
Abstract
Cryptorchidism is associated with histologic changes in the human testis apparent by 2 y of age. The mechanism accounting for these changes is still unknown. To clarify whether apoptosis plays a role in human cryptorchidism, we evaluated its occurrence in cryptorchid testes of 73 prepubertal boys, 43 of whom had received human chorionic gonadotropin (hCG) treatment. The histologic samples in our study included both scrotal and inguinal testes. Using anin situ apoptosis detection method, we were able to demonstrate that both interstitial cells and germ cells were affected and that the specific germ cells undergoing apoptosis were exclusively spermatogonia. Apoptosisin situ was further seen in both scrotal and inguinal testes; in scrotal testes the numbers of apoptotic spermatogonia were 170% of those seen in the cryptorchid testes (p < 0.05). Analysis of apoptotic DNA fragmentation from isolated DNA of a few selected biopsy samples served to validate our in situ findings. The amount of germ cell apoptosis analyzed during the 1st mo after hCG treatment was increased in both scrotal and inguinal testes compared with the amount before treatment (p< 0.001). But after the 1st mo it returned to the initial level, suggesting that hCG (and/or androgen) withdrawal increases germ cell apoptosis in the human testis. Our findings lead to the conclusion that apoptosis is a hormonally controlled, normal phenomenon in a human prepubertal testis and that cryptorchidism decreases its occurrence by reducing the number of germ cells capable of undergoing apoptosis.
Similar content being viewed by others


Main
The normal cycle of a cell includes growth, differentiation, and death. Death may occur by two different mechanisms: necrosis and apoptosis(1). In apoptosis, nuclear endonuclease cleaves the cell's DNA internucleosomally to form multimers of 180-200 bp, a precise phenomenon which has been largely accepted as the hallmark of apoptosis(2). Observations on the morphologic changes in the cell reveal nuclear and cytoplasmic condensation and breakage of the cell into several membrane-bound apoptotic bodies. These bodies are then rapidly phagocytosed by macrophages or by other neighboring cells. Apoptosis has been observed in many different tissues, both healthy and neoplastic. It typically involves single scattered cells and, because it progresses rapidly, it is difficult to observe(3). Apoptosis may be caused by noxious agents, but, unlike necrosis, it may also occur spontaneously or after a physiologic stimulus such as a surge or a withdrawal of a hormone(4).
The seminiferous epithelium of the testis is a rapidly proliferating tissue in which germ cells degenerate spontaneously. Up to 75% of the spermatogonia die before reaching maturity(5) and, interestingly, these dying cells display the internucleosomal cleavage typical of apoptosis(4, 6). In the testis, apoptotic cell death is hormonally controlled. Hypophysectomized immature rats display massive testicular apoptosis of both germinal and somatic cells which, however, can be inhibited by treatment with FSH or hCG(4). Therefore, in addition to the well known role of gonadotropins in stimulating testicular cell differentiation and growth, both FSH and LH, as well as testosterone(6), are able to prevent testicular apoptosis and act as testicular cell survival factors.
Cryptorchidism is the most common disorder in the sexual development of the male, its prevalence, decreasing slightly after birth, being 1.1% among 1-y-old boys(7). Cryptorchidism is known to cause histologic changes in the undescended testis. During the first 12 mo of life these changes cannot be distinguished by light microscopy. By 2 y, however, the germ cell count in an undescended testis has decreased, being significantly less than that in a normal testis(8). Patients with cryptorchid testes also possess smaller densities per unit volume of seminiferous tubules, have more interstitial bleeding (Kaleva M, Arsalo A, Louhimo I, Rapola J, Toppari J, Perheentupa J, Henriksen K, unpublished observations), and have interstitial fibrosis already demonstrable at 1 y of age(8). The exact mechanisms responsible for these changes in a cryptorchid testis are unclear. However, experimentally induced cryptorchidism in the rat causes testicular cell degeneration that is associated with apoptotic DNA fragmentation(9).
Various hormonal therapies have been advocated for the treatment of cryptorchidism, usually consisting of administration of hCG(10, 11) or GnRH agonists(12, 13) for several weeks. hCG has been known to induce some adverse effects in the cryptorchid testis, including inflammation-like changes, and to stimulate spermatogenesis and increase the diameter of the seminiferous tubules(14).
