
Abstract
The gene for Clara cell secretory protein (CC16) is an ideal candidate for investigating genetic predisposition to asthma because of its role in the airway as an anti-inflammatory molecule, differences in its levels between asthmatics and healthy controls, and its genetic location (11q13). We investigated the association of an SNP (A38G) and an intragenic repeat polymorphism in the CC16 gene with asthma and its associated traits, such as total serum IgE levels, in a case control as well as in a family based study design. A significant association was observed for the microsatellite repeat at the level of alleles and genotypes with asthma (P<0.05) in both the study designs. However, no association was observed for the A38G SNP with asthma. When haplotypes were constructed for these two loci and compared, the haplotype A_18 was found at higher frequency in patients (OR=1.59, 95%CI=1.08, 2.33, P=0.016). Also, in the family based design, a biased transmission was observed for haplotypes from parents to affected offspring (P=0.003). Individually, haplotype A_18 showed preferential transmission (82.6%) to affected offspring (P=0.001), thereby confirming the case-control results. In summary, this is the first study identifying the CC16 gene to be associated with asthma in the Indian population.
Similar content being viewed by others

Introduction
Asthma is a chronic airway disease affecting 15–18% of the world’s population (Smith 2000). It has been estimated that atopic asthma accounts for up to 11–12%, with a loss of man-days due to asthma and airway disorders to be 34% in Indian population (Ghosh et al. 2003; Smith 2000). Both genetic and environmental factors have been implicated in the causation of the disease (Ghosh et al. 2003). Amongst the various genes implicated, the human Clara cell secretory gene (CC16) encoding the 16 kDa protein is an important potential candidate gene for asthma because of its expression, anti-inflammatory function and genetic location (Mansur et al. 2002). The CC16 protein is primarily expressed in the respiratory tract (7% of the total protein content in the bronchoalveolar lavage fluid) by nonciliated bronchiolar secretory (Clara) cells, which play important immunomodulatory and anti-inflammatory roles in airway inflammation (Bernard et al. 1992; Broeckaert and Bernard 2000). Even micromolar concentrations of CC16 have been shown to inhibit chemotaxis of neutrophils and monocytes (Laing et al. 1998). The protein is known to control the proliferation and migration of fibroblasts in the lungs (Lesur et al. 1995). In addition, it also inhibits the activity of secreted and intracellular phospholipase A2, thereby limiting the synthesis of prostaglandins and leukotrienes (Levin et al. 1986). Interferon-γ (IFN-γ), a Th1 cytokine, has been found to increase the expression of CC16 mRNA in the mouse lung and the CC16 protein levels in cultured human airway epithelial cells (Magdaleno et al. 1998; Yao et al. 1998). Moreover, mice deficient in CC16 expression were found to exhibit a higher susceptibility to oxidant-induced lung injury and an excessive inflammatory response (Harrod et al. 1998; Johnston et al. 1997; Mango et al. 1998). All this evidence suggest that CC16 plays a protective role in the lung, and it is possible that low activity variants of CC16 may be associated with inflammatory lung disorders such as asthma. This view gains support from the observation that asthmatic individuals demonstrate significantly decreased levels of CC16 protein in their bronchoalveolar lavage fluid (BALF) (Van Vyve et al. 1995) and serum when compared to normal controls (Shijubo et al. 1999).
The gene for CC16 in humans has been localized to chromosome 11q12-13, a region shown to be highly linked to asthma and atopy (Hay et al. 1995). An adenine to guanine substitution has been detected at position 38 (A38G) downstream from the exon 1 transcription initiation site (Laing et al. 1998). The first intron also contains a polymorphic microsatellite at +2,921 to +3,110 (Mao et al. 1998). Polymorphisms within the gene, which either alter the production of CC16 or its activity, may therefore predispose an individual towards an increased risk of developing asthma. The A38G polymorphism has earlier been shown to be associated with altered plasma levels of CC16 (Laing et al. 2000); however, the mechanism for this modulation remains unclear. In a case-control study carried out in the Western Australian population, it was observed that the AA homozygotes were at 6.9-fold greater risk and AG heterozygotes were at 4.9-fold greater risk of developing asthma (Laing et al. 1998). A follow-up study showed that the asthmatics had lower plasma levels of CC16 compared to normal controls (Laing et al. 2000). This polymorphism has also been associated with an increased risk of physician-diagnosed asthma in a population of Australian children (Laing et al. 1998). A study carried out in the German population showed that PC(20) FEV(1) values were significantly lower in individuals homozygous or heterozygous for the CC16*38A allele compared with those in subjects with the CC16*38GG genotype (Sengler et al. 2003). In contrast to these results, studies on populations of Japanese and British adults (Gao et al. 1998), North American children, North European Caucasians (Laing et al. 2000), and Chinese (Gui et al. 2003) failed to replicate these associations. Also, no association has been reported between asthma and an intragenic microsatellite repeat polymorphism in CC16 in studies carried out in different populations (Mao et al. 1998).
