
Abstract
Na+,K+-ATPase in tubular cells plays a pivotal role for the regulation of renal sodium excretion. In adult rats the activity of this enzyme is inhibited by natriuretic hormones and stimulated by antinatriuretic hormones. Here we have examined the tubular response to α-adrenergic agonists and neuropeptide Y (NPY) in both infant and adult rats. In the adult kidney, α-adrenergic agonists and NPY stimulate Na+,K+-ATPase activity via Ca2+-dependent pathways. Oxymetazoline, a selective α-adrenergic agonist, and NPY failed to stimulate proximal tubular (PT) Na+,K+-ATPase activity in 10-d-old rats in doses of 10-8 to 10-5 M and 10-8 to 10-6 M, respectively, but when tubules were incubated simultaneously with both oxymetazoline 10-8 M and NPY 5 × 10-9 M, stimulation was observed in both 10- and 40-d-old rat PT. This effect was abolished by FK 506, an inhibitor of Ca2+ and calmodulin-dependent protein phosphatase 2B in both age groups. A23187, a calcium ionophore, stimulated Na+,K+-ATPase in both infant and adult PT, but 10-fold higher doses were required for the infant tubules. The effect ofα-adrenergic agonists and NPY on free intracellular Ca2+ was studied in PT cells in primary culture. The Ca2+ response to each agent was less pronounced in infant than in adult cells. Preincubation with NPY, which increases Ca2+ influx into the cells, enhanced the response to the α-adrenergic agonist in both infant and adult cells. The results support the concept that the systems regulating renal tubular Na+,K+-ATPase and sodium metabolism undergo postnatal maturation.
Similar content being viewed by others


Main
The infant kidney does not respond to changes in salt and water balance as well as the adult kidney. As a consequence, homeostatic disturbances are quite common. Sick infants, and particularly sick preterm infants, often have inappropriate sodium losses resulting in negative sodium balance(1).
Sodium excretion is determined by the rate of tubular reabsorption, which in turn is determined by the activity of the sodium transporters in the various tubular segments. Na+,K+-ATPase is of central importance for the regulation of renal sodium reabsorption by generating the driving force for transcellular transport of many electrolytes and organic solutes. In the adult kidney Na+,K+-ATPase is the target for a large number of hormones that regulate sodium metabolism(2). Natriuretic hormones, such as dopamine, down-regulate the activity of Na+,K+-ATPase(3). The finding that dopamine inhibition of renal tubular Na+,K+-ATPase is attenuated in the infant rat(4, 5) led us to speculate that an attenuated response to hormones regulating tubular sodium transport is one of the main reasons why infants have a limited capacity to regulate sodium balance.
Antinatriuretic hormones such as NE, acting on α-adrenergic receptors, will in the adult kidney stimulate Na+,K+-ATPase at nonsaturating Na+ concentrations(2, 6). This effect is mediated by Ca2+ and calmodulin-dependent PP2B. NPY, which is colocalized with NE in renal nerve endings, also stimulates Na+,K+-ATPase via PP2B. In addition, α-adrenergic agonists and NPY have a synergistic effect on a tubular Na+,K+-ATPase activity(7). Both α-adrenergic agonists and NPY initiate an increase in cytoplasmic Ca2+(8, 9).
Here we have examined the effect of the α-adrenergic agonist and NPY on Na+,K+-ATPase activity in proximal tubular segments and on cytoplasmic Ca2+ in renal PT cells from infant and adult rats. We found that the Na+,K+-ATPase response to each of the drugs was attenuated. In contrast, the synergistic actions of α-adrenergic agonists and NPY on both Na+,K+-ATPase activity and intracellular Ca2+ were well developed in the infant rat PT cells.
METHODS
Animals
Male Sprague-Dawley rats (ALAB, Sollentuna, Sweden) aged 10-12 (infant) and 40-45 d (adult) were used. Body weights were 22-28 g and 160-200 g, respectively. The pups were kept with their dams, and the adult rats were fed rat chow (Ewos, Södertälje, Sweden) ad libitum and drank tap water.