Using a technique for detecting apoptosis in situ, we investigated the occurrence of apoptosis in human prepubertal testes and the association of apoptosis with cryptorchidism. The in situ detection method enabled us to study the specific cells undergoing apoptosis in the human testis. The role of hCG in the control of testicular apoptosis and the effect of treatment age on the number of apoptotic cells were also evaluated.
METHODS
Subjects. The subjects of our study were 73 patients treated for cryptorchidism in the Children's Hospital, University of Helsinki, or in the Aurora Hospital, Helsinki, between 1975 and 1976. The localization of each cryptorchid testis was examined twice (at intervals of 2 wk) by one of us(A.A.). The testis was manipulated as low as possible first in a standing position, then in a half-sitting position to exclude saltatory testes from the study.
All 73 patients underwent surgery for the treatment of cryptorchidism. Before the surgical treatment, 43 patients had received unsuccessful hCG treatment, which consisted of 10 injections over a period of 5 wk. A single dose for patients less than 12 mo was 250 IU, for patients under 7 y old, 500 IU, and for patients over 7 y old, 1000 IU. Of these boys, 29 also had an inguinal hernia or hydrocele requiring surgery, and consequently they were operated on without prior hormonal treatment.
During the operation, a total of 102 testicular biopsies were obtained, of which 69 were from the group with prior hCG treatment and 31 were from the untreated group. One patient's records concerning treatment were missing. Biopsies were also taken from the scrotal testis in some of the unilateral cases to assess the patient's future fertility (Table 1). The testicular biopsies were fixed in Stieve's fixative and embedded in paraffin.
The patient work for the present study was done approximately 20 y ago. The aim of the original study was to improve the practice of diagnostics and therapy as well as the anatomical, endocrinologic, and histologic classification of the patients(15). At that time, the Children's Hospital did not have an Ethics Committee and it is possible that this study would not have met the ethical requirements prevailing today. However, because this unique material already existed, we felt that it should be used for scientific purposes to clarify the association of cryptorchidism and its treatment with programmed cell death.
In situ 3′-end labeling of DNA. For in situ detection of DNA fragmentation in the testes we used a nonradioactive DNA 3′-end labeling technique(16, 17). The fixed, paraffin-embedded testes were sectioned at 5 μm and mounted on slides coated with Vectabond (Vector Laboratories, Burlingame, CA), deparaffinized, and hydrated. To remove the mercury compound included in the acidic Stieve fixative and to neutralize the histologic sections, we first soaked the slides in Gram's iodine for 5 min and then left them for 30 min in 100 mM Tris, pH 8.
Proteinase-K treatment for 20 min at 37°C (Boehringer Mannheim, Indianapolis, IN; 5 μg/mL in 20 mM Tris, 2 mM CaCl2, pH 7.4) was followed by incubation for 10 min in terminal transferase buffer (200 mM potassium cacodylate, 25 mM Tris, 0.25 mg/mL BSA, 5 mM CoCl2, pH 6.6) at room temperature. DNA 3′-end labeling with digoxigenin-ddUTP was performed by adding terminal transferase (1 IU/μL, Boehringer Mannheim), digoxigenin-ddUTP (5 μM, Boehringer Mannheim), and ddATP (45 μM, Pharmacia, Uppsala, Sweden) in fresh buffer and incubating the sections in this solution at 37°C for 1 h.
After labeling, the slides were washed three times for 10 min at room temperature in buffer 1 (100 mM Tris, 150 mM NaCl, pH 7.5) and then incubated with blocking buffer (100 mM Tris, 150 mM NaCl, pH 7.5, 0.5% wt/vol blocking-reagent, Boehringer Mannheim) for 30 min at room temperature. Anti-digoxigenin antibody, conjugated with alkaline phosphatase, was next added to this buffer (1:8000 in 0.5% wt/vol blocking reagent), and the sections were incubated with the antibody at room temperature in a humidified chamber for 2 h.
Three 10-min washes in buffer 1 were followed by equilibration in alkaline phosphatase buffer (100 mM Tris, 100 mM NaCl, 50 mM MgCl2, pH 9.5), after which substrates for alkaline phosphatase (337.5 μg/mL nitro blue tetrazolium and 175 μg/mL 5-bromo-4-chloro-3-inodylphosphate; Boehringer Mannheim) were added. The color reaction was allowed to develop for about 20 min and terminated by soaking the slides in buffer 4 (10 mM Tris, 1 mM EDTA, pH 8) for 5 min. The stained sections were then mounted with coverslips, and the extent of apoptosis was analyzed by light microscopy using 400 × magnification. For each section (depending on its size), one to three randomly selected fields were scored, so that tubular and interstitial compartments were analyzed separately. Also the volume densities of seminiferous tubules and interstitial tissue were measured for each section using a 121-point square lattice in the eyepiece of the microscope. The results were then expressed as the number of apoptotic cells/mm2 of either tubular or interstitial area. The analysis was done without any prior knowledge of the sample.
