
Abstract
Coronary artery disease is associated with multiple genetic and environmental risk factors. In this study, we evaluated the correlation of angiotensin l-converting enzyme (ACE) (I/D) and ApoE gene polymorphisms (E2, E3, E4 and g.-219G/T) with myocardial perfusion. We examined 410 patients using exercise–rest myocardial perfusion single photon emission computed tomography (SPECT), in which the summed stress score (SSS), summed rest score (SRS) and summed difference score (SDS) indexes were calculated. Homozygotes for the ACE D allele had greater mean values of SSS (P<0.001) and SDS (P<0.001). In addition, E3 homozygotes, E4 heterozygotes and E4 homozygotes had significantly higher values of SSS and SDS compared with E3 heterozygotes (P<0.001); E4 homozygotes had significantly higher values of SSS and SDS compared with E3 homozygotes. Furthermore, for the g.-219G>T polymorphic site at the promoter region of ApoE gene, the mean values of SSS and SDS were significantly higher for T heterozygotes/homozygotes than for GG homozygotes. Adjusting for all demographic and clinical data using multiple linear regression analysis it was found that ACE D and both ApoE genotypes were independent predictors with a cumulative contribution for the prediction of SSS and SDS. Furthermore, logistic regression analysis revealed that all three genotypes had an independent predictive ability for abnormal SSS (SSS>2). These data provide the first evidence of an association and significant cumulative contribution of the aforementioned genotypes in myocardial perfusion with E4 allele having the strongest association followed by ACE D and ApoE g.-219T alleles.
Similar content being viewed by others
Introduction
Coronary artery disease (CAD) and its severe complications are leading causes of disability and death in the developed world.1 CAD is a chronic disease caused by multiple genetic and environmental risk factors, such as cigarette smoking, stress and a sedentary lifestyle.2, 3 Specific genetic causes for CAD have been identified in members of families affected by monogenetic forms of hypercholesterolemia, such as familial hypercholesterolemia.4 However, in the general population, the multifactorial etiology of CAD is not fully understood.5 The cumulative effects of both genetic and environmental factors have been the focus of recent attention.6 However, the major challenge confronting researchers is to identify the predominant genetic factor and determine how the environmental factor modulates the expression of candidate genes associated with risk for atherosclerosis and CAD.
Several studies have shown an association between CAD and polymorphisms in genes related to the control of blood pressure and lipid metabolism, like angiotensin l-converting enzyme (ACE) and apolipoprotein E (ApoE). Angiotensin II, a very potent vasoconstrictor, is generated by the angiotensin I-converting enzyme (ACE). ACE expression is associated with a deletion (D)/insertion (I) polymorphism in intron 16 of the ACE gene. The D allele was recognized as being associated with high ACE activity in the plasma, increased blood pressure and myocardial infarction risk. There is compelling evidence of an association between variation in the ApoE gene, and risk and severity of coronary artery disease (CAD) and Alzheimer's disease. The E2/E3/E4 polymorphism in the coding region of the gene has been studied extensively, with the E4 allele consistently found to be associated with increased risk of these diseases. The E2, E3 and E4 alleles, respectively, encode the apoE2, apoE3 and apoE4 isoforms that differ in amino-acid sequence at residues 112 and 158, with the E2 isoform having a cysteine at both sites, the E3 isoform having a cysteine and an arginine, respectively, and the E4 isoform possessing an arginine at both residues. However, these results have not been consistent6 and they have never been associated with myocardial perfusion scintigraphy, the only widely available method of assessing myocardial perfusion directly. Myocardial single photon emission tomography (SPECT) is a well established method for the realistic approach of myocardial perfusion. The diagnostic and prognostic value of this method has already been extensively reported previously.7 On the basis of these considerations, we designed a study, specifically aiming to evaluate the effect of ACE (I/D) and the E2/E3/E4 polymorphism in the coding region of the ApoE gene as well as the functional polymorphism (g.-219G>T) in the promoter of the ApoE gene on myocardial perfusion by focusing on the correlation with myocardial SPECT imaging in a large number of Greek patients. ApoE has a key role in lipoprotein metabolism working as a receptor ligand for the uptake of lipoproteins from circulation, which has been proposed as a risk factor for cardiovascular events.8 The apoE-encoding gene (ApoE) has a common Hhal polymorphism located in exon 4 that results in three alleles: ɛ2, ɛ3 and ɛ4. Moreover, several polymorphisms in the promoter of the gene have also been identified, and it has been shown that the g.-219G>T polymorphism exerts an allele-specific effect on ApoE expression such that the T allelic promoter has a lower transcriptional activity than the G allelic promoter.9 Previous studies have shown an association of ApoE gene polymorphisms with variation serum concentrations, hypertension and risk of myocardial infarction.10, 11 Our results show the first evidence of an association of ACE and ApoE polymorphisms with myocardial perfusion and suggest that the proposed effect of the abovementioned polymorphisms may have important influence on early patient risk stratification.