Measurement of Na+,K+-ATPase Activity in Single Dissected Rat PT Segments
PT segments were dissected as previously described(10). The rats were anesthetized with Mebumal vet (Nord Vacc, Stockholm, Sweden; 5-6 mg/100 g of body weight, intraperitoneally). The left kidney was exposed and perfused with a modified Hanks' solution having the following composition (in mM): 137 NaCl, 5 KCl, 0.8 MgSO4, 0.33 Na2HPO4, 0.44 KH2PO4, 2 CaCl2, 1 MgCl2, and 10 Tris-HCl, with 0.05% collagenase (Sigma Chemical Co., St. Louis, MO) and 0.1% BSA (Behringwerke, Marburg, Germany). The kidney was removed and cut along its corticopapillary axis into small pyramids that were incubated for approximately 15-20 min at 35°C in the perfusion solution to which 10-3 M butyrate had been added to optimize mitochondrial respiration(11) and bubbled with 95% O2 and 5% CO2. After incubation, the tissue was rinsed three times with a solution with the same composition as the perfusion solution, except that collagenase and BSA were deleted and the CaCl2 concentration was reduced to 0.25 mM.
Microdissection was performed on ice under a stereomicroscope. The single PT segments (length 0.5-1.0 mm) were manually dissected from the outer cortex and individually transferred to the concavity of a bacteriologic slide in a drop of the microdissection solution and photographed for length determination in an inverted microscope at 100× magnification. Tubules were stored on ice until dissection was completed, at most for 30 min.
The tubule segments were incubated for 30 min at room temperature either in 1 μL of microdissection solution alone (control tubules) or in 1 μL of microdissection solution containing one or more of the drugs mentioned below(experimental tubules). Unless otherwise stated, the Na+ concentration of the solution was 20 mM, and 117 mM choline chloride was added to obtain a final osmolality of 290 mosmol/kg of water.
Na+,K+-ATPase activity was determined as described elsewhere(10). The preincubation period was stopped by rapid cooling to 4°C. To clamp intracellular Na+ concentration and to allow ATP to enter the cells, the tubular segments were made permeable by freezing and thawing. They were incubated at 37°C for 15 min in a medium containing (in mM): 20 or 70 NaCl, 5 KCl, 10 MgCl2, 1 EGTA, 100 Tris-HCl, 10 Tris-ATP (10 Na2ATP instead when Na+ concentration was 70 mM), and [γ-32P]ATP (DuPont NEN, Boston, MA); 2-5 Ciμmol-1 in tracer amounts (5 nCi μL-1) in the absence or presence of 2 mM ouabain (U. S. Biochemical Corp., Cleveland, OH). For determination of ouabain-insensitive (Mg-dependent) ATPase activity, NaCl and KCl were omitted, and Tris-HCl was 150 mM. The [32P]phosphate liberated by hydrolysis of ATP was separated by filtration through a Millipore filter after absorption of the unhydrolyzed nucleotide on activated charcoal, and radioactivity was determined in a liquid scintillation spectrometer.
In each study, total ATPase activity and ouabain-insensitive ATPase activity was measured on each of five to eight other tubule segments. Na+,K+-ATPase activity (picomoles of inorganic[32P]phosphate hydrolyzed/mm of tubule/h) was then calculated as the difference between the mean value for total ATPase and ouabain-insensitive ATPase activity and expressed either as absolute values or percent values of those from control tubules obtained in each experiment.
Measurement of Intracellular Calcium in Cultured Rat PT Cells
Preparation of cells. Primary cultures of PT cells were prepared using a modification of the method described by Larsson et al.(12). The cells were cultured in Dulbecco's modified Eagle's medium (20 mM HEPES, 24 mM NaHCO3, 50,000 IU L-1 penicillin, and 50 mg L-1 streptomycin, pH 7.4) with 10% fetal bovine serum (Life Technologies, Inc., Bethesda, MD) in an incubator at 37°C with 95% O2 and 5% CO2. After 28 h in culture, the medium was changed to Dulbecco's modified Eagle's medium with 1% fetal bovine serum. The cells were examined approximately 18 h later.
