
Abstract
Previous studies on the piglet colon in newborns cleared of bacterial metabolic activity showed a capacity for lactose absorption. Colonic absorption occurred at a flux rate equal to the assimilation of lactose by the small intestine but by a process that did not involve either glucose-galactose sodium cotransport or simple diffusion. Surprisingly, colonic lactose transport did not require either fermentation or cleavage of the disaccharide for uptake. Experiments were designed to test the selectivity of the colonic transport process for a variety of carbohydrates. Colonic tissues from 4-7-d-old piglets were mounted in Ussing chambers and the mucosal-to-serosal flux of radiolabeled carbohydrates was compared with that of lactose. The results showed a 3-4-fold greater flux of galactose-containing sugars as compared with glucose-containing carbohydrates at concentrations up to 40 mM. Even lactulose, a synthetic disaccharide assumed to require bacterial digestion before assimilation, was transported readily.N-Acetylgalactosamine, a component of colonic mucus, inhibited the flux of lactose, whereas N-acetylglucosamine did not. Similarly, lactosylated BSA inhibited lactose flux, whereas nonlactosylated BSA did not. The capacity of the colon of the newborn to differentiate moieties as similar as glucose and galactose suggests an absorptive process for carbohydrates with a high degree of discrimination.
Similar content being viewed by others

Main
The colon not only functions to reabsorb fluid and electrolytes but also is involved in the recovery of endogenous and exogenous carbohydrates(1). In the newborn, colonic retrieval of malabsorbed lactose energy may have a substantial nutritional impact(2). Beyond the newborn period, luminal fiber, secretions, mucus, and endogenous and bacteria-derived cellular debris represent abundant sources of nutrients for colonocytes, which use short-chain fatty acids from fermentation to maintain mucosal integrity(3). Although it has been assumed that bacterial fermentation accounts for the recovery of luminal carbohydrates from the colon, perfusions in newborn pigs have demonstrated that an alternate route for absorption exists in the colon cleared of bacterial metabolic activity(4). In one study, a perfusate containing lactose showed avid absorption from the colon. No evidence of luminal fermentation products or of mucosal β-galactosidase activity was found to suggest that lactose digestion had occurred either from bacterial or mucosal enzymatic activity. Further studies on colonic tissue mounted in Ussing-type chambers showed a concentration dependent flux of lactose across the colon that equalled the rate of assimilation of lactose in the jejunum, yet was not due to a glucose-galactose sodium cotransport mechanism(5). One surprising finding was that the colonic serosal bath contained intact lactose, not free glucose and galactose, indicating that neither fermentation nor cleavage of the sugar was required for transport. There was negligible flux of small homologous oligomers of PEG 400, which are insoluble in lipid and therefore useful as a measure of passive permeability(6). This finding suggests that paracellular sieving was not responsible for the movement of lactose.
Flux experiments in mounted colonic tissue were used to explore the selectivity of colonic absorption of carbohydrate in newborn piglets. The results suggest a galactose-selective process.
METHODS
Animals and preparation. All studies were approved by the Animal Care and Use Committee of the Wexner Research Institute. Newborn standard Yorkshire pigs 4-7 d old and 2.0-3.5 kg were brought from the breeding farm to the laboratory on the day of study. After anesthesia, intestinal tissues were removed and the animals were killed by an injection of concentrated pentobarbitol. Following a protocol previously published(5), small and large intestinal segments were stripped of their muscular coats and mounted in Ussing chambers (1.12-cm2 surface area) that isolate mucosal from serosal baths. After tissue stabilization, test carbohydrates were added to the mucosal bath. Transepithelial isotonicity was maintained between mucosal and serosal baths by balancing test carbohydrates with the simultaneous addition of an equal amount (millimoles) of mannitol. Bacterial fermentation was evaluated by HPLC analysis for short-chain fatty acids in the mucosal and serosal solutions at the end of incubation. Further, in early studies, 1-mL samples from both bathing solutions were incubated with additional lactose in anaerobic chambers and assayed by HPLC for fermentation products to ensure that bacterial metabolism did not occur.