Materials and methods
Study subjects
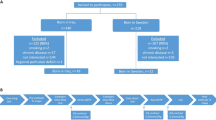
The study cohort consisted of 410 patients (271 men and 139 women) mostly from Central Greece, ranging in age from 40 to 87 years (mean age 61.4±10.3 years). In total, 904 patients were referred between March 2005 and February 2007 for a symptom-limited exercise testing combined with a SPECT myocardial perfusion imaging, to evaluate known or suspected CAD and stratify patient risk (Table 1). Fifty one of these patients (13%) had previously determined CAD, according to a previous angiography (13 had single-vessel disease, 22 had two-vessel disease and 16 had three-vessel disease).
In our study, we excluded patients younger than 40 years, pregnant women and patients whose myocardial perfusion imaging might have been affected by factors other than myocardial ischemia. We, therefore, excluded patients with left bundle branch block, cardiomyopathy and those patients with an implanted pacemaker. We also excluded patients with a previous cardiac surgery (bypass grafting or angioplasty), those with contraindication to or inability to perform treadmill testing, or to achieve a satisfactory exercise level because of an exocardiac condition and patients taking digoxin (due to it's prolonged effect). Moreover, we excluded patients with a history or other evidence of myocardial infraction, as they comprise an inhomogeneous group whose myocardial perfusion study is affected not only by myocardial ischemia but also by necrosis related to both episode severity and applied therapy. However, 502 patients were excluded from the study because they did not meet the inclusion criteria, whereas 32 patients refused to participate in the study.
Medications (β-blockers, calcium channel antagonists and nitrates) that could possibly influence patient performance on exercise testing and the related variables were temporarily withdrawn (for approximately five half-lives), as described previously.12, 13
Before testing, all patients gave informed consent for their complete participation according to the Hospital Ethical Committee, which approved this study, and the ethical standards laid down in the 1964 Declaration of Helsinki, and a brief structured interview from which we obtained data on symptoms, medications, previous cardiac events, coronary risk factors and cardiac or non-cardiac diagnoses.
Hypertension was defined as a condition with systolic blood pressure of 140 mm Hg or greater at rest and/or a diastolic blood pressure of 90 mm Hg or greater at rest, or treatment with antihypertensive medicines. Diagnoses of diabetes mellitus and lipid disorders were derived from the interviews with the patients and the use of corresponding medications. Obesity was considered as a condition with body mass index (BMI calculated as weight in kilograms divided by height in meters squared) value of 30.0 or greater.
Genetic analysis
Genomic DNA was extracted from peripheral blood leukocytes using the salting-out method.14 ACE I/D polymorphism genotyping was carried out by polymerase chain reaction (PCR), as previously described.15 Each DD genotype was confirmed through a second PCR with primers specific for the insertion sequence.16 The ApoE gene polymorphism (E2/E3/E4) was detected by PCR with primer sequences derived from the procedure used by Hixson and Vernier.17 Moreover, these substitutions in the ACE and ApoE genes were analyzed, according to the CVD StripAssay (ViennaLab, Vienna, Austria). For the g.-219 G/T polymorphic site, a DNA fragment, containing this site, was amplified using PCR primers 5′-AGAATGGAGGAGGGTGCCTG-3′ (FW) and 5′-ACTCAAGGATCCCAGACTTG-3′ (RV), followed by digestion with the BstNI restriction enzyme and gel electrophoresis.
