
Abstract
In Brazil, similar intrauterine growth restriction (IUGR) rates were observed between cities with distinct levels of socioeconomic development, challenging the current knowledge that higher rates of IUGR would necessarily be observed in poorer areas than in wealthier ones. Ribeirão Preto, a city located in the most developed area in Brazil, showed an IUGR rate of 18% in 1994, whereas this rate was 18.5% in 1997/1998 in São Luís, located in one of the poorest areas in the country. The objective of this study was to compare risk factors for IUGR in these two cities and to identify factors that are responsible for this unexpected lack of difference between the rates. Using data from two birth cohorts, including 2839 neonates who were from Ribeirão Preto and born in 1994 and 2439 neonates who were from São Luís and born in 1997/1998, a multivariable analysis was conducted to assess changes in the risk for IUGR in the poorer city compared with the wealthier one in a combined model, adjusting for some risk factors for IUGR. The wealthier city showed higher rates of maternal smoking, attendance in the private sector, and obstetric interventions than the less developed one. Differences in maternal smoking and obstetric interventions were possibly responsible for the similarity of the rates between cities. It seems that early detection of IUGR followed by cesarean section in the wealthier city is associated with increased low birth weight and IUGR rates but reduced stillbirth and infant mortality rates.
Similar content being viewed by others


Main
Intrauterine growth restriction (IUGR), which predisposes the child to metabolic disturbances during the neonatal period and to alterations in somatic and neurocognitive development during childhood (1,2), is one of the main public health problems in developing countries. It is also responsible for diseases that affect adults, such as cardiovascular disorders, hypertension, and non–insulin-dependent diabetes (3,4). The IUGR rate in developing countries is six times higher than in developed ones, and it is estimated that 23.8% of all newborn infants, ∼30 million, are born with IUGR every year worldwide (5).
Various social, cultural, and environmental factors, which vary between developed and developing countries, affect intrauterine growth. In developed countries, cigarette smoking accounts for 25% of the cases; in addition, low weight gain, low body mass index, primiparity, and short stature are responsible for nearly half of the cases. In contrast, in developing countries, the contribution of cigarette smoking is lower, whereas the other causes increase considerably (6). However, little information is available about what factors may be implicated in differences in IUGR rates between wealthy and poor settings.
In Brazil, similar IUGR rates were observed between cities with distinct levels of socioeconomic development, challenging the current knowledge that higher rates of IUGR would necessarily be observed in poorer areas than in wealthier ones (7). Ribeirão Preto, a city located in the most developed area in Brazil, showed an IUGR rate of 18% in 1994, whereas this rate was 18.5% in 1997/1998 in São Luís, located in one of the poorest areas in the country. The purpose of this study was to compare risk factors that are associated with IUGR between these two cities using data from two birth cohorts and to identify factors that are responsible for the unexpected lack of difference between rates.
METHODS
Study area.
Ribeirão Preto is located in the state of São Paulo, southeast of Brazil, one of the richest and most industrialized regions of the country, with a population of 461,427 inhabitants in 1994 (8). Its human development index was 0.855 in 2000, occupying the sixth place in the São Paulo ranking and the 22nd place in the national ranking (9). São Luís, the capital of Maranhão State, has a population of 781,068 inhabitants (10) and is located in the northeast of Brazil, one of the poorest regions in the country. Its human development index was 0.778 in 2000, occupying the first place in the Maranhão ranking but the 1112th place in the national ranking (9). The per capita income of Ribeirão Preto is twice as high as that of São Luís.
Ribeirão Preto sample.
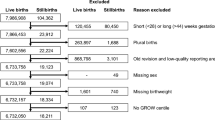
All maternity hospitals in the city participated in the survey. Data included all births over a period of 4 consecutive months from March to August 1994. Considering a maximum product of p × q (event proportion of 50%) and establishing the minimum significant difference at 4%, the minimum sample size was 2499 births. Excluding newborns of unknown birth weight and multiple deliveries, the total sample consisted of 2839 newborns. This sampling was based on a previous study that did not show seasonality in births along the year in terms of the variables studied: birth weight, preterm birth (PTB), maternal age, and twinning (8).
São Luís sample.