Study 1: Transepithelial flux of a variety of carbohydrates from the colon. A series of separate flux experiments were performed in 4-7-d-old piglets in which the flux of [U-14C]lactose was compared with equimolar radiolabeled galactose, lactulose, glucose, maltose, or glucose-containing starch oligomers with a mean DP of 23. Cumulatively, there were three galactose-containing (galactose, Mr 180; lactulose and lactose, Mr 342 each) and three glucose-containing(glucose, Mr 180; maltose, Mr 342; and glucose polymers, mean Mr 3744) carbohydrates tested. Analyzed individually, each glucose-containing sugar had a mean flux less than that of lactose, whereas each galactose-containing sugar had a flux equal to or greater than that of lactose. The results were used to generate the hypothesis for studies 2-4; that is, that colonic absorption in newborns discriminates between galactose- and glucose-containing carbohydrates.
In the studies grouped as study 1, carbohydrates were labeled with14 C (lactose, maltose, glucose, glucose polymers) or with 3H(galactose and lactulose) and combined with unlabeled carbohydrate to achieve a specific activity of 0.02 μCi/mmol in 10 mM concentrations. Flux(nanomoles·cm-2·h-1) was determined at the end of a 60-min incubation by scintillation counting of a 1-mL sample, which represents 8% of the serosal bath, as described previously(5, 7). Radiolabeled glucose polymers(DP23avg) were made from U-14C-labeled tobacco starch enzymatically reduced to an array of small oligomers with lengths of DP>14, following the methods of Murray et al.(8) and Sloan et al.(9). The concentration used would be equivalent to 10 mM glucose units if the polymers were completely cleaved to individual glucose units. Lactulose(4-O-β-D-galactopyranosyl-D-fructose) is a synthetic disaccharide of similar size and weight to that of lactose but containing the constituents galactose and fructose. No mucosal enzymes exist for its degradation; bacterial fermentation has been considered to account for its assimilation(10).
In initial studies, the serosal solution was drained and analyzed by HPLC and thin layer chromatography, as described previously(5). None of the parent compounds underwent metabolism during its flux to the serosal bath.
Study 2: Comparison of flux of glucose and galactose over a range of concentrations. To confirm the preference of the colonic mucosal transport process for galactose and to discern whether saturation occurred, a concentration curve was generated for both [14C]glucose and[3H]galactose in 4-d-old animals. Repeating the procedures of study 1, the individual fluxes of glucose and galactose were compared in colon tissue over a concentration range from 1 to 40 mM, considered to represent the physiologic range in the intestinal lumen(11).
Study 3: Comparison of flux of [U-14C]glucose and[1-3H]galactose from a mixture containing both sugars. Flux of the two monosaccharide components of lactose were directly compared by the addition of 40 mM of each monosaccharide in the mucosal bath. On glucose the label resided on carbon 1, whereas on galactose the label was on the hydrogen of carbon 1. Jejunum was included as a control. The serosal bath was assayed by dual-channel scintillation counting.
Study 4: Inhibition of lactose flux by components of colonic glycoproteins. To test the selectivity of process further, inhibition studies were designed. In study 4a, lactose flux was measured when coincubated with N-acetylgalactosamine and N-acetylglucosamine, aminated compounds with Mr 221. Both would be available in the colonic lumen as glycoprotein components of endogenous mucopolysaccharides. BSA (Mr 60,000) was used to test steric hinderance of a large molecule. In separate chambers, the inhibitors (25 mM) were preincubated for 5 min in the mucosal bath before the addition of 40 mM[14C]lactose to determine their capacity to inhibit lactose flux. Incubation was then allowed to proceed for 1 h.
In study 4b, 25 mM BSA was lactosylated and compared with nonlactosylated BSA to determine whether the addition of a terminal galactose moiety on albumin would impede the flux of 40 mM [14C]lactose. Lactosylated BSA was made by using published methods in which BSA and lactose were incubated in the presence of NaCNBH3 and the lactosylated albumin purified over a Bio-Gel P2 column(12). After completion of a 1-h flux study, the capacity of BSA or lactosylated BSA to inhibit [14C]lactose flux was determined. Thereafter, the serosal bath was drained, weighed, and assayed for the presence of carbohydrate and protein to ascertain whether the addition of lactose to the albumin molecule allowed transcytosis of a high molecular weight protein that would otherwise have been excluded. As a control for serosal protein accumulation during incubation in the Ussing chambers, in each study one chamber was mounted without the addition of any mucosal test substrate. In a subsequent experiment 14C-labeled lactosylated BSA was made by the methods described above, and a 1-h flux study was performed. The mounted colonic tissue was recovered and assayed to determine whether lactosylated BSA accumulated in the mounted tissue without transcytosis to the serosal bath.