Exercise testing
After discontinuing cardioactive medication, a 12-h fasting and avoiding smoking or engaging in heavy physical activity for, at least, 3 h before the examination, the patients underwent a symptom-limited treadmill exercise testing (Bruce protocol), as described previously.13 Data on symptoms and estimated workload in metabolic equivalents—METs (using standard tables) were obtained.18
SPECT myocardial perfusion imaging
Myocardial perfusion studies were carried out using thallium-201 (Tl-201) or technetium-99m (Tc-99m) tetrofosmin (Myoview, Amersham Health, Arlington Heights, IL, USA).7, 12, 13 Acquisition and processing protocols used in our department of Nuclear Medicine for Tl-201 and Tc-99m-tetrofosmin SPECT studies have been described in detail elsewhere, according to EANM/ESC procedural guidelines.12, 13 In the unprocessed anterior projection image of Tl-201 studies, acquired as part of the initial imaging process, the lung/heart ratio (LHR) of Tl-201 activity was measured, as described in a previous report, and values <0.55 were considered to be normal.19
We carried out polar and three-dimensional mapping in all studies (with Tl-201 or Tc-99m tetrofosmin) and calculated the transient ischemic dilation (TID) index (Sopha medical Vision software), which is determined as an index of the pathologic dilation of the left ventricle at stress, as compared with rest (normal values <1.2). Both the LHR and TID indexes are considered to be indexes of severe myocardial ischemia.12 For SPECT interpretation, the myocardium of the left ventricle was divided into 17 segments, according to previous reports.20, 21 Two independent experienced observers blindly evaluated the reconstructed images, the polar maps and the three-dimensional images of both stress and rest studies by scoring the radiotracer uptake in each of the 17 regions, using a 5-point scoring system (0: normal uptake; 1: mildly reduced uptake; 2: moderately reduced uptake; 3: severely reduced uptake and 4: no uptake).20, 21
In 12 studies (5.8%) in which discordance between the two observers was detected (difference >2 in SSS and/or SRS values), the view of a third observer was requested and the disagreement was resolved by consensus.13, 19, 20 Ischemia was considered in every region of the myocardium with an uptake higher than 0 at stress imaging and a reduction of the score by, at least, one unit at rest. Finally, the ‘summed stress score’ (SSS) and ‘summed rest score’ (SRS) were obtained by adding the scores of the regions in stress and rest studies. Subsequently, a ‘summed difference score’ (SDS) was estimated by subtracting the SRS from the SSS to assess defect reversibility.13, 19, 20, 21
Studies with an SSS value equal or <2 were considered normal, an SSS value of 3–8 was considered mildly abnormal, a score of 9–13 moderately abnormal and an SSS>13 was considered severely abnormal.22
Statistical analysis
Continuous variables are presented as mean±s.d. Student's t-test was used for the comparison of proportions and of the mean values of SSS and SDS between two groups, respectively. Analysis of variance (ANOVA) was used for the comparison of SSS and SDS values between three genotypes groups. Bonferroni correction was carried out to control for multiple testing.
To explore the independent association of genotypes with SPECT variables, TID index and LHR after adjusting for age, sex, smoking, the presence of chest pain, diabetes, hypertension, obesity, lipid disorder, the use or non-use of cardioactive medications (β-blockers, calcium channel antagonists and nitrates), exercise duration, maximal systolic blood pressure, maximal heart-rate, METs, double product, angina and abnormal ST response during exercise testing, linear regression models were carried out. Regression coefficients with their s.e. and coefficients of determination of the models (adjusted R2) are presented from the results of the linear regression analysis. Multiple logistic regression analysis was also carried out to evaluate the independent association of genotypes with SSS>2. Adjusted odds ratios with 95% confidence intervals were computed from the results of logistic regression analyses. For all regression analyses two models were carried out. The first model (model 1) contained genotypes as categorical variables and comparisons between different categories were made. The second model (model 2) contained genotypes as continuous variables to explore the existence of a gene dose effect on the outcomes (genotypes were ranked as follows: ACE D: I/I=1, I/D=2 and D/D=3; ApoE: E2/E2=1, E2/E3=2, E3/E3=3, E2/E4=4, E3/E4=5, E4/E4=6 and ApoE g.-219: GG=1, GT=2, TT=3). All reported P-values are two-tailed. Statistical significance was set at P<0.05 and analyses were conducted using SPSS statistical software (version 13.0).
Results
The study population consisted of 410 patients (mean age 61.4±10.3 years, range 40–87). The demographic and clinical characteristics of the study group are shown in Table 1.
Three hundred and eight patients (75%) underwent myocardial SPECT imaging using Tl-201 and 102 patients (25%), especially obese patients or women with large breasts, were studied using Tc-99 m tetrofosmin, to minimize the effect of soft-tissue attenuation artefacts.
Two hundred and seventy-seven (67.6%) out of the 410 patients had an abnormal myocardial perfusion SPECT (SSS>2). Specifically, 179 patients (43.7%) had a mildly abnormal SPECT study (SSS: 3–8), 53 patients (12.9%) had a moderately abnormal study (SSS: 9–13) and 45 patients (11%) had a severely abnormal study (SSS>13). In addition, 88 patients (21.5%) had an abnormal TID index, whereas 55 patients (17.9%) out of the 308 who were examined using Tl-201 had an abnormal LHR value.
The allele frequencies were D=0.59, I=0.41 for ACE polymorphism, ɛ2=0.17, ɛ3=0.73, ɛ4=0.10 and g.-219G=0.55, g.-219T=0.45 for the coding region and the promoter of ApoÅ gene polymorphisms, respectively. The ACE I/D genotype distribution was 37.6, 43.9 and 18.5% for D/D, I/D and I/I, respectively. The overall distributions of ApoE genotypes E2/E2, E2/E3, E3/E3, E2/E4, E3/E4, E4/E4 in our individuals were 0.5, 26.1, 54.4, 6.6, 12, 0.5%, respectively. The E4 allele was present in 78 (19.1%) patients. Regarding the ApoE g.-219 G/T genotype, distribution was 27.8, 53.4 and 18.8% for g.-219G/G, g.-219G/T and g.-219T/T, respectively. Table 2 presents the number of patients with the aforementioned genotypes according to SSS values.