DNA isolation and analysis for fragmentation. The specificity of the in situ 3′-end labeling technique was further validated by analyzing DNA fragmentation from isolated DNA. In this method, the total DNA was extracted from paraffin-embedded testicular tissue and quantified by absorbance at 260 nm(18, 19). One microgram of DNA from each sample was labeled at the 3′-ends with[α-32P]ddATP (3000 Ci/mmol; Amersham Corp., Arlington Heights, IL), using 25 IU of terminal transferase (Boehringer Mannheim)(18, 20). The labeled DNA samples were loaded onto 2% agarose gels (400 ng/lane) and separated by electrophoresis for 3 h at 50 V. The gels were dried for 2 h in a slab-gel drier and exposed to Kodak X-Omat films (Eastman Kodak Co., Rochester, NY) at -70°C for 2-6 h for qualitative analysis. After autoradiography, apoptosis with its radiolabeled, internucleosomally cleaved DNA fragments could be identified by its typical ladder pattern(18).
Statistical analysis. For statistical analysis the patients(whose ages ranged from 1.1 to 15.8 y) were divided into three age groups(<5 y, 5-9 y, and >9 y). Because there were only four abdominal testes in the series, these were omitted from further analysis, and the position of the testis was therefore recorded as either scrotal or inguinal. Analysis of variance was used to analyze the effects of hCG treatment, age, and testicular position on the amount of apoptosis in both tubular and interstitial compartments. Further comparisons between separate groups were done using Fisher's protected least significant difference.
RESULTS
In this study, testicular cell apoptosis was investigated mainly using thein situ 3′-end labeling technique to find the specific cells undergoing apoptosis. Apoptotic cell death in the human testis was noted to affect single cells that appeared scattered in the testicular tissue. Furthermore, it was observed in the cells of both tubular and the interstitial compartments. To quantify our findings, the amount of apoptosis in each analyzed section was recorded as the number of positively staining cells/mm2 of either tubular of interstitial area. The tubular and interstitial compartments were analyzed separately.
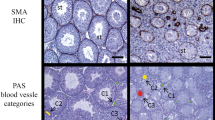
Apoptosis in the seminiferous tubules. With the in situ 3′-end labeling technique, the apoptotic cells in the seminiferous tubules were identified as being mostly spermatogonia, but a few positive Sertoli cells were also detected (Fig. 1). These apoptotic tubular cells appeared as single cells in both scrotal and cryptorchid testes.

Apoptotic cell death in situ in the germ cells of the human testis. A representative testicular biopsy from a scrotal testis is shown. The biopsy was taken from a 7-y-old boy less than 1 mo after hCG treatment. The histologic sections were stained with an in situ 3′-end labeling technique in which the digoxigenin-ddUTP label is detected by digoxigenin antibodies conjugated to alkaline phosphatase.Arrows indicate apoptotic cells.
To validate our in situ findings, we selected three biopsy specimens containing a great number of apoptotic cells detected in situ and three containing only a few positive cells per sample. We then analyzed the degree of DNA fragmentation from the isolated DNA(Fig. 2). The ladder pattern indicating the internucleosomal DNA fragmentation typical of apoptosis was pronounced in those samples in which apoptosis in situ was abundant(A-C), whereas in the samples with little apoptosis in situ (D-F) the ladder pattern was barely noticeable. This result corroborates the finding that the cells appearing to be positive in situ are indeed apoptotic.

DNA isolation and analysis for fragmentation. The specificity of the apoptotic staining in situ was further validated in six biopsies, of which the first three displayed considerably more apoptosis in situ than the other three. The typical ladder pattern indicates the extent of DNA fragmentation, showing high (lanes A-C) and low (lanes D-F) numbers of positive cells. For this detection technique, 1 μg of DNA from each biopsy sample was isolated before labeling its 3′-ends with radioactive [α-32P]ddATP. The DNA samples were then loaded onto agarose gels and separated by electrophoresis. After autoradiography DNA ladder assay was apparent.