Materials. Radiolabeled glucose and galactose were purchased from New England Nuclear Dow Research Products, Boston MA. Lactose and lactulose were from American Radiolabeled Chemical, Inc., St. Louis, MO; whereas maltose came from ICN, Irvine, CA. Mannitol, BSA,N-acetylglucosamine, and N-acetylgalactosamine came from Sigma Chemical Co., St. Louis, MO.
Statistical analysis. The experiments in study 1 on various sugars were performed individually and therefore the fluxes of each could only be compared with the lactose control using simple t tests. Differences in flux between galactose- versus glucose-containing sugars led to the hypothesis that colonic absorption of carbohydrate is galactose-selective. In study 2, fluxes of glucose and galactose were compared over a range of concentrations using paired t tests. In study 3, glucose and galactose were coincubated in colonic and jejunal tissues and their fluxes. To overcome missing data points a Mann-Whitney test was used. In study 4a, the three inhibitors-BSA, N-acetylgalactosamine, andN-acetylglucosamine-were compared with each other based on their ability to inhibit lactose flux using Wilcoxin signed-ranks tests. In study 4b, BSA was compared with lactosylated BSA by paired t test.
RESULTS
Study 1: Transepithelial flux of carbohydrates in the colon. Fluxes of mono-, di-, and polysaccharides (glucose polymers) are presented in Figure 1. Fluxes ranged from 90 ± 13 nmol·cm-2·h-1 for the polymer solution to 1131± 289 nmol·cm-2·h-1 for lactulose. Carbohydrates containing galactose (galactose, lactose, lactulose) showed flux values 3-4-fold higher than those containing glucose (glucose, maltose, glucose polymers). By simple t tests, all three glucose-containing sugars had fluxes less than lactose (p < 0.05), whereas sugars containing galactose equaled or surpassed the flux of lactose.

Mucosal-to-serosal flux of galactose-containing carbohydrates (shaded: Lactu, lactulose; Gal, galactose;Lact, lactose) and glucose-containing carbohydrates (open:GP23, glucose polymers; Malt, maltose; Glc, glucose) across newborn piglet colon in Ussing chambers. In all studies,n = number of tissues studied and values represented are±SEM.
Study 2: Comparison of flux of glucose and galactose over a range of concentrations in colon. Glucose and galactose concentration curves are derived by linear regression are presented in Figure 2[for y = a + b(x), for glucose y = -40.6 + 21.4(glucose concentration); for galactose y = 139 + 70 (galactose concentration)]. At each concentration galactose flux was significantly greater than that of glucose (p < 0.001). At 40 mM galactose flux was 2944 ± 394 nmol·cm-2·h-1 compared with 954 ± 410 nmol·cm-2·h-1 for glucose. Neither saturated between 1 and 40 mM under the experimental conditions, which differed from results in our lab with glucose in jejunum under similar conditions(13).

Mucosal-to-serosal flux of galactose (GAL) compared with glucose (GLC) between 1 and 40 mM concentrations in colonic tissue from piglets. The lines are derived by linear regression. Values are mean ± SEM. Differences were significant at each concentration tested, p < 0.001.
Study 3: Comparison of equimolar [14C]glucose with[3H]galactose. Figure 3 shows a mean flux of galactose of 3258 ± 232 from the colon and 2955 ± 358 from the jejunum (NS). Although coincubated with galactose, the flux of glucose was only 722 ± 125 from the colon, substantially less than that of equimolar galactose (p < 0.002). Glucose flux in the jejunum was 3229 ± 688, similar to that of galactose in jejunum and in colon(NS).

Mucosal-to-serosal flux of [14C]glucose(solid) and [3H]galactose (hatched) from a mucosal solution that contained 40 mM of each sugar in both colonic and jejunal piglet tissue. Values are mean ± SEM. In the colon, galactose flux exceeded that of glucose, p < 0.0001; no differences were noted between galactose flux in jejunum or colon, or between glucose and galactose flux in jejunum.
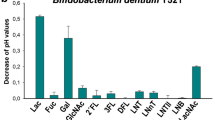
Study 4: Inhibition of lactose flux by components of glycoproteins of mucus available in colon. The results of study 4a are shown in Figure 4. The presence of N-acetylgalactosamine lowered the flux of lactose to that of the flux of the BSA andN-acetylglucosamine (p < 0.05), which were similar to the mean flux of lactose recorded in study 1.