Quantitative fluorescence microscopy. Single cell intracellular calcium ([Ca2+]i) was quantified using Fura-2(Fura-2/AM) (Molecular Probes, Eugene, OR). After loading the cells with this dye, the petri dish was placed on a stage of a Zeiss IM 405 inverted microscope, and a single cell was focused. A computerized spectrophotometer system (DM3000 cm; Spex Industries, Edison, NJ) was used, and emitted light was measured by photon counting (Hamamatsu R928, Japan). All experimental solutions were kept at 37°C and equilibrated with 95% O2 and 5% CO2. The [Ca2+]i was measured using a balanced salt solution (concentration in mM: NaCl 109, KCl 5, CaCl2 1, MgCl2 1.2, Na2HPO4 1, NaHCO3 25, HEPES 20, glucose 5, and sodium butyrate 1). The cells were exposed to the indicated drugs by completely removing the 2.5-mL solution in the petri dish, except for a thin layer covering the cells, and adding solution with NPY or phenylephrine(drugs). The cells were excited at 345 and 380 nm, and emitted light was measured at 510 nm. To calculate intracellular Ca2+ concentrations from experimental (345/380)-ratios, the following equation was used(13): R is the ratio from the cell measurements; Rmax and Rmin represent the ratios for Fura-2 in the presence of saturating and zero calcium, respectively; Kd is the dissociation constant for the Fura-2-Ca2+ complex, assumed to be 224 nM at 37°C;F0 and F1 are the fluorescence intensities at 380 nm for free and Ca2+-saturated Fura-2, respectively.Rmin and Rmax were measured using Fura-2 potassium salt dissolved in medium with 1 mM Ca2+(Rmax) or in Ca2+-free medium with 1 mM EGTA(Rmin). The background was obtained by recording the signal without any cell in the field of measurement. In pilot experiments the background values obtained in this way deviated less than 5% from the values obtained with a cell in the field and the Fura-2 signal quenched with MnCl2.
Drugs and peptides. Porcine NPY, oxymetazoline, and phenylephrine were purchased from Sigma Chemical Co.; FK 506 was a gift from Jay Luly, Abbott Labs (North Chicago, IL); A23187 was from Calbiochem (La Jolla, CA).
Statistical analysis. Values are given as mean ± SEM in the text, tables and figures. Statistical analysis was performed witht test and analysis of variance. A value of p < 0.05 was considered significant.
RESULTS
In PT from adult rats, α-adrenergic agonists as well as NPY increase the Na+ affinity of Na+,K+-ATPase but have no effect onVmax(6, 7). All studies were therefore performed at the nonsaturating Na+ concentration of 20 mM. At this Na+ concentration, Na+,K+-ATPase works at approximately 75% of its maximal rate. In this study we found that theα-adrenergic agonist oxymetazoline, 10-5 M, increased Na+,K+-ATPase to 160.6 ± 3.0% of control value(n = 3). The lowest dose of oxymetazoline significantly increased Na+,K+-ATPase in adult PT was 5 × 10-8 M. Oxymetazoline 10-7, 10-6, and 10-5 M had no significant stimulatory effect on Na+,K+-ATPase activity in infant PT(Fig. 1A).

