
Abstract
Clinical scenario
A 54 year-old man consults about a long-standing cough: his wife encouraged him to attend as she was tired of hearing him cough all the time. He is a bit vague about when it started, but it must be ‘nearly a year’. He has consulted his usual general practitioner about the cough three times. Eight months ago he presented with a ‘chesty’ cough associated with a feverish illness and an upper respiratory tract infection; he was prescribed a course of antibiotics which he thinks might have slightly improved the cough, though it did not fully resolve. Two subsequent consultations resulted in a further course of antibiotics and a trial of a salbutamol inhaler, neither of which appear to have made any difference. The clinical notes record that his chest was ‘clear’ at each of these consultations. He describes himself as ‘generally well’, though he has been tired recently which he attributes to the long hours he is working. He smoked for about 15 years but quit in his mid-thirties.
Similar content being viewed by others

My first thoughts on hearing this man's history are that as he stopped smoking about 20 years ago his cough, which only started a year ago, is unlikely to be linked to the smoking habit. Treatment with antibiotics did not make a substantial difference to his symptom, so acute respiratory infection seems unlikely to be a cause. The case scenario refers to fatigue which the patient blames on his heavy workload but may be exacerbated by disturbed sleep due to the presence of cough. It will be important to ask more about his sense of well-being, as weight loss and general ill health might point to causes such as chronic infection or toxic conditions which are relatively common in my practice.
History
I would start by taking a history in order to gather the information that I need to make a diagnosis.1–3 I would ask some specific questions about the characteristics of the cough: is it dry or productive, was the onset sudden or gradual, what makes it better or worse (cold air, talking, eating, lying down exercise), is it worse at different times of day or night? A personal or family history of allergic conditions might suggest a diagnosis of asthma,4 though his history suggests that he has not noticed any benefit from using salbutamol.5–7 I would check to see if he was taking medication, such as β-blockers or ACE inhibitors [see Medford's perspective below], whether he has a post-nasal drip, whether there are signs or symptoms that might suggest heart failure or gastroesophageal reflux as a cause for his cough, remembering that he may have more than one cause of this chronic cough.3
Tuberculosis
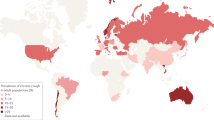
In Argentina, the incidence of tuberculosis (TB) is about 11,000 new cases per year,8 most commonly in young men, and concentrated in the provinces (such as Corrientes where I work) which have the highest rates of poverty. In the first six months of 2012 we have diagnosed 274 new cases of TB: of the four cases diagnosed in June, one 24 year-old man was also diagnosed with HIV. The percentage of co-infection with HIV-AIDS remains between 5–5.5% in Argentina.9
Our case complains of fatigue, and if I thought TB may be the cause of the chronic cough I would enquire about other symptoms such as afternoon fever, night sweats, anorexia, weakness, expectoration and weight loss.10 Each patient with respiratory symptoms who has cough and expectoration for more than 15 days should be investigated to rule out TB, but there are still patients who wander from one doctor to another resulting in a wrong diagnosis or delays in treatment.
Confirming a diagnosis of HIV is relatively easy, but TB is more complicated. Obtaining a sputum sample in a patient who is malnourished, dehydrated and uncooperative can be difficult, particularly when diagnostic tests are not performed at the Primary Care Centre. To investigate a patient with a productive cough, I would need to arrange two smears of sputum, and a chest radiograph. We cannot analyse the smear, nor do we have local radiography, which means that the patient would have to make two round trips to the hospital. At two Argentinian pesos for each ticket, the total expenditure on four journeys is equivalent to the cost of 2 kg of bread. Primary care does not receive direct funding from the National Programs of TB, only medication for its treatment.
If TB is confirmed, the patient is referred to the hospital to be put under the TB-Program and provided with medication which would be monitored in primary care. The Health Agents or Promoters of Health who administer DOTS (Directly Observed Treatment, Short-course) undertake their essential task with admirable devotion, assuming a co-responsibility with the patient to ensure treatment compliance.11
Environmental causes
The conditions in which people live and work may be important as a cause of cough.
Occupational exposure to pollution in Argentina is not controlled, especially in small factories. For example, in some poor neighbourhoods, families are installing municipality-funded brick kilns in the courtyard of their houses in order to earn enough money to survive. Increasingly we are seeing people suffering the effects of smoke given off by this kind of ‘family factory’.12,13 Additional risk factors are poor families with many children, poor housing, damp, unheated homes, people who do not have social security coverage, high rates of illiteracy, and alcoholism. Usually these are peripheral neighbourhoods of unplanned urbanisation, and sanitation is poor — adding yet another cause of pollution as small piles of garbage are often burned outside each home because there is no regular collection.