Homozygotes but not heterozygotes for the ACE D had greater mean values of SSS compared with homozygotes for the ACE I allele (8.4±6.2 vs 3.5±4.1, P<0.001 and 3.4±3.2 vs 3.5±4.1, P>0.999, Figure 1) and SDS (7.4±5.8 vs 2.9±3.4, P<0.001 and 3.0±2.8 vs 2.9±3.4, P>0.999). The mean values of SSS were 2.6±2.4, 5.2±4.5, 9.5±7.2 for E3 heterozygotes (E3/E2), E3 homozygotes and E4 heterozygotes (E4/E2, E4/E3)/homozygotes (E4/E4), respectively (Figure 2a). The mean values of SDS were 2.2±2.1, 4.4±3.7, 8.9±7.1 for E3/E2 heterozygotes, E3 homozygotes and E4 heterozygotes (E4/E2, E4/E3)/homozygotes (E4/E4), respectively. E3 homozygotes and E4 homozygotes or heterozygotes (E4/E2, E4/E3) had significant greater values of SSS and SDS compared with E3/E2 heterozygotes (ANOVA, P<0.001 after Bonferroni correction for all comparisons). In addition, E4 homozygotes had significantly greater values of SSS and SDS compared with E3 homozygotes (ANOVA, P<0.001 after Bonferroni correction for all comparisons). Regarding ApoE g.-219G/T genotypes, the mean values of SSS were 3.0±3.5, 5.0±3.8, 9.9±7.7 for homozygotes for the g.-219G allele, heterozygotes and homozygotes for the g.-219T allele, respectively (P<0.001 for all comparisons) (Figure 2b). The mean values of SDS were 2.5±2.9, 4.3±3.5, 8.7±7.3 for homozygotes for the g.-219G allele, heterozygotes and homozygotes for the g.-219T allele, respectively (P<0.001 for all comparisons).

Mean values and 95% confidence intervals of summed stress score (SSS) according to the presence of the angiotensin I-converting enzyme (ACE) D allele.

Mean values and 95% confidence intervals of summed stress score (SSS) according to the presence of the ApoE E3 and E4 alleles (a) and the ApoE g.-219G/T alleles (b).
To examine the independent predictive ability of genotypes on SSS and SDS multiple linear regression models were used. Adjusting the analysis for age, sex, smoking, the presence of chest pain, diabetes, hypertension, obesity, lipid disorder, the use or non-use of cardioactive medications (β-blockers, calcium channel antagonists and nitrates), exercise duration, maximal systolic blood pressure, maximal heart-rate, METs, double product, angina and abnormal ST response during exercise testing, the three genotypes were significantly associated with SSS and SDS. Results from multiple analyses are presented in Table 3.
ACE D, ApoE and ApoE g.-219 genotypes were found to be independent predictors of SSS and SDS. E3 homozygotes and E4 homozygotes or heterozygotes (E4/E2, E4/E3) had significant greater values of SSS compared with E3/E2 heterozygotes, with E4 allele revealing the strongest association (standardized regression coefficient is 0.48 for SSS and 0.52 for SDS). An increase in adjusted R2 was found when genotypes were simultaneously added to the regression model revealing the significant cumulative contribution of the aforementioned genotypes for the prediction of SSS and SDS. The results were similar, when ACE D, ApoE and ApoE g.-219 genotypes were treated as continuous variables in the model to explore any gene dose effect on SSS and SDS (Table 3). Ranking the ACE D, Apo E and ApoE g.-219 genotypes as follows: ACE D: I/I=1, I/D=2 and D/D=3; ApoE: E2/E2=1, E2/E3=2, E3/E3=3, E2/E4=4, E3/E4=5, E4/E4=6 and ApoE g.-219G/G=1, g.-219G/T=2, g.-219T/T=3, it was found an additive effect with SSS and SDS. Apo E had the strongest association, as defined from the standardized regression coefficients, followed by ACE D and ApoE g.-219 genotypes.
The association of TID index and LHR with the ACE D, Apo E and ApoE g.-219 genotypes was also explored (Table 4) using multiple regression analysis. All genotypes were found to be independent predictors of TID index and LHR. Similar to SPECT variables, Apo E had the strongest association following by ACE D and ApoE g.-219 genotypes. The genotypes had an addictive contribution in the prognosis of TID index and LHR as defined from the adjusted R2. Ranking the ACE D, Apo E and ApoE g.-219 genotypes by their relative risk an addictive effect on TID index and LHR was found (model 2 in Table 4).