The data were collected between March 1997 and February 1998. Sampling, performed in a random manner, was stratified by maternity hospital, with the share being proportional to the number of deliveries. Systematic sampling was carried out at each maternity hospital on the basis of the birth list by order of occurrence, with a sampling interval of seven. Sample size calculations were based on the same assumptions as used for Ribeirão Preto. A total of 2439 newborns were selected, excluding multiple births, stillbirths, and newborns of unknown birth weight.
Common procedures applied in the two studies.
The samples of the two cities only comprised hospital deliveries, which corresponded to 96% of all births in São Luís and to 98% in Ribeirão Preto, with only mothers living in the municipalities being included. A similar method for data collection was used in the two studies.
The mothers were interviewed during their hospital stay or at home in cases of early discharge, which caused some losses. At the end of the study, the loss was 3.2% for Ribeirão Preto and 5.8% for São Luís.
The newborn infants were weighed without clothing soon after birth on an electronic scale or an infant-type scale, with a precision of 5 and 10 g, respectively, calibrated weekly by the research teams. Two trained staff members measured length at birth with the infant laid in the supine position on a neonatometer with a fixed vertical headpiece and a smooth sliding vertical footpiece. The first measurer kept the head in line with the body and fixed against the headpiece; the other measurer stretched the legs and touched the heels with the sliding footpiece. Measurements were made to the nearest 0.5 cm (11).
Gestational age was calculated for both cohorts on he basis of the date of the last normal menstrual period reported by the mother. For Ribeirão Preto, this date was classified as unknown when not recalled by the mother. In São Luís, day 15 was adopted for cases in which only the month of the last menstruation was known. In the two studies, cases of birth weight incompatible with the date of the last menstruation (identified using the cutoff points suggested by Altman and Coles based on English reference data) (12) or newborns with an unlikely gestational age (<20 or >50 wk) had their gestational age reclassified as unknown. There were 553 cases for which gestational age was missing in Ribeirão Preto and 120 cases in São Luís. All cases with missing or ignored gestational age were imputed in a regression model (13). The characteristics that were used to impute gestational age were birth weight, parity, family income, and newborn sex. Fifty-six cases were imputed as preterm in Ribeirão Preto and five in São Luís.
The concept of IUGR was based on the birth weight ratio (BWR), which is the ratio between the newborn's weight and the mean weight for gestational age of the sex-specific reference curve (14). A BWR ≥0.85 was defined as no growth restriction, and a BWR <0.85 was defined as IUGR (15).
Newborns were classified as large for gestational age, appropriate for gestational age, and small for gestational age when their birth weight was, respectively, above the 90th percentile, between the 90th and 10th percentiles, and less than the 10th percentile of the weight for gestational age from the curve of Williams et al. (14).
For the determination of body proportionality, Rohrer's ponderal index, defined as 100 times the weight in grams divided by the cube of the height in centimeters (16), was used. Newborns who had IUGR and whose ponderal index was below the 10th percentile of the reference value were considered to be asymmetric (17). The following variables were studied: newborn sex, number of cigarettes smoked by the mother per day during pregnancy (none, one to 10, or >10), maternal age (<18, 18–19, 20–34, or 35 y or more), marital status (married, cohabiting, or without a partner), maternal schooling (0–4, 5–11, or 12 y or more), parity (one, two to four, or five or more children), category of hospitalization (public or private), type of delivery [normal or cesarean section (CS)], and family income (expressed as multiples of the minimum wage: one or fewer, one to three, or more than three minimum wages). Adequate prenatal care use was determined using an index created on the basis of the minimum number of prenatal visits recommended by the Brazilian Ministry of Health (18). This variable was adjusted for the duration of pregnancy to prevent bias, because mothers of preterm infants tend to attend fewer prenatal visits, and classified into three categories: no prenatal care use, adequate prenatal care use, and inadequate prenatal care use. A missing category was added for all variables with missing information.
The study was approved by the Ethics Committees of the Maternal-Infant University Hospital of São Luís and the Ribeirão Preto Hospitals, and the mothers gave written informed consent to participate in the study before the interview.