Here, we have conducted a case control as well as a family based study to identify the genetic association of CC16 locus with asthma in the Indian population. We have investigated the A38G and the intragenic microsatellite repeat polymorphism in the study population and have attempted to evaluate the association between these markers individually and at the haplotype level to asthma status and the quantitative traits associated with asthma such as total serum IgE levels. Our results show that the CC16 gene is associated with asthma in the Indian population.
Materials and methods
Subjects
Two hundred and fifty-nine unrelated asthmatic patients (28.2±14.82 years) were recruited from various collaborating hospitals and institutions from northern India after taking written informed consent. For the family based association study, 106 trios (probands and parents) [proband mean age=14.5±9.7 years, gender ratio (male versus female)=58:42] were also recruited. The ethics committees of the participating centers and hospitals approved the study. Subjects were clinically characterized by completing a validated respiratory questionnaire designed as per the National Asthma Education and Prevention Program (Expert Panel Report-2) guidelines (Nagarkatti et al. 2004). These included patient details of the present and the past history of physician-diagnosed asthma, history of atopic symptoms, family history, the geographical region of origin, and migration status. Clinical tests performed to validate the asthma phenotype were PFT [FEV1, bronchial reversibility (>15%) test using β2-agonist inhaler (albuterol/salbutamol)], skin-prick test (SPT, wheal reaction >3 mm diameter) to a panel of 15 local environmental allergens, and total serum IgE. Only individuals with a family history of asthma/atopy were included in the study. Healthy volunteers/normal controls (N=251, 26.82±10.42 years) were selected on the basis of the criteria of having no symptoms or history of allergic diseases (Table 1). Total serum IgE levels were determined for all the control samples recruited for the study; however, SPT was performed wherever consent was obtained. Individuals who were active smokers in the past 2 years or suffering from parasitic/helminthic infestations (as determined from the clinical histories) were excluded. The genetic homogeneity between patients and controls was confirmed by genotyping loci as yet unlinked to asthma or related atopic disorders (Sharma et al. 2004). The panel of unlinked markers used were: D20S117, D6S1574, D20S196, D6S470, D12S368, D16S404, D6S446, D16S3136, D6S441, D8S264, D8S258, D8S1771, D8S285, D8S260, D8S270, D8S1784, D8S514, D8S284, D8S272, D5S406, D5S416, D5S419, D5S426, D5S418, D5S407, D5S647, D5S424, D5S641, D5S428, D5S2027, D5S471, D5S2115, D5S436, D5S422, D5S408, D6S281, D6S308, D6S264, and D6S287. These markers were tested for differences in allele frequencies in patients and controls.
Total IgE estimation
Sera were separated from blood, and total IgE levels were estimated by using the human IgE quantification kits (Bethyl Laboratories Inc., Montgomery, TX, USA), as described earlier (Nagarkatti et al. 2002).
PCR amplification and genotyping
Genomic DNA was extracted from peripheral blood leukocytes using the modified salting out procedure (Nagarkatti et al. 2004) and genotyped for polymorphisms in the CC16 gene. All subjects recruited for the study were genotyped for the A38G polymorphism by amplifying exon 1 using primers and PCR conditions, as described (Gao et al. 1998). Amplified DNA fragments were genotyped by restriction digestion with Sau96I (1 U/15 μl reaction, New England Biolabs, Beverly, MA, USA), as per the manufacturer’s instructions. PCR products from individuals with AA genotypes were refractory to digestion with Sau96I, while DNA from homozygotes for the G allele (GG genotype) was completely digested into two fragments. The accuracy of the RFLP (restriction fragment length polymorphism) genotyping was confirmed by direct sequencing of the DNA samples (N=20) for all three respective genotypes.