The independent predictive ability of ACE D, Apo E and ApoE g.-219 genotypes on abnormal SSS was investigated using logistic regression analysis adjusted for all demographic and clinical data (Table 5). All genotypes were found to be independent predictors for SSS>2. ACE D homozygotes were 17.92 times more likely to have abnormal SSS. E3 homozygotes and E4 homozygotes or heterozygotes (E4/E3, E4/E2) had 8.26 and 35.80 times greater likelihood for abnormal SSS, respectively, compared with E3/E2 heterozygotes. Furthermore, g.-219T heterozygotes and homozygotes had 2.17 and 5.81 times greater likelihood for abnormal SSS, respectively, compared with g.-219G homozygotes. Furthermore, an increase in the rank categories of genotypes (according to their relative risk) was found to be associated with an increase in the odds of having abnormal SSS (model 2 in Table 5).
Discussion
Cardiovascular disease is one of the leading causes of mortality in the world.23 CAD has a multifactor etiology resulting from the interaction of genetic predisposition and environmental risk factors. Myocardial perfusion scintigraphy is the only widely available method of assessing myocardial perfusion directly, and a large body of reports supports its evidence in the diagnosis of myocardial ischemia and necrosis. Although the anatomical extent of CAD is shown by coronary angiography, myocardial perfusion SPECT imaging provides information on important features, such as endothelial function, small vessel function and collateralization, in addition to the hemodynamic significance of epicardial stenosis. This is the main reason for the strong power of myocardial SPECT in predicting coronary events, whereas the method is of proved independent and incremental prognostic value even after clinical assessment, exercise electrocardiography and coronary angiography.1, 7, 24
In this study, we investigated the influence of ACE and ApoE polymorphisms on myocardial perfusion by evaluating the corresponding SPECT variables, SSS, SDS, TID and LHR. No previous reports have investigated the role of genetic factors on myocardial perfusion and association with SPECT studies. Our results show a significant correlation among the ACE I/D genotype and the aforementioned myocardial SPECT variables. The ACE D allele had an increased prevalence in heterozygosity or homozygosity in our study group with abnormal myocardial perfusion SPECT (SSS>2). More specifically, the majority of patients with a moderate to abnormal SPECT study (SSS⩾9) were homozygous for D allele, whereas the distribution of I/I and I/D was equal.
ACE has an important function in blood pressure regulation, in the progression of atherosclerosis and its clinical manifestations which may affect the myocardial perfusion and the risk of developing coronary disease.25 In previous studies, ACE I/D polymorphism was associated with an increased risk for cardiovascular disease in genetically homogenous populations,26 although other studies have failed to detect associations between ACE polymorphism and CAD or myocardial infraction.27, 28 The D allele was recognized as being associated with high ACE activity in plasma, increased blood pressure and increased risk of plaque rupture in many different populations.29, 30 Our results are consistent with these findings according to which the presence of ACE D/D genotype may modify the myocardial perfusion promoting an increase of cardiovascular events. These findings show the importance of studying ACE polymorphism in correlation to myocardial perfusion values.
Numerous studies in different populations have shown that ApoE polymorphisms are a major determinant of individual susceptibility to CAD,31, 32 although there are other studies in which the allelic and/or genotypic impact of ApoE polymorphism has been shown to have variable significance in terms of predicting the risk of vascular events.33, 34, 35, 36 In our study, almost all patients carrying the ɛ4 allele had an abnormal myocardial perfusion SPECT (SSS>2). The subjects with ApoE E3/E3 and E3/E4 genotypes were prevalent (86.8%) among those with moderately and severely abnormal SPECT study (SSS⩾9). In addition, the genotype E4/E4 was present only in those with severely abnormal SPECT study in contrast to its absence from the individuals with moderate abnormal SPECT values. The distribution of ɛ3 allele was similar between those with normal and abnormal SSS value, whereas ɛ2 and ɛ4 allelic frequencies were higher in those with SSS value⩽2 and ⩾9 (P<0.001), respectively. ApoE has a key role in lipoprotein metabolism working as a receptor ligand for the uptake of lipoproteins from circulation, which has been proposed as a risk factor for cardiovascular events.8 The ApoE gene has a common Hhal polymorphism located in exon 4 that results in three alleles: ɛ2, ɛ3 and ɛ4. Previous studies have shown an association of ApoE gene polymorphisms with variation serum concentrations, hypertension and risk of myocardial infarction.10, 11 It has been shown that individuals with the ɛ2 allele had lower risk of myocardial infarction and higher in ɛ4 carriers, with a decrease of ɛ4 allele frequency across the countries from Northern to Southern Europe, which follows the gradient of coronary heart disease mortality rates.11, 37 These results are consistent with the findings from this study in which the ɛ4 allele and its genotypes have priority among patients with moderate and severe abnormal myocardial perfusion.