Flux across piglet colon in the presence of a 40 mM[14C]lactose solution of 25 mM glucosamine, galactosamine, or BSA. The lactose flux from study 1 in the absence of inhibition was included for comparison (open bar). Galactosamine inhibited lactose flux 3-fold(p < 0.05) relative to glucosamine and BSA and to the lactose flux in study 1.
Study 4b addressed two further questions. First, could BSA be made to inhibit the flux of lactose by the addition of a terminal lactose moiety? Second, could the addition of lactose to BSA induce its transport (absorption or transcytosis)? In Figure 5, the mean flux of[14C]lactose in the presence of BSA was 636 ± 231, whereas in the presence of lactosylated BSA lactose flux was only 212 ± 120, nearly a 40% reduction (p < 0.02). Analysis of the carbohydrate and protein content of the serosal baths from the BSA, lactosylated BSA, and control groups indicates that transcytosis of BSA did not occur even when the molecule was lactosylated. In addition, after incubation with 40 mM14 C-labeled lactosylated BSA, mounted colonic tissue was retrieved and assayed by scintigraphy (data not shown). Colonocyte retention of the molecule accounted for a mean of only 92.1 ± 46.1 μmol (35-164 μmol) of labeled lactosylated albumin per mean tissue weight of 83.1 ± 22.0 g. The results of scintillation counting confirmed the previous findings obtained with cold lactosylated BSA that transcytosis of the BSA molecule to the serosal bath did not occur even with the addition of a terminal galactose.

Flux across piglet colon in the presence of a 40 mM[14C]lactose solution that contained either 25 mM BSA or lactosylated BSA (LBSA). The lactosylated molecule inhibited the flux of lactose nearly 3-fold relative to the nonlactosylated molecule (p < 0.01).
DISCUSSION
Using colonic tissue from newborn piglets mounted in Ussing chambers we tested the hypothesis that the colonic absorption of carbohydrates is selective. The hypothesis was derived from a series of comparisons between lactose and other sugars, grouped as study 1 in this report, which showed an apparent preference for galactose-containing sugars. Even lactulose, a synthetic disaccharide that cannot be cleaved by mucosal enzymes and is generally assumed to require degradation by bacterial enzymatic activity, was readily transported across the colonic tissue. Studies confirmed that galactose had a 3-4-fold higher rate of flux in colon than glucose at all concentrations tested between 1 and 40 mM. Similarly, galactosamine, a carbohydrate component of colonic glycoproteins, inhibited the flux of lactose, whereas glucosamine and BSA did not. Yet when BSA was lactosylated(adding a terminal galactose moiety), it too reduced the flux of lactose across the colon tissue, suggesting that it was not simply the stearic hinderance of a large molecular weight molecule that inhibited lactose flux.
Previously, we established that lactose absorption from colon does not occur via a glucose-galactose sodium cotransport process, such as that in the small intestine(4, 5). The lack of digestion or fermentation of lactose, its assimilation in colon (passage to the serosal bath) as a disaccharide, and the fact that small oligomers of PEG 400 did not cross simultaneously with lactose, led us to speculate that the colonic transport process could represent transcytosis rather than simple paracellular diffusion. Our findings differed somewhat from the description of PEG 400 and inulin movement in the perfused rat colon as described by Krugliak et al.(14) and by Ma et al.(15). In both of those studies the colonic mucosa showed permselectivity, but movement was clearly tied to water flux, suggesting paracellular sieving. In Ussing chambers water flux is negated by balanced osmolality on both sides of the tissue, yet flux of galactose-containing sugars was not reduced. In other studies not presented here, we tested lactose absorption from piglet colon during recirculating perfusions in which osmolality was 230 or 600 mosm. Lactose absorption was unaffected by changing the water flux from absorption to secretion (our unpublished data). Collectively, the data suggest that carbohydrate absorption occurs by a process more complicated than simple diffusion.
