
Abstract
To determine whether human milk contained soluble receptors and cytokine antagonists that might contribute to its anti-inflammatory properties, ELISA and enzyme-amplified sensitivity immunoassay methods were used to quantitate soluble intercellular and vascular cell adhesion molecules, soluble E-selectin, soluble IL-6 receptor, IL-1 receptor antagonist, and soluble tumor necrosis factor-α (TNF-α) receptors I and II in human milk and colostrum. Soluble adhesion receptors (soluble intercellular and vascular cell adhesion molecules and soluble E-selectin) were present in colostrum at levels approximately equal to serum, whereas milk levels were significantly lower. Both colostrum and milk contained soluble IL-6 receptor, but the levels present were significantly lower than that reported for serum. The colostrum contents of IL-1 receptor antagonist (672 ± 202 pg/mL), TNF-α receptor I (>3703 ± 305 pg/mL), and TNF-α receptor II(>4507 ± 770 pg/mL) were significantly elevated over serum/plasma levels. Milk levels of IL-1 receptor antagonist and TNF-α receptor I were also greater than serum/plasma levels, but lower than colostrum levels. Examination of sequential milk specimens collected from seven women over a period of 2-6 mo showed that IL-1 receptor antagonist and TNF-α receptors I and II persisted throughout lactation. Column chromatographic fractionation of colostrum and milk demonstrated that soluble TNF-α receptors I and II had molecular sizes up to 60 kD, suggesting that they might be associated with other molecules. Antigen assays for TNF-α in colostrum and milk, as well as chromatographic fractionation experiments, showed that, although present, most TNF-α was not “free” in colostrum or milk, consistent with the observed content of soluble TNF-α receptors I and II. These studies demonstrate that human milk and colostrum contain soluble receptors and cytokine antagonists, materials which could contribute to their anti-inflammatory properties.
Similar content being viewed by others


Main
Human milk contains a variety of components that potentially exert anti-inflammatory effects(1–3). Experimentally, human colostrum alters inflammatory cell function via effects on reactive oxygen metabolites(4–6) by suppression of lysosomal enzyme activity(4) and by alteration of adherence(6, 7), movement(7), and suppression of bactericidal activity(6). Human milk suppresses leukocyte adherence and movement(7), suppresses lymphocyte production of IL-2(8), and blocks selected lymphocyte surface antigens(9). Although colostrum contains the proinflammatory cytokine TNF-α(10), it also contains the anti-inflammatory cytokine IL-10(11). Milk contains soluble globotriaosylceramide, the receptor for Shiga toxin and Shiga-like toxin(12), and fucosylated oligosaccharides that block the action of heat-stable enterotoxin of Escherichia coli(13), the binding of Campylobacter pylori(14) to intestinal epithelium, and adherence mechanisms of other microorganisms(15). In animals, colostrum exerts potent anti-inflammatory activity in a subcutaneous air pouch model(16). In some countries, colostrum is instilled topically into the eyes of newborn infants, where it markedly decreases the incidence of “sticky eyes” and conjunctivitis(17).
It is increasingly clear that receptor-mediated events are important in the evolution of the inflammatory response(18, 19). Interaction of inflammatory cells with vascular endothelium and of proinflammatory cytokines with their cellular receptors occurs early in inflammation, and blockade of either results in anti-inflammatory effects(20–22). We hypothesized that human milk might derive some of its anti-inflammatory effects via alteration of receptor-mediated events involved in inflammation. The objective of this study was to determine whether human colostrum/milk contained soluble receptors or cytokine antagonists that could contribute to its anti-inflammatory character.
METHODS
ELISAs for sICAM-1, sVCAM-1, sE-SELECTIN, sIL-6R, IL-1RA, sTNF RI, sTNF RII, and TNF- α ELISAs for sICAM, soluble sVCAM, sE-selectin, sIL-6R, sTNF RI, sTNF RII, and TNF-α were commercially available assays (R&D Systems, Minneapolis, MN). The sensitivities of these assays are in the picogram/mL range as reported by the manufacturer. The ability of this TNF-α ELISA to differentiate between free and bound antigen is not addressed by the manufacturer, but others have published that it recognizes only free TNF-α(23).