The effect of hCG on spermatogonial apoptosis was further investigated by dividing the patients into four subgroups according to their hCG treatment. In the first group, no hormonal treatment had been given before the biopsy. In the other three groups, patients had received hCG injections and had had a biopsy taken either 0-1, 1-3, or 3-14 mo after the last hCG injection. Overall, the scrotal testes contained more apoptotic spermatogonia than the inguinal ones (p < 0.05). This also proved to be true when all four treatment groups were analyzed separately. Further analysis of the treatment groups demonstrated that immediately after hCG treatment the number of apoptotic cells had increased significantly compared with the nontreated group (p < 0.001). The effect of hCG was not permanent, because 1-3 mo after the last hCG injection the number of spermatogonial apoptosis was comparable to that in the nontreated group. The difference between the groups less than 1 mo after treatment and 1-3 mo after treatment was significant(p < 0.001). In the group in which more than 3 mo had elapsed after the last injection, the level of apoptosis was similar to the nontreated level (Fig. 3).

Effects of hCG treatment on apoptosis in seminiferous tubules of scrotal and cryptorchid testes. Patients were divided into four groups according to hCG treatment. In the first group, no hormone treatment was given. In the other three groups, the biopsy was obtained 0-1, 1-3, and 3-14 mo after the last injection of hCG. The histologic samples were stained using the in situ 3′-end labeling technique of DNA. The seminiferous tubules of the sections were analyzed under the light microscope and the results recorded as positive cells/mm2 of tubular area. Theasterisk denotes the statistical difference between the nontreated group and the various treatment groups (*p < 0.001; NS, nonsignificant difference).
To compare the levels of testicular apoptosis at different ages, the patients were divided into three age groups (1-5 y, 5-9 y, and 9-16 y), but the amount of tubular cell apoptosis did not differ significantly in these three groups.
Apoptosis in the interstitial cells. To investigate the effects of testicular position and hCG treatment on interstitial cell apoptosis, the histologic samples were divided into scrotal and inguinal ones and further into four treatment groups in which the time lapse between treatment and biopsy varied as described earlier. Testicular position did not affect the amount of interstitial cell apoptosis. Therefore, for further analysis, the scrotal and inguinal testes were grouped together. The specific cell types in the interstitium of the human prepubertal testis cannot be identified based on morphologic studies.
Apoptotic interstitial cells were found evenly scattered around the tissue samples (Fig. 4). In the interstitial tissue, in contrast to the findings in the seminiferous tubules, hCG treatment decreased the numbers of apoptotic cells. The samples from the nontreated patients and those operated on 0-1 mo after treatment showed interstitial cell apoptosis to similar extents. In the group operated on 1-3 mo after the last hCG injection, however, the extent of apoptosis was significantly less than in the nontreated group (p < 0.05). The effect of hCG treatment on interstitial cell apoptosis was likewise only temporary, because the amount of apoptosis returned to the nontreatment level 3 mo after the last hCG injection(Fig. 5).

Apoptotic cell death in situ in the interstitial cells of the human testis. A representative testicular biopsy from a scrotal testis is shown. The biopsy was taken from a 7.1-y-old boy with no hCG treatment. The histologic sections were stained with an in situ 3′-end labeling technique in which the digoxigenin-ddUTP label is detected by digoxigenin antibodies conjugated to alkaline phosphatase.Arrows indicate apoptotic cells.

Effects of hCG treatment on apoptosis in interstitial cells of scrotal and cryptorchid testes. Patients were divided into four groups according to hCG treatment. In the first group, no hormone treatment was given. In the other three groups, the biopsy was obtained 0-1, 1-3, and 3-14 mo after the last injection of hCG. The histologic samples were stained using the in situ 3′-end labeling technique of DNA. The interstitial compartments of the sections were analyzed under the light microscope and the results recorded as positive cells per square mm of interstitial area. The asterisks denote statistical differences between the nontreated group and the various treatment groups (**p< 0.05; NS, nonsignificant difference).
In the three age groups (1-5 y, 5-9 y, and >9 y) the level of apoptosis did not differ significantly from one group to another.