Genotyping for the polymorphic microsatellite repeat in the intron was performed using oligonucleotide primer pairs 5′-TTTGGCTGGTACAATCTCAATGG-3′ and 5′-TTCTGGGCACCCGTAACCTA-3′. PCR was carried out in a total volume of 15 μl containing 25 ng of genomic DNA, 1.25 pmol of each primer, 1.5 mM MgCl2, 0.25 mM of each dNTP, and 0.03 U/μl of Taq DNA polymerase (Bangalore Genie, India). The forward primer was labeled with fluorescein. PCR products were loaded with internal standard ladder (ROX-labelled) in each lane on an ABI Prism 3100 Automated Sequencer and analyzed using GeneMapper Ver3.5 (Applied Biosystems, Foster City, CA, USA).
Statistical methods
Kolmogorov-Smirnov (KS) test was used to test the association of the microsatellite allele size distribution with disease (Nagarkatti et al. 2002). This test assesses whether or not the largest difference in the cumulative frequencies in the two distributions has been caused by a chance fluctuation and tries to determine if two datasets differ significantly (Maalej et al. 2004). It has the advantage of making no assumption about the distribution of data. Thus, it is nonparametric and distribution free. Chi-square test and Fisher’s exact test (FET) were used to test the genotypic and allelic association of the polymorphisms with asthma. Likelihood ratio (LR) tests and odds ratios (OR) were calculated (http://home.clara.net/sisa/). Hardy-Weinberg equilibrium (HWE) for patients as well as controls was calculated using De Finetti program (http://ihg.gsf.de/cgi-bin/hw/hwa1.pl). ANOVA was used to assess the significance of association between polymorphisms of the CC16 gene and quantitative phenotypes such as total serum IgE levels. Haplotypes were generated in patients and unrelated controls using PHASE version 2.1 (Stephens and Donnelly 2003). The association of haplotypes was tested with asthma status and total serum IgE levels.
For the family based association study, extended transmission disequilibrium testing (E-TDT) was used to detect preferential transmission of allelic and haplotypic combinations to the affected offspring (Sham and Kurtis 1995). The association of A38G SNP with asthma was studied using TDT/STDT Program 1.1 (http://genomics.med.upenn.edu/spielman/TDT.htm) (Spielman et al. 1993). The genotype data in each trio were verified for Mendalian inheritance prior to the analysis.
Results
Total serum IgE levels in patients and healthy volunteers
The mean logarithmic total serum IgE levels were 2.93±0.83 IU/ml and 2.42±0.83 IU/ml for patients and controls, respectively, and were found to be significantly different from each other (P<0.0001). There was no significant difference between cases and controls with respect to age or male-to-female ratio (Table 1).
Association analysis with asthma and total serum IgE levels
For the A38G SNP, the distribution of CC16*A and G alleles were not found to be significantly different between cases and controls (FET P=0.30). Also, the distribution of AA, AG, or GG genotypes was concordant in cases and controls (P=0.88) (Table 2). The observed genotype counts for the markers did not deviate significantly from those expected according to the Hardy–Weinberg equilibrium (P>0.20). Also, none of the alleles/genotypes for this locus was associated with log total serum IgE levels (P>0.05).
However, for the microsatellite repeat in intron 1, a significant difference in the allele count distribution was observed between control and patient groups (KS χ2=8.58, df=2, P=0.014) (Table 2). The heterozygosity index for this repeat polymorphism is 0.6. An examination of allele counts showed that the largest difference between patients and controls was for the 18 repeat. The odds ratio for patients having 18 alleles rather than any other allele (non-18) compared to controls was 1.49 with Wald’s 95% CI=(1.14, 1.97); LR χ2=8.31; (P<0.0039). The genotype 18/18 was also found to be marginally associated with asthma [OR=1.59, 95% CI=(0.99, 2.53); P=0.051]. Further, the 16/17 genotype was found to be overrepresented in controls compared to patients (relative frequency 0.23 versus 0.14). The odds ratio for patients having the 16/17 genotype compared to controls was 0.54 with Wald’s 95% CI=(0.34, 0.85) (P=0.0075). One-way ANOVA showed a significant association between the genotypes for this locus and serum IgE levels (F ratio=2.44, df=7, P=0.019) (Table 3). Hence, the microsatellite repeat in intron 1 of the CC16 gene is strongly associated with asthma.