The data were analyzed using the Stata program, version 6.0 (19). The χ2 test was used to compare proportions, and the odds ratio (OR) and its confidence interval (CI) were calculated to determine the effect of each variable on IUGR. For multivariable analysis, a stepwise logistic multiple regression model with backward elimination was used to control for confounding factors. Variables with p < 0.20 upon univariable analysis entered the analysis, and those with p < 0.10 remained in the model. We also assessed in a combined model that included both cities changes in the OR for an indicator variable (city of study). A crude OR for city was estimated and compared with adjusted ORs for city of study, including variables that were associated with IUGR in at least one of the cities. These variables were included one at a time and were retained in the model when they changed the OR for city of study by >10%. The level of significance was set at 5% (p < 0.05).
RESULTS
There were significant socioeconomic differences between the two cities (Table 1). São Luís showed various disadvantages: 32.3% of the families had an income equal to or lower than one minimum wage, only 4.9% of the mothers had ≥12 y of schooling, most births occurred in public hospitals (89.0%), and the percentage of mothers without a partner was almost double that observed in Ribeirão Preto. In contrast, in Ribeirão Preto, the family income was equal to or lower than one minimum wage in only 8.3% of cases, 13.0% of the mothers had ≥12 y of schooling, and 59.7% of births occurred in public hospitals.
Other disadvantages observed for São Luís were the elevated number of adolescent mothers (29.4%) and the larger number of mothers who did not receive prenatal care. However, Ribeirão Preto showed an almost four times higher incidence of smoking mothers and a higher rate of CS (50.9%).
Mean birth weight was higher in the São Luís sample than in the Ribeirão Preto sample (3177 versus 3113 g; p < 0.001). The same was observed for the mean birth weight of newborns with IUGR (2580 versus 2443 g; p < 0.001).
The BWR identified a similar number of infants with IUGR (Table 2): 18.0% in Ribeirão Preto and 18.5% in São Luís (p = 0.649). The prevalence of preterm newborns was the same in the two cohorts (12.6%). However, the prevalence of low birth weight (LBW) was higher in Ribeirão Preto than in São Luís (10.7 versus 7.6%). Ribeirão Preto had a lower stillbirth rate (9.6 per 1000 in 1994 versus 19.1 per 1000; p < 0.001 in 1997/1998) and lower infant mortality than São Luís (16.6 per 1000 versus 26.2 per 1000; p = 0.014).
The percentage of PTB among growth-restricted infants was higher in the wealthier city (20.4 versus 7.8%; p < 0.001). Moreover, the percentage of asymmetric newborns among those with IUGR was higher in São Luís than in Ribeirão Preto (13.7 versus 8.6%; p = 0.013). This difference was still higher among preterm newborns (18.8 versus 9.5%; p < 0.001).
For the São Luís sample, univariable analysis (Table 3) revealed an association between IUGR and maternal age, maternal schooling, family income, marital status, number of cigarettes smoked, parity, and hospitalization category. In Ribeirão Preto, IUGR was associated with maternal schooling, family income, marital status, maternal number of cigarettes smoked, lack of prenatal care, and hospitalization category.
In the adjusted models, the following variables remained as risk factors for IUGR in São Luís: family income of more than one minimum wage and of three minimum wages or less, hospitalization in a public hospital, primiparity, and smoking >10 cigarettes per day. In Ribeirão Preto, risk factors were maternal schooling of 0–4 and 5–11 y, hospitalization at a public hospital, and smoking one to 10 and >10 cigarettes per day (Table 4). To test whether co-linearity between socioeconomic variables might have affected results because in the final model family income was retained for São Luís and maternal schooling was retained for Ribeirão Preto, models that included only family income or only maternal schooling were tested but produced similar results.
The prevalence of only 5.7% of smoking mothers found in São Luís contrasted with that observed in Ribeirão Preto, which was 17.0% (p < 0.001). However, the risk for IUGR for mothers who smoked >10 cigarettes per day was higher in São Luís than in Ribeirão Preto (4.94 versus 2.27).
Taking Ribeirão Preto as reference, the crude risk for IUGR for São Luís was similar (OR = 1.03, 95% CI 0.90–1.19). Adjustment for number of cigarettes smoked changed the OR to 1.18 (95% CI, 1.02–1.37). When adjusted for category of hospitalization, the OR changed to 0.88 (95% CI, 0.76–1.01). Adjusting for maternal schooling, family income and parity did not change the OR. Simultaneous adjustment for number of cigarettes smoked and category of hospitalization led to an OR of 1.02 (95% CI, 0.88–1.20).