EASIAs for sTNF RI, sTNF RII, and TNF- α EASIA for sTNF RI, sTNF RII, and TNF-α, based upon multiple MAbs directed against distinct epitopes on the target antigen, were commercially available assays (Incstar Corp., Stillwater, MN). In control experiments, recovery of sTNF RI and sTNF RII added exogenously to colostrum ranged from 96 to 104%, whereas recovery of TNF-α added to colostrum or milk samples ranged from 86 to 181% (121 ± 10%, n = 10). According to the manufacturer, all of the EASIAs recognize antigens in toto (free plus bound). The advantages of using assays capable of recognizing totalversus free TNF-α antigen have been addressed by others(23, 24). In two experiments, the EASIA for sTNF-RI was modified, substituting anti-TNF-α-HRP (from the TNF-α EASIA) for anti-sTNF RI-HRP, to attempt ligand detection following capture of the soluble receptor.
Colostrum, milk, plasma, and serum samples. Random colostrum(≤4 d of lactation) and milk samples (referred to as random specimens) were obtained from volunteer donor mothers by breast pump (Medela Inc., McHenry, IL) and were typically processed within 2 h of collection. After ultracentrifugation (80,000 × g, 30 min, 4 °C), cell-free aqueous fractions were collected as previously described(4) and frozen at -70 °C until used. Colostrum and milk samples used for quantitation of soluble adhesion receptors were passed through 0.2-μm filters before assay to remove any membrane associated molecules. Specimens used for other assays were not filtered.
A separate set of 88 milk samples (referred to as longitudinal samples) obtained sequentially over 2-6 mo from seven mothers serving as controls in a prepartum vaccination study(25) were used to examine soluble receptor content over time. After collection, these samples were kept refrigerated until sedimented (10,000 × g, 20 min, 4 °C), then separated to produce acellular aqueous fractions which were frozen at -70°C until used.
Plasma samples were prepared from heparinized whole blood obtained from volunteer adult donors. After centrifugation at 400 × g for 10 min to sediment cellular elements, the plasma fractions were passed through 0.45-μm filters and frozen in aliquots at -70 °C for later testing.
Serum samples were prepared from whole blood obtained from volunteer adult donors. After clotting at room temperature for 30 min, each sample was“rimmed” with a wooden applicator, held at 4 °C for 45 min, and centrifuged, and the serum was frozen in aliquots at -70 °C until used.
Column chromatography. A 2.8 × 34-cm Sephadex G100 column was used to fractionate unconcentrated aqueous colostrum/milk using 0.2 M sodium phosphate (pH 7.5) as running buffer. The column was calibrated with bovine serum albumin (67 kD), HRP (44 kD), trypsin (24 kD), and lysozyme (14.4 kD). The column was run at 5 mL/h, and fractions (2.1 ml) were collected at 4°C and assayed for OD280 and sTNF RI, sTNF RII, and TNF-α by EASIA. For some fractions, the reagents and procedures for the sTNF RI and TNF-α EASIAs were combined to attempt capture of antigens with anti-receptor antibodies and detection with anti-TNF-α antibodies.
Use of human subjects. The use of human subjects in the studies described was approved by the Institutional Review Board of the Eastern Virginia medical School under consent IRB no. 05-06-92-0216.
Statistics. Data are presented as mean ± SEM values. Statistical comparisons are based on a t test or a paired samplet test if natural pairing occurred in the experimental series. Linear regression is used to examine relationships between groups of paired data. A probability of p < 0.05 is taken as statistically significant.
RESULTS
Soluble adhesion receptor content of human colostrum and milk. A range of soluble adhesion receptor concentrations were found in random samples of colostrum and milk. The mean concentration of sICAM in colostrum(184 ± 49 ng/mL, n = 16) was significantly higher than in mature milk (59 ± 11 ng/mL, n = 13, p < 0.05versus colostrum). Similarly, the concentration of sVCAM was higher in colostrum than mature milk (182 ± 49 ng/mL, n = 16versus 16 ± 2 ng/mL, n = 13, colostrumversus milk, p < 0.05). The concentrations of sE-selectin observed were at the limit of sensitivity for the ELISA used, but like sICAM and sVCAM, the concentration in colostrum was higher than in milk(1 ± 0.6 ng/mL, n = 16 versus 0.14 ± 0.04 ng/mL, n = 13, colostrum versus milk, p < 0.05). No relationships between the different adhesion receptor types within specimens of colostrum or milk were observed. Because the levels of soluble adhesion receptors found were similar to those reported for plasma and serum(26–28), the longitudinal samples were not examined for their content of these components.