(A and B) Effects of oxymetazoline(A) and NPY (B) on the Na+,K+-ATPase of rat PT segments from infant and adult rats. Both oxymetazoline and NPY increases PT Na+,K+-ATPase activity in a dose-dependent manner in 40-d-old rats (•). In 10-d-old rats (▪), oxymetazoline 10-8 to 10-5 M and NPY 10-8 to 10-6 M have no significant stimulatory effects. Each data point is expressed as mean ± SEM,n = 3. Measurements are done at Na+ = 20 mM. NS, not significant
In adult PT, NPY 10-8 M significantly increased Na+,K+-ATPase activity, 123.5 ± 2.7% of control(n = 3). Maximal effect was obtained with NPY 10-6 M, 201.3± 5.2% of control (n = 3). In infant PT, NPY 10-8 M to 10-6 M had no effect on Na+,K+-ATPase activity. NPY 10-5 M caused a slight increase, 112.1 ± 4.0% of control(n = 3) (Fig. 1B).
In adult rats threshold doses of oxymetazoline, 10-8 M, and NPY, 5× 10-9 M, synergistically stimulated Na+,K+-ATPase activity to 161.7 ± 0.8% of control value (n = 3). Interestingly, these low doses of oxymetazoline and NPY also had a synergistic effect on Na+,K+-ATPase in infant rats (137.5 ± 3.8% of control value, n = 3) (Fig. 2). In both adult and infant PT, the synergistic effect of oxymetazoline and NPY was completely abolished by FK 506, an inhibitor of PP2B (data not shown).

Synergic effects of oxymetazoline and NPY on PT Na+,K+-ATPase activity. Neither oxymetazoline 10-8 M nor NPY 5 × 10-9 M can stimulate PT Na+,K+-ATPase activity in itself; however, in combination they significantly increase the enzyme activity both in adult and infant rats. This stimulation is abolished in the presence of FK 506, an inhibitor of PP2B.
The calcium ionophore, A23187, also stimulates Na+,K+-ATPase in adult rat renal tubules, and the effect is abolished by FK 506(14). In this study, A23187 (10-6 M) significantly increased PT Na+,K+-ATPase activity to 139.0± 2.3% in adult rats (n = 3). In infant PT, A23187 10-7 M had little effect, whereas 10-6 M significantly increased enzyme activity (134.4 ± 2.7%, n = 3). This stimulation was abolished by FK 506 (data not shown).
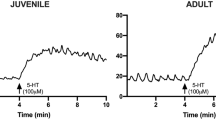
The effect of the α-adrenergic agonist phenylephrine and NPY on cytoplasmic Ca2+ in PT cells is shown in Fig. 3 and Tables 1 and 2. In the adult PT cells, theα-adrenergic agonist caused a rapid and transient increase in[Ca2+]i, and NPY caused a less pronounced, but more prolonged increase in [Ca2+]i. Higher doses of each agent were required to elicit similar responses in infant PT. When NPY andα-adrenergic agents were added simultaneously, no synergistic effect on cytoplasmic [Ca2+]i was observed. In cells that were preincubated with NPY for 30 min, the [Ca2+]i response to the α-adrenergic agonist was significantly enhanced both in adult and in infant PT cells (Fig. 3).

Representative recordings of intracellular calcium[Ca2+]i) in single PT cells after stimulation with theα-agonist phenylephrine 10-7 M and 10-5 M.[Ca2+]i was determined using Fura-2 as an intracellular Ca2+ sensor. Cells were preincubated with either NPY 10-7 M or buffer solution 30 min before they were loaded with Fura-2 and stimulated with the α-agonist. Typically, there was a considerable boost of the α-agonist induced [Ca2+]i peak in cells preincubated with NPY both in cells from young (10-d-old) and mature(40-d-old) animals.
DISCUSSION
More than 80% of the filtrate is under basal conditions, reabsorbed in the proximal tubule, which is innervated by the sympathetic nervous system. This system plays a central role for the regulation of sodium reabsorption. Denervation results in inappropriate sodium losses(15, 16), and stimulation of renal nerve activity results in sodium retention(17). This effect is abolished by α-adrenergic antagonists. Both NE and NPY are released from renal nerve endings. In the adult rat kidney, PT Na+,K+-ATPase is the target for several hormones that regulate salt metabolism(2). α-Adrenergic agonists stimulate PT Na+,K+-ATPase activity(6, 18), and this may contribute to the sodium-retaining effect that follows activation ofα-adrenergic receptors. Although NE and NPY are colocalized in renal nerve endings, and although it is well established that NE and NPY often act synergistically(7, 19–22), few studies have addressed the question of whether tubular sodium reabsorption may be regulated via an interaction between NE and NPY. The finding thatα-adrenergic agonists and NPY synergistically stimulate PT Na+,K+-ATPase activity may imply that this is the case.