Further studies on the promoter region of the ApoE gene have reported three polymorphisms (g.-219G/T, g.-427C/T and g.-491A/T).9, 38 Of these three promoter polymorphisms, the g.-219G/T has the strongest effect on ApoE gene expression as shown by in vitro reporter assays and measurements of ApoE mRNA levels in ex vivo brain tissues from patients with Alzheimer's disease.39 Our results showed that the presence of g.-219 T allele in heterozygosity or homozygosity was significantly associated with higher SSS values; although the presence of g.-219T allele contributed to a lesser extent compared with the patients with moderate and severe abnormal myocardial perfusion, it could be proposed as a genetic factor contributing to cardiovascular risk.
Epidemiologic studies have established that multiple risk factors increase the probability of cardiovascular events because cardiovascular risk factors tend to be additive in influencing morbidity and mortality rates. There is still an open question for the quantitative estimation of the independent contribution of genetic factors opposed to environmental factors on cardiovascular risk.
In this study, we showed the association of specific polymorphisms (ACE and ApoE) with characteristics of the exercise SPECT myocardial perfusion imaging, a well-established technique for the diagnosis of CAD (identifying myocardial ischemia and necrosis) and patients' risk stratification. Myocardial perfusion SPECT imaging is considered as an autonomous valuable method for patients' prognosis, with an incremental prognostic value even above coronary angiography. Thus, we have not used myocardial SPECT as a substitute of coronary angiography, but as an independent functional investigation of myocardial perfusion, focusing on an ‘ischemic’ than an ‘anatomical’ approach to coronary atherosclerosis, regardless the pathogeneses of perfusion alteration (stenoses of the main coronary arteries, microvessels' disease and endothelial dysfunction). In recent years it has become evident that the detection of ischemia, and its extent and severity makes an important contribution to prognosis, independent of the status of the coronary anatomy.40 In addition, the calculation of SSS, SRS and SDS parameters, comprises the only widely accepted quantitative method for the myocardial SPECT interpretation and an objective evaluation of myocardial perfusion, with a reported diagnostic and prognostic value.12 SSS reflects the severity of a perfusion defect at stress, which is related to ischemia severity (in patients without myocardial necrosis), whereas SDS is a marker of defect reversibility which could reflect the improvement of myocardial perfusion at rest.
Our study has some potential limitations. First, few patients were subjected to coronary angiography, and therefore the direct correlation of the genotypes with the presence and severity of CAD was not possible. In addition, we have not included data of patients' longitudinal follow up, as this was beyond the aim of our study, although our study shows that genetic profile is significantly associated with other well-established exercise testing and primarily myocardial scanning prognostic parameters. Finally, we have not included a separate control population in our study, for ethical reasons, as it is not accepted to perform a myocardial SPECT examination without a clinical indication. However, we have considered as reference group the subgroup of the included population with normal myocardial perfusion imaging.
In essence, our study underlines the remarkable influence of ACE and ApoE gene polymorphisms on myocardial perfusion. The independent predictive ability of the genotypes under investigation with the SPECT outcome as derived from multiple analyses could eventually be a useful implication for future research with experimental designs. The analysis of the genotype can improve the quality of medical care through identification of the predisposition to disease and through preventive intervention, mainly risk factors' modulation, in patients with premature manifestation of the disease.
References
Murray, C. J & Lopez, A. D. Alternative projections of mortality and disability by cause 1990–2020: global burden of disease study. Lancet 349, 1498–1504 (1997).
Wilson, P. W. & Evans, J. C. Coronary artery disease prediction. Am. J. Hypertens. 6, 309S–313S (1993).
Galton, D. J. Genetic determinants of atherosclerosis-related dyslipidemias and their clinical implications. Clin. Chim. Acta. 257, 181–197 (1997).
Goldstein, J. L. & Brown, M. S. The cholesterol quartet. Science 292, 1310–1312 (2001).
Winkelmann, B. R. & Hager, J. Genetic variation in coronary heart disease and myocardial infarction methodological overview and clinical evidence. Pharmacogenomics 1, 73–94 (2000).
Doevendans, P. A., Jukema, W., Spiering, W., Defesche, J. C. & Kastelein, J. J. Molecular genetics and gene expression in atherosclerosis. Int. J. Cardiol. 80, 105–106 (2001).
Russell, R. R. & Zaret, L. B. Nuclear Cardiology: present and future. Curr. Probl. Cardiol. 31, 557–629 (2006).
Mahley, R. W. & Rall, S. C. Apolipoprotein E: far more than a lipid transport protein. Annu. Rev. Genomics Hum. Genet. 1, 507–537 (2000).
Lambert, J. C., Pasquier, F., Cottel, D., Frigard, B., Amouyel, P. & Chartier-Harlin, M. C. A new polymorphism in the ApoE promoter associated with risk of developing Alzheimer's disease. Hum. Mol. Genet. 7, 533–540 (1998).
Eichner, J. E., Kuller, L. H., Orchard, T. J., Gradits, G. A., McCallum, L. M., Ferrell, R. E. et al. Relation of apolipoprotein E phenotype to myocardial infarction and mortality from coronary artery disease. Am. J. Cardiol. 71, 160–165 (1993).