Cytokine antagonist content of human colostrum and milk. The IL-1RA content of random samples of colostrum (collected at 2.5 ± 0.2 d), milk (collected at 223 ± 92 d) and plasma is shown inFigure 1A. Both colostrum and milk contained IL-1RA in comparable amounts: colostrum, 672 ± 202 pg/mL, n = 20; milk, 717 ± 248 pg/mL, n = 15. Six colostrum and six milk samples contained no IL-1RA. Three serum samples (239 ± 155 pg/mL) were also tested, and the range observed was similar to serum levels reported by others: approximately 200 pg/mL(29, 30). Results from longitudinal samples (collected at 72 ± 6 d) are shown inFigure 2A: the IL-1RA content of milk was 316 ± 70 pg/mL, n = 88, with the suggestion that levels were higher in early milk, then remained stable or decreased slightly as lactation continued.

(A-D) Levels of IL-1RA, sIL-6R, sTNF RI, and sTNF RII in standard colostrum and milk samples determined by ELISA. Bars denote mean values.

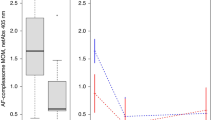
(A-D) Levels of IL-1RA, sIL-6R, sTNF RI, and sTNF RII in longitudinally collected milk samples, determined by ELISA (IL-1RA and sIL-6R) or EASIA (sTNF RI and sTNF RII).
Soluble cytokine receptor content of human milk. Three soluble proinflammatory cytokine receptors were examined: sIL-6R by ELISA, and sTNF RI and RII (the soluble forms of the p55 and p75 TNF receptors, respectively) by both ELISA and EASIA. Figure 1,B-D, shows the results of ELISAs examining random samples of colostrum and milk. The concentration of sIL-6R in colostrum (2.5 ± 0.2 d: 12761 ± 982 pg/mL, n= 22) was significantly higher than milk (223 ± 92 d: 2436 ± 580 pg/mL, n = 15, p < 0.05). Two serum samples examined for their sIL-6R content showed levels significantly higher than those in colostrum and milk (both p < 0.001), but consistent with reported levels of sIL-6R in serum/plasma (mean 80-110 ng/mL)(31, 32).
Colostrum (2.8 ± 0.2 d) levels of sTNF RI (3703 ± 305 pg/mL,n = 24) and sTNF RII (4507 ± 770 pg/mL, n = 25), and milk levels of sTNF RI (1732 ± 208 pg/mL, n = 18), but not sTNF RII (931 ± 104 pg/mL, n = 18), were significantly higher than those present in plasma (824 ± 82 pg/mL, n = 18 and 1518 ± 90 pg/mL, n = 19, respectively).
In longitudinal samples (72 ± 6 d), sIL-6R levels measured by ELISA were lower than in standard milk samples (longitudinal: 171 ± 20 pg/mL,n = 88 versus standard: 2436 ± 580 pg/mL,n = 15). The pattern across time suggested sIL-6R levels were higher in early milk, then decreased as lactation continued (Fig. 2B).
sTNF RI and sTNF RII levels, both measured by EASIA, showed a pattern of scatter across time without a downward trend (Fig. 2,C andD). sTNF RI levels were generally higher than sTNF RII. Longitudinal sample(collected at 64 ± 7 d) sTNF RI levels examined by EASIA were higher than those of standard milk samples (193 ± 61 d) measured by ELISA(3695 ± 487 pg/mL, n = 59 versus 1732 ± 208 pg/mL, n = 18), whereas sTNF RII levels were comparable(longitudinal: 1258 ± 198 pg/mL, n = 60, versus standard: 931 ± 104 pg/mL, n = 18).