In the infant kidney, oxymetazoline (an α1- andα2-adrenergic agonist) and NPY failed to stimulate Na+,K+-ATPase activity at doses which significantly stimulate the enzyme activity in 40-d-old rats. Yet very low and probably physiologic doses of NPY and an α-adrenergic agonist did, when present together, significantly stimulate PT Na+,K+-ATPase activity in infant rats. Whether renal function in the infant kidney can be modulated by a synergism between α-adrenergic receptors and NPY remains to be determined. Although NE and NPY are colocalized in sympathetic nerve endings(23), the release of NPY generally requires a higher level of renal nerve activation than the release of NE(24). Morphologic studies suggest that the ontogeny of renal nerves continues postnatally(25). It is therefore possible that the infant kidney may not be able to synchronize the release of NE and NPY in response to a situation, when there is a need to retain sodium and water.
The question why NPY and α-adrenergic agonists alone did not stimulate Na+,K+-ATPase activity remains unanswered. Developmental changes in receptor availability, the coupling between receptors and G proteins, or the intracellular transduction of the signal from activated receptors are possible explanations.
The synergistic stimulation of Na+,K+-ATPase by oxymetazoline and NPY was found to be completely abolished by the PP2B inhibitor, FK 506. Thus PP2B appears to play a similar role for the modulation of Na+,K+-ATPase activity in infant and adult kidney. In ongoing studies we have observed that PP2B is already well expressed in the kidney during fetal life (Laestadius Å, Svennilson J, Aperia A, manuscript in preparation).
Because PP2B is activated by calcium, we also tested the effect of the calcium ionophore, A23187, on Na+,K+-ATPase activity. A23187 was effective in both infant and adult rat tubules, but 10-fold higher doses of NPY and the α-adrenergic agonist were needed to elicit a[Ca2+]i response. Both α-adrenergic agonists and NPY increased [Ca2+]i, but the mechanism of action is probably different (see below). Although α-adrenergic agonists cause a transient peak in [Ca2+]i, NPY causes an increase that is more long lasting, but of lower amplitude. We measured[Ca2+]i in the whole cell, and the technique used did not allow for recordings of local accumulations of Ca2+ within the cell. It is therefore not possible to quantitatively compare the local[Ca2+]i effect on PP2B.
The effects on Na+,K+-ATPase activity were studied using tubules dissected from a collagenase perfused kidney, whereas the effects on[Ca2+]i were studied on cells in primary culture. The dose-response curves can therefore not be compared. The finding that higher doses of α-adrenergic agonists and NPY were required to elicit a response in the tubular preparation may be due to loss of receptor activity during the preparation, because high concentrations of collagenase may cause damage to the tubular basement membrane(26). It may then be argued that the infant tubules have lost more receptor activity than the adult tubules and that therefore do not respond to oxymetazoline and NPY. The finding that very low doses of NPY and oxymetazoline could synergistically stimulate Na+,K+-ATPase activity in infant rats precludes this explanation.
