicolo E, et al. Noise annoyance and risk of prevalent and incident atrial fibrillation-A sex-specific analysis. Front Public Health. 2022;10:1061328.
Hahad O, Beutel M, Gori T, Schulz A, Blettner M, Pfeiffer N, et al. Annoyance to different noise sources is associated with atrial fibrillation in the Gutenberg Health Study. Int J Cardiol. 2018;264:79–84.
Fields JM, De Jong RG, Gjestland T, Flindell IH, Job RFS, Kurra S, et al. Standardized general-purpose noise reaction questions for community noise surveys: research and a recommendation. J Sound Vib. 2001;242:641–79.
Lampert T, Kroll L, Muters S, Stolzenberg H. [Measurement of socioeconomic status in the German Health Interview and Examination Survey for Adults (DEGS1)]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2013;56:631–6.
Lampert T, Kroll LE, Muters S, Stolzenberg H. [Measurement of the socioeconomic status within the German Health Update 2009 (GEDA)]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2013;56:131–43.
Biswas R, Lugo A, Akeroyd MA, Schlee W, Gallus S, Hall DA. Tinnitus prevalence in Europe: a multi-country cross-sectional population study. Lancet Reg Health Eur. 2022;12:100250.
Babisch W. The Noise/Stress Concept, Risk Assessment and Research Needs. Noise Health. 2002;4:1–11.
Munzel T, Sorensen M, Daiber A. Transportation noise pollution and cardiovascular disease. Nat Rev Cardiol. 2021;18:619–36.
Munzel T, Treede H, Hahad O, Daiber A. Too Loud to Handle? Transportation Noise and Cardiovascular Disease. Can J Cardiol. 2023.
Elarbed A, Fackrell K, Baguley DM, Hoare DJ. Tinnitus and stress in adults: a scoping review. Int J Audio. 2021;60:171–82.
Al-Mana D, Ceranic B, Djahanbakhch O, Luxon LM. Hormones and the auditory system: a review of physiology and pathophysiology. Neuroscience. 2008;153:881–900.
Neri S, Signorelli S, Pulvirenti D, Mauceri B, Cilio D, Bordonaro F, et al. Oxidative stress, nitric oxide, endothelial dysfunction and tinnitus. Free Radic Res. 2006;40:615–8.
Langenbach M, Olderog M, Michel O, Albus C, Kohle K. Psychosocial and personality predictors of tinnitus-related distress. Gen Hosp Psychiatry. 2005;27:73–7.
Wallhausser-Franke E, Schredl M, Delb W. Tinnitus and insomnia: is hyperarousal the common denominator? Sleep Med Rev. 2013;17:65–74.
Probst T, Pryss RC, Langguth B, Rauschecker JP, Schobel J, Reichert M, et al. Does Tinnitus Depend on Time-of-Day? An Ecological Momentary Assessment Study with the “TrackYourTinnitus” Application. Front Aging Neurosci. 2017;9:253.
Acknowledgements
We are indebted to the study participants and all co-workers of the Gutenberg Health Study.
Funding
The GHS is funded through the government of Rhineland-Palatinate (“Stiftung Rheinland-Pfalz für Innovation”, contract AZ 961-386261/733), the research programs “Wissen schafft Zukunft” and “Center for Translational Vascular Biology (CTVB)” of the Johannes Gutenberg-University of Mainz, and its contract with Boehringer Ingelheim and PHILIPS Medical Systems, including an unrestricted grant for the GHS and by the Foundation Heart of Mainz. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript. Omar Hahad is a Young Scientist and Philipp Wild and Thomas Münzel are PI´s of the DZHK (German Center for Cardiovascular Research), Partner Site Rhine-Main, Mainz, Germany. Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
OH and JD designed the present research. KK-B performed the statistical analysis. OH drafted the manuscript. All authors were involved in the interpretation of the results and the critical review of the manuscript. All gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical approval
All procedures conducted in the GHS were approved by the ethics committee of the Statutory Physician Board of the State Rhineland-Palatinate [reference number 837.020.07(5555)] and the local data safety commissioners and were in line with the ethical principles for medical research involving human subjects as outlined in the Declaration of Helsinki. Before inclusion in the study, written informed consent was obtained from each participant.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Hahad, O., Döge, J., Bahr-Hamm, K. et al. Noise annoyance due to different sources is associated with tinnitus presence and distress in the general population. J Expo Sci Environ Epidemiol (2024). https://doi.org/10.1038/s41370-024-00668-9
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41370-024-00668-9