TNF- α Content of human colostrum and milk. The presence of large amounts of sTNF RI and sTNF RII in colostrum and milk prompted us to measure the content of TNF-α in these specimens. Using only the EASIA, random colostrum specimens contained 46 ± 6 pg/mL(n = 12) of “total” TNF-α. Based on both EASIA and ELISA methods, the “total” TNF-α concentration in longitudinal specimens (Fig. 3) was 99 ± 20 pg/mL,n = 87, whereas ELISA-based measurements of “free” TNF-α showed 30-fold less TNF-α (3 ± 1 pg/mL, n = 79) (p < 0.05) in the same samples. This difference suggested that most of the contained TNF-α was “invisible” to the ELISA-based method, potentially by sequestration by soluble receptor.

TNF-α levels in longitudinally collected milk samples, determined by ELISA (free TNF-α) and by EASIA (total TNF-α).
To examine whether TNF-α was receptor-bound, column chromatography was performed to estimate the molecular size of TNF-α, sTNF RI and sTNF RII in colostrum and milk (Fig. 4). Both sTNF RI and sTNF RII were detected in colostrum and milk fraction nos. 31-40 representing molecular sizes of 24-67 kD, with peaks in fraction nos. 34-36 (44-50 kD). As the reported sizes of sTNF RI and sTNF RII (both about 30 kD)(33, 34) should have placed them into fraction nos. 37-39, this suggested that the effective size of these molecules was in the range of 40-60 kD. TNF-α (“total”) was detected only in fractions > no. 36, representing molecular sizes <44 kD. Trimeric TNF-α, the bioactive form, is 51 kD, which should have placed it in fraction nos. 32-34. These results suggested that TNF-α is not in a homotrimeric form in human colostrum/milk. Additionally, for all milk specimens examined by chromatography (n = 5), TNF-α was detected in fewer fractions and with lower signal intensities than in the two colostrum specimens tested.

Representative OD280 patterns from column chromatography fractionation of colostrum (above) and milk (below) using Sephadex G100. Molecular sizes are identified by dotted vertical lines. Below each OD280 curve are the results of EASIAs for sTNF RI, sTNF RII, and TNF-α on the fractions shown, with gray scale representation of signal intensity as defined to the right. Below the EASIA results are shown the results (±) of using anti-sTNF RI for antigen capture and anti-TNF-α for antigen detection on selected column fractions.
If antigenic TNF-α was associated with soluble receptors, this might explain the differences between “free” and “total” TNF-α in longitudinal specimens and the anomalous molecular sizes of TNF-α, sTNF RI and sTNF RII antigens in fractionated milk/colostrum. Therefore, single specimens of colostrum and milk were fractionated, and selected column fractions containing TNF-α and sTNF RI and RII were examined by “capturing” with antibody against sTNF RI and detecting with anti-TNF-α (Fig. 4). In colostrum fractions, TNF-α signal was detected in fractions of 24-44 kD captured with anti-sTNF RI, suggesting that monomeric TNF-α might be associated with sTNF RI. Applying the same approach to milk fractions, for reasons not readily apparent, TNF-α was detected in several milk fractions“captured” with anti-sTNF RI that originally were negative by the“total” TNF-α EASIA. Thus the question of whether TNF-α in colostrum and milk is sequestered in soluble receptor requires further examination.
DISCUSSION
Human milk is a complex biologic fluid that supplies both nutritional and“protective” factors to the breast-fed infant. Until recently, characterization of milk's protective factors centered on“classical” host defense components such as Ig, lactoferrin, and peroxidase. Presently, more attention has turned to the “novel” protective components now realized to be in human milk, such as receptor-mimic oligosaccharides, mucins, antioxidants, anti-inflammatory cytokines, and leukocyte-altering components. Our interests in the “novel” protective mechanisms and factors of colostrum/milk center on its anti-inflammatory characteristics(1–3). In pursuing possible mechanisms for these characteristics, we have found significant suppressive effects of colostrum on multiple human granulocyte functions(4–6) as well as anti-inflammatory effects in an animal model(16). Based upon recent studies that implicate soluble receptors and cytokine receptor antagonists as potent anti-inflammatory agents(35, 36), we sought to determine whether human colostrum and milk contained these biomolecules, what their content was, and whether they could contribute to the anti-inflammatory character of colostrum and milk.