In an ongoing study we have found that the NPY effect on[Ca2+]i, but not the α-adrenergic effect on[Ca2+]i, was abolished when Ca2+ was removed from the medium and when the cells were preincubated with the Ca2+ channel blocker, nifedipine (Sahlgren B, Ono S, Lehman S, Zettergren E, Larsson S, manuscript in preparation) indicating that NPY increases[Ca2+]i by increasing the influx from the extracellular space and that the α-adrenergic effect is due to release of Ca2+ from the intracellular stores. The[Ca2+]i response to α-adrenergic agonists was enhanced if the PT cells were preincubated with NPY. This may be interpreted in the following way: the infant cells have a lower amount of stored Ca2+ and can therefore not respond adequately to α-adrenergic stimulation. The finding that the infant tubules required higher doses of the calcium ionophore to increase Na+,K+-ATPase activity may also imply that infant cells have a lower supply of intracellular Ca2+. Preincubation with NPY will allow the stores to be filled, resulting in an enhancement of the α-adrenergic [Ca2+]i response. This may be one of the reasons why Na+,K+-ATPase could be stimulated in the presence of both α-adrenergic agonists and NPY. Most likely there are also other factors contributing to the synergistic response of Na+,K+-ATPase to α-adrenergic agonists and NPY, such as an interaction between the receptors and/or the G proteins coupled to the receptors. The interaction between NPY and α-adrenergic receptors, which has been observed in many tissues(7, 19–22), is an area that is under intense investigation, and comparative studies in infant and adult kidneys may be a good model to further explore this interaction on a molecular level.
In conclusion, this study provides further evidence that the intracellular signaling systems in the kidney develop postnatally, and that immaturity of these systems may contribute to the poor capacity of the infant to regulate salt and fluid homeostasis.

Abbreviations
- NPY:
-
neuropeptide Y
- PT:
-
proximal tubule
- PP2B:
-
protein phosphatase 2B
- NE:
-
norepinephrine
- [Ca2+]i:
-
free intracellular calcium
- HEPES:
-
N-2-hydroxyethylpiperazine-N′-2-ethanesulfonic acid
References
Aperia A, Celsi G 1992 Ontogenic processes in nephron epithelia: structure, enzymes, and function. In: Seldin DW, Giebisch G (eds) The Kidney: Physiology and Pathophysiology, 2nd Ed. Raven Press, New York, 803–828.
Aperia A, Holtback U, Syren M-L, Svensson L-B, Fryckstedt J, Greengard P 1994 Activation/deactivation of renal Na+,K+-ATPase: a final common pathway for regulation of natriuresis. FASEB J 8: 436–439.
Aperia A, Bertorello A, Seri I 1987 Dopamine causes inhibition of Na+,K+-ATPase in rat proximal convoluted tubule segments. Am J Physiol 252:F39–F45.
Fukuda Y, Bertorello A, Aperia A 1991 Ontogeny of the regulation of Na+,K+-ATPase activity in the renal proximal tubule cell. Pediatr Res 30: 131–134.
Fryckstedt J, Svensson L-B, Linden M, Aperia A 1993 The effect of dopamine on adenylate cyclase and Na+,K+-ATPase activity in the developing rat renal cortical and medullary tubule cells. Pediatr Res 34: 308–311.
Aperia A, Ibarra F, Svensson L-B, Klee C, Greengard P 1992 Calcineurin mediates -adrenergic stimulation of Na+,K+-ATPase activity in renal tubule cells. Proc Natl Acad Sci USA 89: 7394–7397.
Ohtomo Y, Meister B, Hokfelt T, Aperia A 1994 Coexisting NPY and NE synergistically regulate renal tubular Na+,K+-ATPase activity. Kidney Int 45: 1606–1613.
Minneman KP 1988 1-Adrenergic receptor subtypes, inositol phosphates, and sources of cell Ca2+. Pharmacol Rev 40: 87–120.
Lynch JW, Vemos VS, Bucher B, Stoclet J-C, Takeda K 1994 A pertussis toxin-insensitive calcium influx mediated by neuropeptide Y2 receptors in a human neuroblastoma cell line. J Biol Chem 269: 8226–8233.
Nishi A, Eklof A-C, Bertorello AM, Aperia A 1993 Dopamine regulation of renal Na+,K+-ATPase activity is lacking in Dahl salt-sensitive rats. Hypertension 21: 767–771.