A process exists in the colon that is highly selective for the transport of certain carbohydrate-containing moieties. The findings could be explained by only a few possibilities. A mucosal receptor for galactose is feasible. If present, saturation would be expected, however, and it did not occur in study 2 at least between 1 and 40 mM, the concentration range reported as physiologic for glucose in rabbit jejunum(7, 11). Another possibility is a permselective process that induces an alteration in the paracellular flux of certain sugars. This too is unlikely. Glucose and galactose did not show similar fluxes when coincubated in study 3. Alterations in paracellular structure or in water flux should have opened it to both molecules equally. The two sugars are similar in size, molecular weight, and constituent carbons, but have very different stearic shapes, so discrimination between them requires a higher degree of specificity than could be accounted for by passive paracellular movement. Another possible route of absorption is a galactose sensitive receptor-mediated endocytic mechanism.
If a receptor-mediated process is functional in the newborn colon, there are a few reasons why it may have failed to saturate in the preparation used. Saturation may have occurred but only at much lower concentrations than tested here, as was noted with mannose(16). If saturation occurred at low concentration, diffusion would be required to explain our results and diffusion is unlikely for the reasons described above. Another explanation for the failure to saturate could be that dietary carbohydrates, such as galactose and lactose, do not have a sufficient affinity(Kd) for the receptor to clearly demonstrate saturation. For example, asialofetuin and asialoorosomucoid both demonstrated a million-fold greater affinity for the asialoglycoprotein receptor of liver than did galactose, illustrating that a large substrate with several galactoses exposed can substantially heighten affinity(17). A third possibility is that the conditions of our experiment may have obscured saturation. Even the asialoglycoprotein receptor, when tested at 37°C, failed to show the saturability that was clearly evident when it was retested at 4°C(18). At the lower temperatures, binding is retained, but endocytosis and recycling of the receptor are inhibited, making saturation more apparent(19).
The presence of a colonic transport process for galactose-containing carbohydrates is intriguing. Lactose is not completely assimilated in the small bowel in neonates(20–23). The described colonic transport pathway may offer the neonate a substantial reserve that, in conjunction with bacterial metabolism, prevents lactose energy loss in feces. However, it must be kept in mind that the current and previous studies on colonic uptake of carbohydrates done in our lab were performed under conditions that excluded bacterial metabolism, which probably contributes substantially to the degradation of luminal carbohydrates, both exogenous and endogenous(23). Still, such a transport process could provide an additional mechanism to prevent an osmotic influx of fluid into the colon and the accumulation of acid due to fermentation of sugars(24, 25). Either of these pathophysiologic states would limit carbohydrate energy salvage to the detriment of the newborn.
This study further characterizes a potential role for the colon in neonatal nutrition. The transport process described appears to favor galactose-containing carbohydrates, which could include exogenous sources, such as dietary milk, and endogenous sources, such as galactoproteins of mucus or bodily secretions. The extent of the colon's contribution to carbohydrate energy salvage in the presence of the colonic flora, the duration of the phenomenon after the newborn period, and the specific mechanism involved merit further study.
Abbreviations
- PEG:
-
polyethylene glycol
- DP:
-
degree of polymerization
References
Macfarlane GT, Cummings JH 1991 The Large Intestine: Physiology, Pathophysiology, and Disease. Raven Press, New York, 51–92.
Kien CL, Heitlinger LA, Li BUK, Murray RD 1989 Digestion, absorption, and fermentation of carbohydrates. Semin Perinatol 13: 78–87.
Sakata, T 1991 Effects of short-chain fatty acids on epithelial cell proliferation and mucus release in the intestine. In Roche AF(ed) Short-Chain Fatty Acids: Metabolism and Clinical Importance (Report of the Tenth Ross Conference on Medical Research). Ross Laboratories, Columbus, OH, 63–67.
Murray RD, Ailabouni AH, Powers PA, McClung HJ, Li BUK, Heitlinger LA, Sloan HR 1991 Absorption of lactose from colon of newborn piglet. Am J Physiol 261:G1–G8.
Murray RD, Ailabouni AH, Powers PA, Heitlinger LA, Li BUK, McClung HJ, Sloan HR 1993 Lactose flux occurs by differing mechanisms in the colon and jejunum of newborn piglets. Pediatr Res 33: 568–572.
Krugliak P, Hollander Dm Ma TY, Tran D, Dadufalza VD, Katz KD, Le K 1989 Mechanisms of polyethylene glycol 400 permeability in perfused rat intestine. Gastroenterology 97: 1164–1170.
Heitlinger LA, Li BUK, Murray RD, McClung HJ, Sloan HR, DeVore DR 1991 Glucose flux from dietary disaccharides: all sugars are not absorbed at equal rates. Am J Physiol 261:G818–G822.