As leukocyte adhesion is key to inflammatory cell accumulation at sites of infection or injury, and because both laboratory and clinical studies have shown that adhesion molecule blockade (either of the ligands themselves or their receptors) inhibits numerous inflammation-related events(37–42), we hypothesized that soluble adhesion molecules might be present in colostrum and milk. Three soluble adhesion molecules were found in colostrum in quantities similar to (sICAM and sVCAM) or less than (sE-selectin) those in human serum. The milk content of these molecules was lower than in colostrum, suggesting that soluble vascular adhesion molecules were unlikely to contribute significantly to milk's anti-inflammatory effects.
IL-1RA shares enough sequence homology with the proinflammatory cytokines IL-1α and IL-1β to include it as an IL-1 isoform. Unlike IL-1α and IL-1β, however, binding of IL-1RA to the IL-1 receptor does not transduce an IL-1 signal. Current evidence suggests that IL-1RA normally competes with IL-1α/IL-1β for receptor binding, and thus represents a control mechanism to modulate IL-1 physiologic effects(35). IL-1RA was present in standard colostrum and milk samples in amounts higher than reported in serum. When examined in longitudinally collected milk samples, IL-1RA levels were either stable or declined slightly, suggesting that the breast-fed infant continuously receives significant amounts of IL-1RA throughout the period of breast-feeding.
Unlike IL-1RA, IL-6 is a proinflammatory cytokine that shares many physiologic effects with IL-1β(43). The cell surface receptor for IL-6 is comprised of gp130, a non-IL-6-binding, signal-transducing component, and of IL-6R, and IL-6R-binding, nontransducing component. A soluble form of IL-6R can be produced by cell shedding and binds IL-6 with low affinity(44). When the sIL-6R/IL-6 complex forms in solution, it retains the ability to interact with surface gp130 and thus, to transduce the IL-6 signal. Therefore, binding of IL-6 to either soluble or surface IL-6R may lead to association with surface gp130 and initiate effects of the proinflammatory cytokine(44). For an anti-inflammatory effect, low levels of sIL-6R would be necessary, as we observed in both colostrum and milk. In longitudinally collected samples, sIL-6R values were 1-2% of the colostrum values, confirming that milk levels of sIL-6R are low under normal conditions.
TNF-α is a pleiotropic cytokine with many dose-related physiologic actions. In concert with IL-1β, TNF-α synergistically mediates proinflammatory effects via two cell surface receptors. Soluble forms of both receptors, sTNF RI and sTNF RII, can bind TNF-α and modulate its biologic effects(36). Both sTNF RI and sTNF RII were present in random colostrum samples, in amounts significantly greater than in plasma. Both were also present in random milk samples, but sTNF RII content was not different from the plasma content. Longitudinally collected milk samples contained high levels of TNF RI throughout the first 200 d of lactation, whereas TNF RII levels in these same samples approximated those of plasma.
The presence of large amounts of sTNF receptors in colostrum/milk prompted reexamination of the content of their ligand in colostrum/milk. Others had previously used a competitive RIA to determine that TNF-α was present in milk collected 24-48 h postpartum, noting that the observed levels (620± 183 pg/mL) were high enough to potentially mediate biologic effects(10). Because these biologic effects would likely be proinflammatory, and colostrum/milk are anti-inflammatory, the presence of TNF-α in milk is paradoxical. Using an ELISA that putatively detects only “free” TNF-α(23), we found that TNF-α levels in longitudinally collected milk samples were quite low. However, when EASIA methods that detect “total” TNF-α were applied to the same specimen set, approximately 30-fold more TNF-α was detected, suggesting that only a small percentage of TNF-α in these specimens was “free” and therefore, potentially active.
Column chromatography-based estimates of the molecular sizes of colostrum/milk TNF-α, sTNF RI, and sTNF RII were inconsistent with the reported sizes of these antigens. Variance in column chromatography-based estimates of the size of TNF-α and sTNF RI and RII have also been reported by others(45). In our studies, sTNF RI and RII had sizes of up to 60 kD, perhaps because the soluble receptor had other components associated with it. Antigenic “total” TNF-α was variably present in fractions ≤44 kD. On the basis of these experiments and the differences between the ELISA and EASIA measurements of TNF-α, we speculate that TNF-α in colostrum and milk may be associated with soluble receptor, which could neutralize the bioactivity of TNF-α. Experiments are currently underway to test this hypothesis.