Jakobsson B, Larsson SH, Wieslander A, Aperia A 1990 Amino acid stimulation of Na,K-ATPase activity in rat proximal tubule after high-protein diet. Acta Physiol Scand 139: 9–13.
Larsson S, Aperia A, Lechene C 1986 Studies on final differentiation of rat renal proximal tubular cells in culture. Am J Physiol 251:C455–C464.
Grynkiewicz G, Poenie M, Tsien RY 1985 A new generation of Ca2+ indicators with greatly improved fluorescence properties. J Biol Chem 260: 3440–3450.
Ibarra F, Aperia A, Svensson L-B, Eklof A-C, Greengard P 1993 Bidirectional regulation of Na+,K+-ATPase activity by dopamine and -adrenergic agonist. Proc Natl Acad Sci USA 90: 21–24.
Bello-Reuss E, Colindress RE, Pastoriza-Munoz E, Mueller RA, Gottschalk CW 1975 Effects of acute unilateral denervation in the rat. J Clin Invest 56: 208–217.
Pelayo JC, Zeigler MG, Jose PA, Blantz RC 1983 Renal denervation in the rat: analysis of glomerular and proximal tubular function. Am J Physiol 244:F70–F77.
DiBona GF 1977 Neurogenic regulation of renal tubular sodium reabsorption. Am J Physiol 233:F73–F81.
Beach RE, Schwab SE, Brazy PC, Dennis VW 1987 Norepinephrine increases Na, K-ATPase and solute transport in rabbit proximal tubules. Am J Physiol 252:F215–F220.
Ekblad E, Edvinsson L, Wahlestedt C, Uddman R, Hakanson R, Sunder F 1984 Neuropeptide Y co-exists and co-operates with noradrenaline in perivascular nerve fibers. Regul Pept 8: 225–235.
Wahlestedt C, Edvinsson L, Ekblad E, Hakanson R 1985 Neuropeptide Y potentiates noradrenaline-evoked vasoconstriction: mode of action. J Pharmacol Exp Ther 234: 735–741.
Zukowska-Grojec Z, Haass M, Bayorh MA 1986 Neuropeptide Y and peptide YY mediate non-adrenergic vasoconstriction and modulate sympathetic responses in rats. Regul Pept 15: 99–110.
Wahlestedt C, Hakanson R, Vaz CA, Zukowska-Grojec Z 1990 Norepinephrine and neuropeptide Y: vasoconstrictor cooperationin vivo and in vitro. Am J Physiol 258:R736–R742.
Lundberg JM, Hokfelt T 1983 Coexistence of peptides and classical neurotransmitters. Trends Neurosci 6: 325–333.
Pernow J, Lundberg JM, Kaijser L, Hjemdahl P, Theodorsson-Norheim E, Martinsson A, Pernow B 1986 Plasma neuropeptide Y-like immunoreactivity and catecholamines during various degrees of sympathetic activation in man. Clin Physiol 6: 561–578.
Liu L, Barajas L 1993 The rat renal nerves during development. Anat Embryol 188: 345–361.
Linshaw MA, Grantham JJ 1980 Effect of collagenase and ouabain on renal cell volume in hypotonic media. Am J Physiol 238:F491–F498.
Acknowledgements
The authors thank Lill-Britt Svensson and Eivor Zettergren for technical assistance.
Author information
Authors and Affiliations
Additional information
Supported by a grant from the Swedish Medical Research Council (No. 03644)(to A.A.). Y.O. was supported by Juntendo University School of Medicine(Tokyo, Japan).
Rights and permissions
About this article
Cite this article
Ohtomo, Y., Ono, S., Sahlgren, B. et al. Maturation of Rat Renal Tubular Response to α-Adrenergic Agonists and Neuropeptide Y: A Study on the Regulation of Na+,K+-ATPase. Pediatr Res 39, 534–538 (1996). https://doi.org/10.1203/00006450-199603000-00024
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1203/00006450-199603000-00024