DISCUSSION
In contrast to what was expected, the wealthier city was not at an advantage in terms of IUGR compared with the poorer city. However, stillbirths and infant mortality rates do differ in favor of the wealthier city. Differences in maternal smoking and obstetric interventions were possibly responsible for the similarity of the rates between the cities.
One of the factors that were responsible for the similarity of the IUGR rates was maternal smoking. The wealthier city showed a higher prevalence of maternal smoking than the less developed one. In a combined model, when adjustment for the number of cigarettes smoked was performed, the decreased OR suggested that if the rate of maternal smoking had been similar in the two cities, then the risk of IUGR would have been higher in the poorer city. Frisbie et al. (20), studying IUGR in different ethnic groups of the American population, obtained equally paradoxical results: although belonging to a demographic and socioeconomic group of high risk, white mothers of Hispanic origin showed an incidence of IUGR similar to that of white mothers of non-Hispanic origin. One of the factors that they thought could explain these findings was lower cigarette consumption among white mothers of Hispanic origin, in agreement with the present results.
Another factor that probably is associated with this paradox is obstetric intervention. The higher rate of IUGR among mothers attended in the private sector in the wealthier city was possibly a consequence of early detection of maternal pathology and consequent early interruption of pregnancy. Better perinatal care in the wealthier city may be rescuing some fetuses who otherwise would be stillborn. Further support for this hypothesis is that in the combined model, when adjustment for category of hospitalization was made, the OR decreased, suggesting that if mothers had received the same rate of attendance in the private sector in the two cities, then the IUGR rate would have been higher in the wealthier city.
In the separate models, risk for IUGR related to category of hospitalization (public versus private) was adjusted for socioeconomic indicators. Consequently, this adjusted risk might reflect quality of care. Differences in the risk for IUGR between mothers who delivered in the private and in the public sectors were higher for the poorer city. The increased risk for IUGR among mothers in the private sector in the wealthier city compared with mothers in the poorer city, instead of representing a worsening, probably reflects an improvement in the quality of care, because it was associated with better obstetric and neonatal outcomes. Stillbirth and infant mortality rates differ in favor of the wealthier city.
LBW rate was higher in Ribeirão Preto than in São Luís. The CS rate was also higher in Ribeirão Preto (50.8%) (21) than in São Luís (33.7%; p < 0.001) (10). It seems that early detection of IUGR followed by CS in the wealthier city was associated with increasing LBW and IUGR rate but also with a reduction in stillbirths and infant mortality. Others have also shown that obstetric intervention in preterm gestations, when correctly indicated, can help prevent stillbirths and infant mortality (22).
The size effect of socioeconomic factors in Ribeirão Preto was greater than in São Luís, possibly also reflecting higher rates of obstetric interventions among wealthier mothers. Not only were IUGR rates similar for the poorer and the wealthier city, but also IUGR rate increased in the wealthier city from 15.5% in 1978/1979 to 18.0% in 1994 (p = 0.003) despite improvements in various socioeconomic indicators and some known risk factors for IUGR over the same time. For example, the percentage of smoking mothers decreased from 28.9 to 21.4% (p < 0.001) (23). This is in contrast to what has been reported by others, who have shown decreasing IUGR rates in Canada (24).
In the wealthier city, when 1978/1979 data were compared with 1994 data, the PTB rate increased from 7.6 to 13.6% (p < 0.001) (25). The CS rate also rose from 30.3 to 50.8% (p < 0.001) (21). However, the infant mortality rate dropped from 36.6 per 1000 to 16.9 per 1000 (p < 0.001) (26) and the stillbirth rate also fell from 22.0/1000 stillbirths in 1978/1979 to 9.6/1000 in 1994 (27). In the wealthier city, increasing PTB, IUGR, and LBW rates but decreasing stillbirth and infant mortality rates over time further add to the evidence that increasing obstetric interventions, especially CS, might be associated with these trends.
We observed a predominance of symmetric IUGR in the two cities, in agreement with Tavares (28) and De Onis et al. (5), who also found a predominance of symmetric IUGR. The rate of asymmetric IUGR was lower and the percentage of PTBs among growth-restricted infants was higher in the wealthier than in the poorer city, further adding to the evidence of a higher rate of obstetric intervention in the wealthier city.