Sakuma, T., Hirata, R. D. & Hirata, M. H. Five polymorphisms in gene candidates for cardiovascular disease in Afro–Brazilian individuals. J. Clin. Lab. Anal. 18, 309–316 (2004).
Hesse, B., Tägil, K., Cuocolo, A., Anagnostopoulos, C., Bardies, M., Bax, J. et al. EANM/ESC procedural guidelines for myocardial perfusion imaging in nuclear cardiology. Eur. J. Nucl. Med. 32, 855–897 (2005).
Georgoulias, P., Demakopoulos, N., Orfanakis, A., Xydis, K., Xaplanteris, P., Vardas, P. et al. Evaluation of abnormal heart-rate recovery after exercise testing in patients with diabetes mellitus: correlation with myocardial SPECT and chronotropic parameters. Nucl. Med. Commun. 28, 165–171 (2007).
Miller, S. A., Dykes, D. D. & Polesky, H. F. A simple salting out procedure for extracting DNA from human nucleated cells. Nucleic Acids. Res. 16, 1215–1216 (1988).
Rigat, B., Hubert, C., Corvol, P. & Soubrier, F. PCR detection of the insertion/deletion polymorphism of the human angiotensin converting enzyme gene (DCP1) (dipeptidyl carboxypeptidase 1). Nucleic Acids. Res. 20, 1433–1438 (1992).
Shanmugam, V., Sell, K. W. & Saha, B. K. Mistyping ACE heterozygotes. PCR Methods Appl. 3, 120–121 (1993).
Hixson, J. E. & Vernier, D. T. Restriction isotyping of human apolipoprotein E by gene amplification and cleavage with HhaI. J. Lipid Res. 31, 545–548 (1990).
Fletcher, G. F., Balady, G., Froelicher, V. F., Hartley, L. H., Haskell, W. L. & Pollock, M. L. Exercise standards. A statement for healthcare professionals from the American Heart Association Writing Group. Circulation 91, 580–615 (1995).
Georgoulias, P., Orfanakis, A., Demakopoulos, N., Xaplanteris, P., Mortzos, G., Vardas, P. et al. Abnormal heart rate recovery immediately after treadmill testing: correlation with clinical, exercise testing, and myocardial perfusion parameters. J. Nucl. Cardiol. 10, 498–505 (2003).
Kapur, A., Latus, K. A., Davies, G., Dhawan, R. T., Eastick, S., Jarrit, P. H. et al. A comparison of three radionuclide myocardial perfusion tracers in clinical practice: the ROBUST study. Eur. J. Nucl. Med. 29, 1608–1616 (2002).
Cerquira, M. D., Weissman, N. J., Dilsizian, V., Jacobs, A. K., Kaul, S., Laskey, W. K. et al. Standarized myocardial segmentation and nomenclature for tomographic imaging of the heart: a statement for healthcare professionals from the Cardiac Imaging Committee of the Council on Clinical Cardiology of the American Heart Association. J. Nucl. Med. 9, 240–245 (2002).
Iskarndrian, A. E. Risk assessment of stable patients (panel III). In Wintergreen panel summaries. J. Nucl. Cardiol. 6, 93–97 (1999).
Frazier, L., Johnson, R. L. & Sparks, E. Genomics and cardiovascular disease. J. Nurs. Scholarship 37, 315–321 (2005).
Underwood, S. R., Anagnostopoulos, C., Cerquira, M., Ell, P. J., Flint, J., Harbinson, M. et al. Myocardial perfusion scintigraphy: the evidence of a consensus conference organised by the British Cardiac Society, the British Nuclear Cardiology Society and the British Nuclear Medicine Society, endorsed by the Royal College of Physicians of London and the Royal College of Radiologists. Eur. J. Nucl. Med. 31, 261–291 (2004).
Uemura, K., Nakura, J., Kohara, K. & Miki, T. Association of ACE I/D polymorphism with cardiovascular risk factors. Hum. Genet. 107, 239–242 (2000).
Agerholm-Larsen, B., Nordestgaard, B. G. & Tybjaerg-Hansen, A. ACE gene polymorphism in cardiovascular disease. Meta-analyses of small and large studies in whites. Arterioscler. Thromb. Vasc. Biol. 20, 484–492 (2000).
Chiang, F. T., Lai, Z. P., Chern, T. H., Tseng, C. D., Hsu, K. L., Lo, H. M. et al. Lack of association between angiotensin-converting enzyme gene polymorphism and coronary heart disease in a Chinese population. Jpn. Heart. J. 38, 227–236 (1997).
Fujimura, T., Yokota, M., Kato, S., Hirayama, H., Tsunekawa, A., Inaqaki, H. et al. Lack of association of angiotensin converting enzyme gene polymorphism or serum enzyme activity with coronary heart disease in Japanese subjects. Am. J. Hypertens. 10, 1384–1390 (1997).