Investigations, empirical treatment and follow-up
In primary care I can arrange blood tests (for example to look for infection or eosinophilia) and arrange a CXR to help diagnose conditions such as TB, interstitial lung disease, lung cancer, or heart failure. If these tests do not confirm a specific diagnosis which can be treated, based on the history I would start empirical treatment for postnasal drip, gastro-oesophageal reflux,14 or asthma, and review the patient after four to six weeks to find out if symptoms have improved.15 If the patient has not improved and the diagnosis is still not clear I would refer to the pulmonologist for further investigations such as spirometry or bronchoscopy.
The primary care context
Primary Care Centres offer free consultation and medicines, though demand is high. Patients with health insurance also use these services increasing the expenditure of resources. There is a need to standardise the use of clinical guidelines in primary care; although there are national guidelines for the management of TB and HIV-TB co-infection,10,16 the guidelines for asthma and COPD are not standardised, thus leading to considerable variation in practice. Healthcare professionals are often distracted from their clinical role by having to engage in addressing the deprivation, economic and psychosocial situation of the patients.13 Access to health services is acceptable, but often the people who most need care are the least demanding and the health team may need to go in search of them.17
References
Irwin RS, Curley FJ, French CL . Chronic cough. The spectrum and frequency of causes, key components of the diagnostic evaluation, and outcome of specific therapy. Am Rev Respir Dis 1990;141:640–7. http://dx.doi.org/10.1164/ajrccm/141.3.640
Irwin RS, Rosen JM, Braman SS . Cough: a comprehensive review. Arch Intern Med 1977;137:1186–91. http://dx.doi.org/10.1001/archinte.1977.03630210060019
Irwin RS, Boulet LP, Cloutier MM et al. Managing Cough as a defense mechanism and as a symptom. A consensus panel report of the American College of Chest Physicians. Chest 1998;114:133–81. http://dx.doi.org/10.1378/chest.114.2_Supplement.133S
Strass MD, Ardusso LRF, Crisci CD . Prevalencia de sensibilidad a aeroalergenos en pacientes con rinitis y/o asma en el sur de Misiones y noreste de Corrientes, Argentina. Archivos Alerg Inmunol Clin 2002;33:47–5.
British Thoracic Society/Scottish Intercollegiate Guideline Network. British Asthma Guidelines. Thorax 2008;63(Suppl 4):1–121. Updated June 2009 http://www.brit-thoracic.org.uk (accessed April 2010)
Global Initiative for Asthma (GINA). The Global Strategy for Asthma Management and Prevention, Updated 2011. Available from: http://www.ginasthma.org (accessed July 2012)
Roncoroni AJ, Abbate E, Figueroa Casas JC, et al. Normas para el tratamiento del asma bronquial. Medicina (Buenos Aires) 1993;53:249–59.
US Global Health Policy. Data by Country: Argentina. Available from http://globalhealth.kff.org (accessed July 2012)
UNAIDS. AIDSinfo country factsheets available from http://www.unaids.org/en/dataanalysis/tools/aidsinfo/countryfactsheets/ (accessed July 2012)
Abbate EH, Palmero DJ, Castagnino J, et al. Tratamiento de la tuberculosis: Guía práctica elaborada por la Sección Tuberculosis, Asociación Argentina de Medicina Respiratoria. Medicina (B. Aires) 2007;67:295–305.
World Health Organization. Implementing the Stop TB Strategy. A Handbook for National Tuberculosis Control Programmes. WGO; Geneva. 2008
Godoy Emilio . Latin America: Brick-Making Industry Confronts Its Climate Impacts. Inter Press Service News Agency available from http://www.ipsnews.net/2011/03/latin-america-brick-making-industry-confronts-its-climate-impacts/ (accessed July 2012)
Guttikunda S . Impact Analysis of Brick Kilns on the Air Quality in Dhaka, Bangladesh. SIM-air working paper 21. 2009 http://www.urbanemissions.info/sim-series-21.html (accessed August 2012)
Marzo M, Alonso P, Bonfill X, et al. Guía de práctica clínica sobre el manejo del paciente con enfermedad por reflujo gastroesofágico (ERGE). Gastroenterol Hepatol 2002;25:85–110.
Baena EM, Rodríguez EP, Esteban JJ . Manual de Actuación en Patología Respiratoria. Available from http://neumomadrid.org/images/upload/manual%20de%20actuaci%C3%B3n%20de%20patolog%C3%ADa%20respiratoria.pdf#page=89. (accessed July 2012)
World Health Organization. Tuberculosis. available from http://www.who.int/topics/tuberculosis/en/ (accessed August 2012)
Hart T . The inverse care law. Lancet 1971;1:405–12. http://dx.doi.org/10.1016/S0140-6736(71)92410-X
Acknowledgements
Handling editor Hilary Pinnock
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The author declares that there are no conflicts of interest in relation to this article.
Rights and permissions
About this article
Cite this article
Fiori, L. A 54 year-old man with a chronic cough — A primary care perspective from Argentina. Prim Care Respir J 21, 344–345 (2012). https://doi.org/10.4104/pcrj.2012.00076
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.4104/pcrj.2012.00076