DISCUSSION
Our knowledge of apoptosis in reproductive organs has so far been largely based on rodent models. As far as we are aware, this is the first study to describe apoptotic DNA degradation in the human testis. We found that scrotally located testes displayed considerable numbers of apoptotic cells, suggesting that apoptosis occurs normally in the human testis prepubertally. Furthermore, we found that human testicular apoptosis is hormonally controlled. Using in situ analysis of DNA fragmentation, we were able to demonstrate apoptosis in both germ cells and somatic cells and it was noted to affect single scattered cells. The affected germ cells were spermatogonia.
In the normal testis, up to 75% of germ cells are known to die before reaching maturity(5, 21). From morphologic evidence, we know that the massive loss of germ cells in the rat testis occurs through apoptosis and that the process continues throughout testicular development(5). In rats at various developmental stages of spermatogenesis, in situ analysis shows that in younger animals(16 and 28 d) apoptosis affects mainly spermatocytes, and in older ones (32 d) spermatogonia(22). Quantitative analysis of apoptotic DNA fragmentation indicates that in the rat testis both germ cells and interstitial cells undergo apoptosis(4). Our study on human testes shows that apoptotic cell death is present in the normal prepubertal testis, the affected germ cells appearing to be spermatogonia. In addition to this, apoptotic interstitial cells were also detected along with few positive Sertoli cells.
In general, programmed cell death can be activated in two different ways, either by the presence of a tissue-specific inducer or by the withdrawal of a tissue-specific trophic factor, for instance a hormone(23). In addition to being responsible for the initiation and maintenance of spermatogenesis, these hormones have been shown to act as cell survival factors in the rat testis(4, 6, 22). For instance, hypophysectomy-induced massive testicular apoptosis can be prevented by administration of gonadotropin and testosterone(4). In the present study, we were able to demonstrate that apoptosis is hormonally controlled in the human testis also. Within the 1st mo after a 5-wk treatment with hCG, a significant increase in spermatogonial apoptosis was seen. Later, the amount of apoptosis returned to the baseline level. On the basis of a study on rats in which hCG was presented as a cell survival factor and in which GnRH antagonists and hypophysectomy were shown to induce testicular apoptosis(4). we suggest that the transient increase in spermatogonial apoptosis appearing 0-1 mo after hCG treatment is caused by hCG(or androgen) withdrawal rather than by hCG itself. Repeated administration of intramuscular hCG to prepubertal boys is known to cause a 100-fold increase in their serum testosterone level(24). This increase is followed by a phase of gradual withdrawal of the hormone effect(25).
Mature Leydig cells, not normally present in the human cryptorchid testes, are known to appear 4 d after hCG treatment and disappear again after 6-12 mo(14). We found that the number of apoptotic interstitial cells decreased 1 mo after hCG treatment, returning back to the nontreatment level 3 mo after the last hCG injection. The precise cell type undergoing apoptosis could not be identified morphologically. The exact mechanism accounting for these changes in the interstitial compartment is presently unclear. It may well be, however, that hCG-induced cell survival lasts for a few months after cessation of treatment as indicated by the survival of mature Leydig cells mentioned above. This is consistent with earlier observation of hCG serving as a testicular cell survival factor(4, 26).
Cryptorchidism is a common disorder, with a prevalence of 1.1% among 1 y olds(7). It is associated with histopathologic changes in the testicular tissue which are known to increase with age. The most important of them is the decrease in the number of germ cells appearing by the age of 2 y. If the cryptorchid testis remains undescended beyond puberty, it will never develop a normal spermatogenic pattern(8), and in the adult the seminiferous tubules will be totally devoid of germ cells(27). Even after early treatment of cryptorchidism, fertility seems to be decreased in adulthood(27–29). Studies on rats show that degenerative changes associated with experimentally induced cryptorchidism are mediated by an increase in germ cell apoptosis. In the rat, a decrease in testicular weight, in addition to the increase in the number of apoptotic germ cells associated with the induction of cryptorchidism, is apparent after 2 d of intraabdominal position(9). In our series of histologic samples of human undescended testes, however, the number of germ cells undergoing apoptosis was smaller than in the scrotal testes. The reason why experimentally induced cryptorchidism in the rat increases germ cell apoptosis, whereas cryptorchidism in humans seems to decrease it, is probably associated with the difference between these situations. Incomplete testicular descent is a chronic condition in which the testis is exposed to an unphysiologic milieu from birth for months or even years, whereas experimentally induced cryptorchidism represents the acute state of the same condition, induced after normal postnatal testicular development.