Although Ferraz et al. (29), analyzing another Brazilian childbearing population in the late 1980s, found an association between inadequate prenatal care use and IUGR, we did not observe such association. It is possible that increasing rates of poor neonatal outcomes (LBW, PTB, and IUGR) among women who adequately used prenatal care might be causing a bias by reducing the estimates of the effect of inadequate prenatal care use on poor neonatal outcomes (18). Conversely, CS rate probably could not explain this lack of difference in IUGR rates between the poorer and the wealthier city because of its increasing rates among better-off women in both cities, which might be reflecting both abusive and correctly indicated interventions (10,23). We were not able to differentiate between abusive and correct indications for CS, because we did not have data on this topic.
Underregistration of livebirths was higher in the poorer than in the wealthier city (30), a fact that may have produced a slight underestimation of IUGR in the poorer city. However, because this difference was small, it might have caused no substantial bias. We were unable to include other variables that have reported as being associated with IUGR in the literature, such as weight gain during pregnancy and maternal height and body mass index in our study. Likewise, pregnancy hypertension and other maternal pathologies were not analyzed because the study was not designed for this purpose. The main strength of the present investigation resides in its population-based approach, because the samples were representative of all deliveries that occurred in Ribeirão Preto in 1994 and in São Luís in 1997/1998. Comparing data from two populations with marked socioeconomic and health service contrasts permitted an easier detection of differences in risk factors for IUGR. In addition, our investigation is an important contribution to the study of IUGR in Brazil, where population studies are scarce, especially in the Northeast region, because of difficulties in determining gestational age.
CONCLUSION
In conclusion, the factors that are associated with IUGR seem to differ between richer and poorer regions, suggesting that causal factors act differently within the same country. Measures to reduce the incidence of IUGR should include the establishment of public policies that are properly directed at decreasing smoking during pregnancy. It seems that obstetric interventions in preterm gestations, when correctly indicated, can help to prevent stillbirths and infant mortality despite an increase in IUGR rate.
Abbreviations
- BWR:
-
birth weight ratio
- CI:
-
confidence interval
- CS:
-
cesarean section
- IUGR:
-
intrauterine growth restriction
- LBW:
-
low birth weight
- OR:
-
odds ratio
- PTB:
-
preterm birth
References
Ashworth A 1998 Effects of intrauterine growth retardation on mortality and morbidity in infants and young children. Eur J Clin Nutr 52( suppl 1): S34–S42
Leitner Y, Valevski FA, Geva R, Bassan H, Posner E, Kutai M, Many A, Jaffa AJ, Harel S 2000 Six year follow-up of children with intrauterine growth retardation: long-term, prospective study. J Child Neurol 15: 781–786
Barker DJ 1995 Fetal origins of coronary heart disease. BMJ 311: 171–174
Rosenfeld RG 1997 Intrauterine growth retardation: our current understanding and future directions. Acta Paediatr Suppl 423: 216–217
de Onis M, Blossner M, Villar J 1998 Levels and patterns of intrauterine growth retardation in developing countries. Eur J Clin Nutr 52( suppl 1): S5–S15
Kramer MS, Séguin L, Lydon J, Goulet L 2000 Socio-economic disparities in pregnancy outcome: why do the poor fare so poorly?. Paediatr Perinat Epidemiol 14: 194–210
Silva AA, Bettiol H, Barbieri MA, Ribeiro VS, Aragão VMF, Brito LGO, Pereira MM 2003 Infant mortality and low birth weight in cities of Northeastern and Southeastern Brazil. Rev Saúde Pública 37: 693–698
Bettiol H, Barbieri MA, Gomes UA, Andrea M, Goldani MZ, Ribeiro ERO 1998 [Perinatal health: methodology and some characteristics of the population studied]. Rev Saúde Pública 32: 18–28