Further, to confirm the results obtained from our case-control study, we performed a family based study using 106 trios. The genotypic distribution followed HWE in the parents recruited for this study (P=0.20). The TDT/STDT program showed equal transmission of the CC16*A allele to that of the G allele (53 transmitted versus 53 nontransmitted) (P=1.0). On the other hand, when the transmission frequency of the microsatellite repeat in intron 1 was analyzed using E-TDT software, a biased transmission was observed for the alleles from parents to their affected offspring (allele-wise TDT χ2=9.35, df=3, P=0.02 and genotype-wise TDT χ2=10.50, df=5, P=0.06, respectively). Individually, significance was also observed for allele 18 where the transmission was observed in 66.7% of cases (TDT χ2=6.12, df=1, P=0.01). The results were statistically significant, even after Bonferroni correction (α=0.05/number of tests performed=0.01).
Association of CC16 haplotypes with asthma and total serum IgE levels
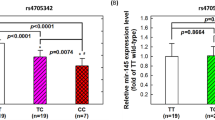
The association of the A38G polymorphism and the microsatellite repeat in intron 1 at the haplotype level was investigated using PHASE in the case-control study (Stephens and Donnelly 2003). Phase probabilities of each site were calculated for each individual by this software. Individuals with phase probabilities less than 80% were excluded from the analysis. A total of six haplotypes were obtained (Fig. 1). It was observed that the haplotype A_18 was found to be present at a higher frequency in patients compared to controls (0.15 versus 0.098; NP=76/518 and NC=49/502). The odds in favor of patients rather than controls having the haplotype A_18 was 1.59 with 95% CI=(1.08, 2.33). The corresponding likelihood χ2 showed P value less than 0.016 (LR χ2=5.76). On comparing the different haplotypic combinations with respect to the log total serum IgE levels, a marginally significant difference was obtained (F ratio=2.08, df=5, P=0.066). The log total IgE levels corresponding to the respective haplotypes are given in Table 3. Thus, the two-locus haplotype A_18 is associated with asthma and its associated trait serum IgE.

The frequency distribution of the two-locus haplotypes of the CC16 gene in patients and controls. The haplotypes were plotted on the X-axis and their respective relative frequencies (%) on the Y-axis
The haplotypes for the two loci were constructed by following the inheritance of alleles in trios. The software E-TDT was used to assess the transmission of haplotypes in the trios. A total of eight haplotypes were obtained (Fig. 1); however, two haplotypes (G_16 and A_24) had counts ≤2. These haplotypes were also not observed in the case-control study.
A biased transmission was observed for haplotypes from parents to their affected offspring (haplotype-wise TDT χ2=21.63, df=7, P=0.003). Individually, the A_18 haplotype was transmitted preferentially to the affected offspring (19 of 23 times, 82.6%transmitted) (TDT χ2=9.78, df=1, P=0.001). The difference in transmission was found to be statistically significant, even after Bonferroni correction (α=0.006).
Discussion
This is the first study showing a positive association between the microsatellite repeat polymorphism in the CC16 gene and asthma/total serum IgE levels in both case-control and family based study. Earlier studies carried out in the Caucasian and Japanese (Mao et al. 1998) population, however, failed to detect any association for this repeat with asthma. We also show here an association of haplotypes in this gene with asthma.
A few earlier studies performed in other populations showed a significant association of A38G (exonic) polymorphism with asthma (Laing et al. 1998, 2000). We have observed no association between the A38G polymorphism and asthma/log IgE in the Indian population. The study conducted in the Australian population suggested that this polymorphism is located within a region corresponding to the rat minimal promoter and therefore may influence levels of CC16 expression (Laing et al. 1998). However, three other studies carried out in different populations (Gao et al. 1998; Gui et al. 2003; Mansur et al. 2002) found no association between this CC16 polymorphism and asthma. Our study supports the latter observation. These differences in results obtained from studies carried out in different populations could be due to variation on phenotype definitions, ethnicity, and environmental exposure. One possible reason for the discrepancy in results obtained by Laing et al. (1998) from others may be that their group examined asthma in children, and it is likely that the phenotypes that constitute asthma in that study group may be different from those present in the adult population. Also, the replication of association or linkage in complex disorders has proven controversial, as the power to detect an effect is limited (Suarez and Hampe 1994). Further, as multiple genes interact to express the phenotype in complex heterogeneous traits like asthma, association will normally be observed in samples that contain an exceptionally high proportion of individuals influenced by that particular gene. However, as many studies have been unable to replicate association with this SNP, it might be possible that the cause of association observed in the first study may be due to the phenomenon of linkage disequilibrium.