Since the importance of apoptosis has been realized, it has been postulated that the number of cells in a tissue does not depend on proliferation alone but rather on the quantitative relationship between the rates of cell proliferation and cell death. Normally, a balance exists between these two processes, so that the number of cells in the tissue neither increases nor decreases with time(23). Cryptorchidism is associated with a time-dependent decrease in germ cells, which indicates an imbalance between cell death and cell proliferation. In the present study we found that the incidence of germ cell apoptosis in the cryptorchid testis was lower than in the normal testis. Taking into account the aforementioned balance between the rates of cell death and proliferation, we suggest that in the cryptorchid testis the cell proliferation cycle is also severely decreased.
The adverse effects of hCG on testicular histology have been studied using a series of testicular biopsies from hCG-treated cryptorchid patients. Macroscopically, hCG has been reported to cause a temporary increase in intratesticular pressure and to render the testes hyperemic and enlarged. hCG treatment also increases the density per unit volume of the seminiferous tubules(14). Other hCG-induced temporary changes in testicular morphology include an increased intravascular polymorphonuclear leukocyte count and stimulation of spermatogenesis up to meiotic spermatocytes(30). Thus, hCG treatment accounts for various other histologic abnormalities, besides a temporary increase in germ cell apoptosis.
In the present study we showed that treatment with hCG causes a temporary increase in germ cell apoptosis both in normal and cryptorchid testes. It is too early to make any statement about the long-term effects of hCG treatment on testicular germ cell survival. However, these findings warrant further studies on the morphometric indices and fertility of these patients postpubertally, to determine the safety of hormonal treatments of cryptorchidism.
Abbreviations
- hCG:
-
human chorionic gonadotropin
- GnRH:
-
gonadotropin-releasing hormone
- dd:
-
dideoxy
References
Buja LM, Eigenbrodt ML, Eigenbrodt EH 1993 Apoptosis and necrosis: basic types and mechanisms of cell death. Arch Pathol Lab Med 117: 1208–1214
Schwartz LM, Osborne BA 1993 Programmed cell death, apoptosis and killer genes. Immunol Today 14: 582–590
Schwartzman RA, Cidlowski JA 1993 Apoptosis: the biochemistry and molecular biology of programmed cell death. Endocr Rev 14: 133–151
Tapanainen J, Tilly JL, Vihko K, Hsueh ALW 1993 Hormonal control of apoptotic cell death in the testis: gonadotropins and androgens as testicular cell survival factors. Mol Endocrinol 7: 643–650
Huckins C 1978 The morphology and kinetics of spermatogonial degeneration in normal adult rats: an analysis using a simplified classification of germinal epithelium. Anat Rec 190: 905–926
Troiano L, Faustini Fustini M, Lovato E, Frasoldati A, Malorni W, Capri M, Grassilli E, Marrama P, Franceschi C 1994 Apoptosis and spermatogenesis: evidence from an in vivo model of testosterone withdrawal in the adult rat. Biochem Biophys Res Commun 202: 1315–1321
Berkowitz GS, Lapinski RH, Dolgin SE, Gazella JG, Bodian CA, Holzman IR 1993 Prevalence and natural history of cryptorchidism. Pediatrics 92: 44–49
Elder JS 1988 The undescended testis: hormonal and surgical management. Surg Clin North Am 68: 983–1005
Shikone T, Billig H, Hsuch AJW 1994 Experimentally-induced cryptorchidism increases apoptotic cell death in rat testis. Biol Reprod 51: 865–872
Rajfer J, Handelsman DJ, Swerdloff RS, Hurwitz R, Kaplan H, Vandergast T, Ehrlich RM 1986 Hormonal therapy of cryptorchidism: a randomized double-blind study comparing human chorionic gonadotropin and gonadotropin-releasing hormone. N Engl J Med 314: 466–470
Christiansen P, Muller J, Buhl S, Hansen OR, Hobolth N, Jacobsen BB, Jorgensen PH, Kastrup KW, Nielsen K, Nielsen LB, Pedersen-Bjergaard L, Petersen KE, Petersen SA, Thamdrup E, Thisted E, Tranebjaerg L, Skakkeback NE 1992 Hormonal treatment of cryptorchidism-hCG or GnRH: a multicentre study. Acta Paediatr 81: 605–608