In summary, we found that human colostrum and milk contain soluble vascular adhesion molecules in small quantities, IL-RA in significant quantities that appear to wane with ongoing lactation, low levels of sIL-6R, and significant levels of soluble TNF receptors. In addition, we confirmed earlier observations that TNF-α is present in colostrum and milk, but have determined that only a small fraction of this material is “free.” We interpret these observations as consistent with the proposed anti-inflammatory character of human milk and suggest that the soluble TNF receptors contribute to this character.
Abbreviations
- sICAM-1:
-
soluble intercellular adhesion molecule-1
- sVCAM-1:
-
soluble vascular cell adhesion molecule-1
- sE-selectin:
-
soluble E-selectin
- sIL-6R:
-
soluble IL-6 receptor
- TNF:
-
tumor necrosis factor
- sTNF RI:
-
soluble tumor necrosis factor-α receptor I
- sTNF RII:
-
soluble tumor necrosis factor-α receptor II
- IL-1RA:
-
IL-1 receptor antagonist
- EASIA:
-
enzyme-amplified sensitivity immunoassay
- HRP:
-
horseradish peroxidase
References
Goldman AS, Thorpe LW, Goldblum RM, Hanson LA 1986 Anti-inflammatory properties of human milk. Acta Paediatr Scand 75: 689–695
Goldman AS, Goldblum RM, Hanson LA 1990 Anti-inflammatory systems in human milk. Adv Exp Med Biol 262; 69–76
Goldman AS 1993 The immune system of human milk: antimicrobial, antiinflammatory and immunomodulating properties. Pediatr Infect Dis J 12: 664–672
Buescher ES, McIlheran SM 1988 Antioxidant properties of human colostrum. Pediatr Res 24: 14–19
Buescher ES, McIlheran SM, French RW 1989 Further characterization of human colostral antioxidants: identification of an ascorbate-like element as an anti-oxidant component and demonstration of anti-oxidant heterogeneity. Pediatr Res 25: 266–270
Buescher ES, McIlheran SM 1993 Polymorphonuclear leukocytes and human colostrum: effects of in vivo and in vitro exposure. J Pediatr Gastroenterol Nutr 17: 424–433
Thorpe LW, Rudloff HE, Powell LC, Goldman A 1986 Decreased response of human milk leukocytes to chemoattractant peptides. Pediatr Res 20: 373–377
Mandalapu P, Pabst HF, Paetkau V 1995 A novel immunosuppressive factor in human colostrum. Cell Immunol 162: 178–184
Newburg DS, Viscidi RP, Ruff A, Yolken RH 1992 A human milk factor inhibits binding of human immunodeficiency virus to the CD4 receptor. Pediatr Res 31: 22–28
Rudloff EH, Schmalsteig FC, Mushtaha AA, Palkowetz KH, Liu SK, GOldman A 1992 Tumor necrosis factor-α in human milk. Pediatr Res 31: 29–33
Garofalo R, Chheda S, Mei F, Palkowetz KH, Rudloff HE, Schmalsteig FC, Rassin DK, Goldman AS 1995 Interleukin-10 in human milk. Pediatr Res 37: 444–449
Newburg DS, Ashkenazi S, Cleary TG 1992 Human milk contains the shiga toxin and shiga-like toxin receptor glycolipid Gb3. J Infect Dis 166: 832–836
Newburg DS, Pickering LK, McCluer RH, Cleary TG 1990 Fucosylated oligosaccharides of human milk protect suckling mice from heat stable enterotoxin of Escherichia coli. J Infect Dis 162: 1075–1080
Emödy L, Carlsson A, Ljungh A, Wadström T 1988 Mannose-resistant haemagglutination by Campylobacter pylori. Scand J Infect Dis 20: 353–354
Kunz C, Rudloff S 1993 Biological functions of oligosaccharides in human milk. Acta Paediatr 82: 903–912
Murphey DK, Buescher ES 1993 Human colostrum has anti-inflammatory activity in rat subcutaneous air pouch model of inflammation. Pediatr Res 34: 208–212
Bishai D, Bishai M 1987 Gonococcal ophthalmia neonatorum. N Engl J Med 316: 1549
Dinarello CA, Gelfand JA, Wolff SM 1993 Anticytokine strategies in the treatment of systemic inflammatory response syndrome. JAMA 269: 1829–1835