Barley, J., Blackwood, A., Miller, M., Markandu, N. D., Carter, N. D., Jeffery, S. et al. Angiotensin-converting enzyme gene I/D polymorphism, blood pressure and the rennin-angiotensin system in Caucasian and Afro–Caribbean peoples. J. Hum. Hypertens. 10, 31–35 (1996).
Fatini, C., Abbate, R., Pepe, G., Battaqlini, B., Gensini, F., Ruqqiano, G. et al. Searching for a better assessment of the individual coronary risk profile. The role of angiotensin-converting enzyme, angiotensin II type 1 receptor and angiotensinogen gene polymorphisms. Eur. Heart. J. 21, 633–638 (2000).
Lahoz, C., Schaefer, E. J., Cupples, L. A., Wilson, P. W., Levy, D., Osqood, D. et al. Apolipoprotein E genotype and cardiovascular disease in the Framingham Heart Study. Atherosclerosis 154, 529–537 (2001).
Eichner, J. E., Dunn, S. T., Preveen, G., Thompson, D. M., Stuart, K. E. & Stroehla, C. B. Apolipoprtotein E polymorphism and cardiovasular disease: a huge review. Am. J. Epidemiol. 155, 487–495 (2002).
Mansur, A. P., Annicchio-Bizzacchi, J., Favarato, D., Avakian, S. D., Cesar, L. A. & Ramires, J. A. Angiotensin-converting enzyme and apolipoproteins genes polymorphism in coronary artery disease. Clin. Cardiol. 23, 335–340 (2000).
Kolovou, G., Yiannakouris, N., Hatzivassiliou, M., Malakos, J., Daskalova, D., Hatzigeorgiou, G. et al. Association of apoliprotein E polymorphism with myocardial infarction in Greek patients with coronary artery disease. Curr. Med. Res. Opin. 18, 118–124 (2002).
Kolovou, G. D., Daskalova, D. C., Hatzivassiliou, M., Yiannakouris, N., Pilatis, N. D., Elisaf, M. et al. The epsilon 2 and 4 alleles of apolipoprotein E and ischemic vascular events in the Greek population-implications for the interpretation of similar studies. Angiology 54, 51–58 (2003).
Giassakis, G., Veletza, S., Papanas, N., Heliopoulos, I. & Piperidou, H. Apolipoprotein E and first-ever ischaemic stroke in Greek hospitalized patients. J. Int. Med. Res. 35, 127–133 (2006).
Brscic, E., Bergerone, S., Gagnor, A., Colajanni, E., Matullo, G., Scaglione, L. et al. Acute myocardial infarction in young adults: prognostic role of angiotensin-converting enzyme, angiotensin II type I receptor, apolipoprotein E, endothelial constitutive nitric oxide synthase and glycoprotein IIIa genetic polymorphisms at medium-term follow-up. Am. Heart. J. 139, 979–984 (2000).
Ye, S., Dunleavey, L., Bannister, W., Day, L. B., Tapper, W., Collins, A. R. et al. Independent effects of the -219 G>T and ɛ2/ɛ3/ɛ4 polymorphisms in the apolipoprotein E gene on the coronary artery disease: the Southampton Atherosclerosis study. Eur. J. Hum. Genet. 11, 437–443 (2003).
Artiga, M. J., Bullido, M. J., Sastre, I., Recuero, M., García, M. A., Aldudo, J. et al. Allelic polymorphisms in the transcriptional regulatory region of apolipoprotein E gene. FEBS Lett. 421, 105–108 (1998).
Sambuceti, G. Differences and similarities between coronary atherosclerosis and ischaemic heart disease: implications for cardiac imaging. Eur. J. Nucl. Med. Mol. Imaging 32, 385–388 (2005).
Acknowledgements
We thank Mrs Anastasia Ziaka for her assistance in this study.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Georgoulias, P., Wozniak, G., Samara, M. et al. Impact of ACE and ApoE polymorphisms on myocardial perfusion: correlation with myocardial single photon emission computed tomographic imaging. J Hum Genet 54, 595–602 (2009). https://doi.org/10.1038/jhg.2009.83
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhg.2009.83
Keywords
This article is cited by
-
Investigating the genetic characteristics of CAD: Is there a role for myocardial perfusion imaging techniques?
Journal of Nuclear Cardiology (2022)
-
Novel approaches for the management of coronary artery disease
Herz (2021)
-
Impact of renin–angiotensin–aldosterone system polymorphisms on myocardial perfusion: Correlations with myocardial single photon emission computed tomography-derived parameters
Journal of Nuclear Cardiology (2019)
-
Does Apolipoprotein E genotype affect cardiovascular risk in subjects with acromegaly?
Endocrine (2012)
-
Apolipoprotein E Genotype and Cardiovascular Diseases in the Elderly
Current Cardiovascular Risk Reports (2010)