Murray RD, Kerzner B, Sloan HR, McClung HJ, Gilbert M, Ailabouni A 1986 The contribution of salivary amylase to glucose polymer hydrolysis in premature infants. Pediatr Res 20: 186–191.
Sloan HR, Kerzner B, Scobell HD, Strohl WR, Ailabouni AH 1985 Large scale production of glucose oligomers and polymers for physiological studies in humans. Prep Biochem 279: 259–279.
Saunders DR, Wiggins HS 1981 conservation of mannitol, lactulose, and raffinose by the human colon. Am J Physiol 241:G397–G402.
Ferraris BP, Yasharpour S, Lloyd KCK, Mirzayan R, Diamond JR 1990 Luminal glucose concentration in the gut under normal conditions. Am J Physiol 259:G822–G837.
Van Der Sluijs P, Postema B, Meijer DKF 1987 Lactosylation of albumin reduces uptake rate of dibromosulfophthalein in perfused rat liver and dissociation rate from albumin in vitro. Hepatology 7: 688–695.
Heitlinger LA, Li BUK, Murray RD, McClung HJ, Sloan HR, DeVore DR, Powers P 1991 Glucose flux from dietary disaccharides: all sugars are not absorbed at equal rates. Am J Physiol. 261:G818–G822.
Krugliak P, Hollander D, Schlaepfer CC, Katz KD, Dadufalza VD, Ma TY 1990 Polyethylene glycol 400 penetration of the colonic epithelial barrier of the rat. Gastroenterology 99: 1001–1007.
Ma TA, Hollander D, Erickson RA, Truong H, Nguyen H, Krugliak P 1995 Mechanism of colonic permeation of inulin: is rat colon more permeable than small intestine?. Gastroenterology 108: 12–20.
Yamaguchi Y, Dalle-Molle E, Hardison WGM 1993 Hepatocyte horseradish peroxidase uptake is saturable and inhibited by mannose-terminal glycoproteins. Am J Physiol 264:G880–G885.
Rice KG, Lee YC 1993 Oligosaccharide valency and conformation in determining binding to the asialoglycoprotein receptor of rat hepatocytes. Adv Enzymol Relat Areas Mol Biol 66: 41–83.
Connolly DT, Hoppe CA, Hobish MK, Lee YC 1981 Steady-state and kinetic analysis of the binding of asialoorosomucoid to the isolated rabbit hepatic lectin. J Biol Chem 256: 12940–12948.
Schwartz AL 1984 The hepatic asialoglycoprotein receptor. CRC Crit Rev Biochem 16: 207–233.
MacLean WC, Fink BF 1980 Lactose malabsorption by premature infants: magnitude and clinical significance. J Pediatr 97: 383–388.
Modler S, Kerner JA, Castillo RO, Vreman HJ, Stevenson DK 1988 Relationship between breath and total body hydrogen excretion rates in neonates. J Pediatr Gastroenterol Nutr 7: 554–558.
Murray RD, Boutton TW, Klein PD, Gilbert M, Paule CL, MacLean WC 1990 Comparative absorption of [13C]glucose and[13C]lactose by premature infants. Am J Clin Nutr 51: 59–66.
Kien CL, Liechty EA, Myerberg DZ 1987 Dietary carbohydrate assimilation in the premature infant: evidence for a nutritionally significant bacterial ecosystem in the colon. Am J Clin Nutr 46: 456–460.
Chauve A, Devroede G, Bastin E 1976 Intradluminal pressures during perfusion of the human colon in situ. Gastroenterology 70: 336–340.
Mortensen PB, Holtug K, Bonnen H, Clausen MR 1990 The degradation of amino acids, proteins, and blood to short-chain fatty acids in colon is prevented by lactulose. Gastroenterology 98: 353–360.
Acknowledgements
The authors thank John Hayes for technical assistance with these studies.
Author information
Authors and Affiliations
Additional information
Supported by grants from the National Institute of Child Health and Human Development, HD-21295, and from the Children's Hospital Research Foundation.
Rights and permissions
About this article
Cite this article
Murray, R., Ailabouni, A., Heitlinger, L. et al. Galactose-Containing Carbohydrates Are Preferentially Absorbed in the Neonatal Pig Colon. Pediatr Res 39, 656–660 (1996). https://doi.org/10.1203/00006450-199604000-00016
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199604000-00016