Hagberg S, Westphal O 1987 Results of combined hormonal and surgical treatment for undescended testis in boys under 3 years of age. Eur J Pediatr 146: 38–39
Karpe B, Eueroth P, Ritzen EM 1983 LHRH treatment in unilateral cryptorchidism: effect on testicular descent and hormonal response. J Pediatr 103: 892–897
Hjertkvist M, Läckgren G, Plöen L, Bergh A 1993 Does hCG treatment induce inflammation-like changes in undescended testes in boys. J Pediatr Surg 28: 254–258
Arsalo A 1982 Retained testis: diagnosis, classification and therapy. Dissertation, University of Helsinki, Helsinki
Gavrieli Y, Sherman Y, Ben-Sasson SA 1992 Identification of programmed cell death in situ via specific labeling of nuclear DNA fragmentation. J Cell Biol 119: 493–501
Billig H, Furuta I, Hsueh AJW 1993 Estrogens inhibit and androgens enhance ovarian granulosa cell apoptosis. Endocrinology 133: 2204–2212
Tilly JL, Hsueh AJW 1993 Microscale autoradiographic method for qualitative and quantitative analysis of apoptotic DNA fragmentation. J Cell Physiol 154: 519–526
Gross-Bellard M, Oudet P, Chambon P 1973 Isolation of high-molecular-weight DNA from mammalian cells. Eur J Biochem 36: 32–38
Tilly JL, Kowalski KI, Johnson AL, Hsueh AJW 1991 Involvement of apoptosis in ovarian follicular atresia and postovulatory regression. Endocrinology 129: 2799–2801
Kerr JB 1992 Spontaneous degeneration of germ cells in normal rat testis: assessment of cell types and frequency during the spermatogenic cycle. J Reprod Fertil 95: 825–830
Billig H, Furuta I, Rivier C, Tapanainen J, Parvinen M, Hsueh AJW 1995 Apoptosis in testis germ cells: developmental changes in gonadotropin dependence and localization to selective tubule stages. Endocrinology 136: 5–12
Berges R, Isaacs JT 1993 Programming events in the regulation of cell proliferation and death. Clin Chem 39: 356–361
Dunkel L, Perheentupa P, Apter D 1985 Kinetics of the steroidogenic response to single versus repeated doses of human chorionic gonadotropin in boys in prepuberty and early puberty. Pediatr Res 19: 1–4
Smals AGH, Pieters GFFM, Drayer JIM, Benraad TJ, Kloppenborg PWC 1979 Leydig cell responsiveness to a single and repeated hCG administration. J Clin Endocrinol Metab 49: 12–14
Dym M, Raj MHG 1977 Response of adult rat Sertoli cells and Leydig cells to depletion of luteinizing hormone and testosterone. Biol Reprod 17: 676–696
Kogan SJ 1987 Fertility in cryptorchidism. Eur J Pediatr 146: 21–24
Chilvers C, Dudley NE, Gougn MH, Jackson MB, Pike MC 1986 Undescended testis: the effect of treatment on subsequent risk of subfertility and malignancy. J Pediatr Surg 21: 691–696
Puri P, O'Donnell B 1988 Semen analysis of patients who had orchidopexy at or after seven years of age. Lancet 2: 1051–1052
Bergada C 1979 Use of gonadotropins for the evaluation of testicular function and correlations to biopsy of cryptorchid testis. In: Job JC (ed) Cryptorchidism: Diagnosis and Treatment, Karger, Basel, 97–107
Author information
Authors and Affiliations
Additional information
Supported by the [Illegible Text] Juselius Foundation (Finland).
Rights and permissions
About this article
Cite this article
Heiskanen, P., Billig, H., Toppari, J. et al. Apoptotic Cell Death in the Normal and Cryptorchid Human Testis: The Effect of Human Chorionic Gonadotropin on Testicular Cell Survival. Pediatr Res 40, 351–356 (1996). https://doi.org/10.1203/00006450-199608000-00026
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199608000-00026
This article is cited by
-
Apoptosis-related gene expression of mice testicular germ cells following long-term leptin administration
Comparative Clinical Pathology (2019)
-
Management of cryptorchidism: a survey of clinical practice in Italy
BMC Pediatrics (2012)
-
N-acetyl-l-cysteine modulates multiple signaling pathways to rescue male germ cells from apoptosis induced by chronic hCG administration to rats
Apoptosis (2012)
-
Hodenhochstand
Der Urologe (2010)