HDI-Human Development Index 2000. Available: http://www.frigoletto.com.br/GeoEcon/idhma.htm
Silva AA, Lamy-Filho F, Alves MT, Coimbra LC, Bettiol H, Barbieri MA 2001 Risk factors for low birthweight in north-east Brazil: the role of caesarean section. Paediatr Perinat Epidemiol 15: 257–264
Davies DP, Holding RE 1972 Neonatometer: a new infant length measurer. Arch Dis Child 47: 938–940
Altman DG, Coles EC 1980 Nomograms for precise determination of birthweight for dates. Br J Obstet Gynecol 87: 81–86
Rubin DB 1987 Multiple Imputation for Nonresponse in Surveys. John Wiley & Sons, New York, pp 15–26
Williams RL, Creasy RK, Cunningham GC, Hawes WE, Norris FD, Tashiro M 1982 Fetal growth and perinatal viability in California. Obstet Gynecol 59: 624–632
Kramer MS, Platt R, Yang H, MacNamara H, Uscher RH 1999 Are all growth-restricted newborns created equally?. Pediatrics 103: 599–602
Miller HC, Hassanein K 1971 Diagnosis of impaired fetal growth in newborn infants. Pediatrics 48: 511–522
Lubchenko LO, Hansman C, Boyd E 1966 Intrauterine growth in length and head circumference as estimated from live births at gestational ages from 26 to 42 weeks. Pediatrics 37: 403–408
Goldani MZ, Barbieri MA, Silva AA, Bettiol H 2004 Trends in prenatal care use and low birthweight in Southeast Brazil. Am J Public Health 94: 1366–1371
Stata Corporation 1999 Stata Reference Manual: Release 6.0—User's Guide. Stata Corp., College Station, TX, pp 327–341
Frisbie WP, Biegler M, de Turk P, Forbes D, Pullum SG 1997 Racial and ethic differences in determinants of intrauterine growth retardation and other compromised birth outcomes. Am J Public Health 87: 1977–1983
Gomes UA, Silva AA, Bettiol H, Barbieri MA 1999 Risk factors for the increasing caesarean section rate in Southeast Brazil: a comparison of two birth cohorts, 1978–1979 and 1994. Int J Epidemiol 28: 687–694
Joseph KS, Demissie K, Kramer MS 2002 Obstetric intervention, stillbirth and preterm birth. Semin Perinatol 26: 250–259
Silva AA, Barbieri MA, Gomes UA, Bettiol H 1998 Trends in low birthweight: a comparison of two birth cohorts separated by a 15-year interval in Ribeirão Preto, Brazil. Bull World Health Organ 76: 73–84
Wen SW, Kramer MS, Platt R, Demissie K, Joseph KS, Liu S, Sauve R 2003 Secular trends of fetal growth in Canada, 1981 to 1997. Paediatr Perinat Epidemiol 17: 347–354
Bettiol H, Rona RJ, Chinn S, Goldani M, Barbieri MA 2000 Factors associated with preterm births in Southeast Brazil: a comparison of two birth cohorts born 15 years apart. Paediatr Perinat Epidemiol 14: 30–38
Goldani MZ, Barbieri MA, Rona RJ, Da Silva AA, Bettiol H 2004 Increasing pre-term and low-birth-weight rates over time and their impact on infant mortality in South-East Brazil. J Biosoc Sci 36: 177–188
Silva AA, Barbieri MA, Bettiol H, Goldani MZ, Rona RJ 2004 Can we explain why Brazilian babies are becoming lighter?. Int J Epidemiol 33: 821–828
Tavares RF 1998 [The study of intrauterine growth of normal newborn infants]. J Pediatr (Rio J) 74: 205–212
Ferraz EM, Gray RH, Cunha TM 1990 Determinants of preterm delivery and intrauterine growth retardation in North-East Brazil. Int J Epidemiol 19: 101–108
Silva AA, Ribeiro VS, Borba AF Jr, Coimbra LC, Silva RA 2001 Evaluation of data quality from the Information System on Live Births in 1997–1998. Rev Saúde Pública 35: 508–514
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported by CNPq (Brazilian National Research Council grants 523474/96-2 and 520664/98-1) and FAPESP (São Paulo Research Council grant 93/0525-0).
Rights and permissions
About this article
Cite this article
De Farias Aragão, V., Barbieri, M., Moura Da Silva, A. et al. Risk Factors for Intrauterine Growth Restriction: A Comparison between Two Brazilian Cities. Pediatr Res 57, 674–679 (2005). https://doi.org/10.1203/01.PDR.0000156504.29809.26
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/01.PDR.0000156504.29809.26
This article is cited by
-
Association between preterm births and socioeconomic development: analysis of national data
BMC Public Health (2022)
-
Passive smoking as a risk factor of anemia in young children aged 0–35 months in Jordan
BMC Pediatrics (2007)