Arai K, Lee F, Myajima A, Miyatake S, Arai N, Yokata T 1990 Cytokines: coordinators of immune and inflammatory responses. Annu Rev Biochem 59: 783–836
Rozdzinski E, Jones T, Burnette WJ, Burroughs M, Tuomanen E 1993 Antinflammatory effects in experimental meningitis of prokaryotic peptides that mimic selectins. J Infect Dis 168: 1422–1428
Thomas TK, Will PC, Srivastava A, Wilson CL, Harbison M, Little J, Chesonis RS, Pignatello M, Schmolze D, Symington J, Kilian PL, Thompson RC 1991 Evaluation of an interleukin-1 receptor antagonist in the rat acetic acid-induced colitis model. Agents Actions 34: 187–190
Martin D, Near SL, Bendele A, Russell DA 1995 Inhibition of tumor necrosis factor is protective against neurologic dysfunction after activ immunization of Lewis rats with myelin basic protein. Exp Neurol 131: 221–228
Hartung T, Döcke W-D, Gantner F, Krieger G, Sauer A, Stevens P, Volk H-D, Wendel A 1995 Effect of granulocyte colony stimulating factor treatment on ex vivo blood cytokine response in human volunteers. Blood 85: 2482–2489
Engelberts I, Stephens S, Francot GJM, van der Linden CJ, Buurman WA 1991 Evidence for different effects of soluble TNF-receptors on various TNF measurements in human biological fluids. Lancet 338: 515–516
Pickering LK, Marrow AL, Herrera I, O'Ryan M, Estes MK, Guillams SE, Jackson L, Carter-Campbell S, Matson DO 1995 Effect of maternal rotavirus immunization on milk and serum antibody titers. J Infect Dis 172: 723–728
Pall AA, Adu D, Drayson M, Taylor CM, Richards NT, Michael J 1994 Circulating soluble adhesion molecules in systemic vasculitis. Nephrol Dial Transplant 9: 770–774
Wenisch C, Varijanonta S, Looareesuwan S, Grainger W, Pichler R 1994 Soluble intercellular adhesion molecule-1 (ICAM-1), endothelial leukocyte adhesion molecule-1 (ELAM-1) and tumor necrosis factor receptor (55 kDa TNF-R) in patients with acute Plasmodium falciparum malaria. Clin Immunol Immunopathol 71: 334–348
Spronk PE, Bootsma H, Huitma MG, Limburg PC, Kallenberg CG 1994 Levels of soluble VCAM-1, soluble ICAM-1, and soluble E-selectin during disease exacerbations in patients with systemic lupus erythematosis(SLE); a long term prospective study. Clin Exp Immunol 97: 439–444
Khosla S, Peterson JM, Egan K, Jones JD, Riggs BL 1994 Circulating cytokine levels in osteoporotic and normal women. J Clin Endocrinol Metab 79: 707–711
Gabay C, Gay-Crosier F, Roux-Lombard P, Meyer O, Maineti C, Guerne PA, Vischer T, Dayer JM 1994 Elevated levels of interleukin-1 receptor antagonist in polymyositis/dermatomyositis. A biologic marker of disease activity with a possible role in the lack of acute-phase protein response. Arthritis Rheum 37: 1744–1751
Gaillard JP, Bataille R, Brailly H, Zuber C, Yasukawa K, Attal M, Maruo N, Taga T, Kishimoto T, Klein B 1993 Increased and highly stable levels of functional soluble interleukin-6 receptor in sera of patients with monoclonal gammopathy. Eur J Immunol 23: 820–824
Mitsuyama K, Toyonga A, Sasaki E, Ishida O, Ikelda H, Tsuruta O, Harada K, Tateishi H, Nishiyama T, Tanikawa K 1995 Soluble interleukin-6 G. ut 36: 45–49
Seckinger P, Isaaz S, Dayer M 1989 Purification and biologic characterization of a specific tumor necrosis factor inhibitor. J Biol Chem 264: 11966–11973
Engelmann H, Novick DN, Wallach D 1989 Two tumor necrosis factor binding proteins from human urine. Evidence for immunological cross-reactivity with cell surface tumor necrosis factor receptors. J Biol Chem 265: 1531–1536
Dinarello CA, Wolff SM 1993 The role of interleukin-1 in disease. N Engl J Med 328: 106–113
Hale KK, Smith CG, Baker SL, Vanderslice RW, Squires CH, Gleason TM, Tucker KK, Kohno T, Russel DA 1995 Multifunctional regulation of the biological effects of TNF- by the soluble type I and II receptors. Cytokine 7: 26–38
Pforte A, Schiessler A, Gais P, von Kress S, Beer B, Riethmuller G, Ziegler-Heitbrock HW 1993 Expression of the adhesion molecule ICAM-1 on alveolar machrophanges and in serum in extrinsic allergic alveolitis. Respiration 60: 221–226
Gearing AJH, Memingway I, Pigott R, Hughes J, Rees AJ, Cashman SJ 1992 Soluble forms of vascular adhesion molecules, E-selectin, ICAM-1, and VCAM-1: pathological significance. Ann NY Acad Sci 67: 324–331
Dore-Duffy P, Newman W, Balabanov R, Lisak RP, Mainolfi E, Rothlein R, Peterson M 1995 Circulating soluble adhesion proteins in cerebrospinal fluid and serum of patients with multiple sclerosis: correlation with clinical activity. Ann Neurol 37: 55–62
Janssen BA, Luqmani RA, Gordon C, Hemingway IH, Bacon PA, Gearing AJ, Emery P 1994 Correlation of blood levels of soluble vascular cell adhesion molecule-1 with disease activity in systemic lupus erythematosus and vasculitis. Br J Rheumatol 33: 1112–1116
Boehme MW, Werle E, Kommerell B, Raeth U 1994 Serum levels of adhesion molecules and thrombomodulin as indicators of vascular injury in severe Plasmodium falciparum malaria. Clin Invest 72: 598–603
Kuhns DB, Alvord WG, Gallin JI 1995 Increased circulating cytokines, cytokine antagonists and E-selectin after intravenous administration of endotoxin to humans. J Infect Dis 171: 145–152
Dinarello CA 1991 Interleukin-1 and interleukin-1 antagonism. Blood 77: 1627–1652
Müllberg J, Schooltink H, Stoyan T, Günther M, Graeve L, Buse G, Mackiewicz A, Heinrich PC, Rose-John S 1993 The soluble interleukin-6 receptor is generated by shedding. Eur J Immunol 223: 473–480
Pennica D, Kohr WJ, Fendly BM, Shire SJ, Raab HE, Borchardt PE, Lewis M, Goeddel DV 1992 Characterization of a recombinant extracellular domain of the type 1 tumor necrosis factor receptor: evidence for tumor necrosis factor-α induced receptor aggregation. Biochemistry 31: 1134–1141
Acknowledgements
The authors thank Rosa Lee Hewitt, R.N., Debra Oelberg, R.N., and Patti Lundy, R.N., for their efforts and persistence in collecting colostrum and milk samples, and thank Medela, Inc., for the use of the breast pump used to collect milk for these studies. In addition, we thank Larry K. Pickering, M.D., for supplying the longitudinally collected milk samples examined in these studies and Penney Koeppen for her technical assistance.
Author information
Authors and Affiliations
Additional information
Supported by National Institute of Child Health and Human Development Grant HD 13021-11.
Rights and permissions
About this article
Cite this article
Buescher, E., Malinowska, I. Soluble Receptors and Cytokine Antagonists in Human Milk. Pediatr Res 40, 839–844 (1996). https://doi.org/10.1203/00006450-199612000-00011
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199612000-00011
This article is cited by
-
Effect of Multi-Microbial Probiotic Formulation Bokashi on Pro- and Anti-Inflammatory Cytokines Profile in the Serum, Colostrum and Milk of Sows, and in a Culture of Polymorphonuclear Cells Isolated from Colostrum
Probiotics and Antimicrobial Proteins (2019)
-
The anti-inflammatory effect of milk and dairy products on periodontal cells: an in vitro approach
Clinical Oral Investigations (2019)
-
Oropharyngeal administration of colostrum to extremely low birth weight infants: theoretical perspectives
Journal of Perinatology (2009)