To observe the combined effect of the intragenic microsatellite repeat and the A38G SNP, we constructed haplotypes using the Bayesian method for inferring haplotypes in the case-control setup (Stephens and Donnelly 2003). The inferred haplotype A_18 was found to be significantly associated with asthma (P=0.01). Our family based study also corroborated this result. Interestingly, it may be noted that the strength of association of this haplotype was weaker than the repeat allele 18 alone (P=0.01 versus P=0.004) in the case-control setup. This suggests that the combined effect of both loci taken together is weaker and the intragenic microsatellite repeat plays a bigger role compared to the SNP. Also, no linkage disequilibrium was detected between the A allele of the A38G SNP and the 18 allele of the microsatellite repeat (D′=0.11). However, in the family based analysis, a stronger association was observed for the A_18 haplotype when compared to allele 18 alone (P=0.001 versus P=0.01). This difference in the P values may be due to the fact that the A_18 haplotype in the CC16 gene is playing an important role in these families, leading to an increased susceptibility to asthma.
Though the functional role of this intronic microsatellite repeat is not yet known, it is possible that the polymorphic nature of these sequences can lead to variable effects on expression, splicing, and stability of the mRNA encoding the CC16 protein. It is known that variable repeat lengths can form secondary structures and contribute to phenotype diversity, as it was observed for the CFTR gene, where a dinucleotide repeat in intron 8 affects splicing (Hefferon et al. 2004). Also, the CA repeat polymorphism in the IFN-γ gene contributes to the variable levels of IFN-γ protein in vitro (Pravica et al. 1999).
Since asthma is a complex disorder caused by the interaction of many genes each having only a small effect, we have used a case-control study for finding any association with one of the promising loci (Sharma et al. 2004). However, a case-control study has a higher chance of finding a false-positive association than a family-based study. To circumvent this problem, the results from a well-characterized (age- and gender-matched) case-control cohort have been confirmed in a trio-based family study. We also ensured genetic homogeneity between patients and controls by genotyping markers as yet unlinked to asthma. We found no significant difference in the allele counts in patients and controls used for this study (P>0.05, data not shown).
It is important to note that the human CC16 gene maps to an important genetic region (11q12-13), which has been linked to asthma and its related phenotypes in studies carried out in various populations (Blumenthal et al. 2004; Huang et al. 2003; Simon Thomas et al. 2000; Young et al. 1992). In addition to CC16, several other important candidate genes for asthma, such as Fcɛ RIβ, CD20, and Glutathione S-transferase pi (GSTP1) are also localized in this region (Mansur et al. 2002). Earlier association studies suggested that the CC16 gene is not contributing towards the association of the 11q13 region to asthma (Gao et al. 1998; Gui et al. 2003; Mao et al. 1998). In contrast, our results suggest that CC16 is an important candidate gene in this region to be considered for genetic studies. We have recently reported a strong association between the polymorphisms of Fcɛ RIβ and asthma in two independent cohorts from the Indian population (Sharma et al. 2004). Therefore, it would be interesting to investigate the gene–gene interactions for various important genes present in this locus.
In summary, using both case-control and family based strategies, we report here the association of an intragenic repeat polymorphism in the CC16 gene with asthma.
References
Bernard A, Marchandise FX, Depelchin S, Lauwerys R, Sibille Y (1992) Clara cell protein in serum and bronchoalveolar lavage. Eur Respir J 5:1231–1238
Blumenthal MN, Ober C, Beaty TH, Bleecker ER, Langefeld CD, King RA, Lester L, Cox N, Barnes K, Togias A, Mathias R, Meyers DA, Oetting W, Rich SS (2004) Genome scan for loci linked to mite sensitivity: the collaborative study on the genetics of asthma (CSGA). Genes Immun 5:226–231
Broeckaert F, Bernard A (2000) Clara cell secretory protein (CC16): characteristics and perspectives as lung peripheral biomarker. Clin Exp Allergy 30:469–475
Gao PS, Mao XQ, Kawai M, Enomoto T, Sasaki S, Tanabe O, Yoshimura K, Shaldon SR, Dake Y, Kitano H, Coull P, Shirakawa T, Hopkin JM (1998) Negative association between asthma and variants of CC16 (CC10) on chromosome 11q13 in British and Japanese populations. Hum Genet 103:57–59
Ghosh B, Sharma S, Nagarkatti R (2003) Genetics of asthma: current research paving the way for development of personalized drugs. Indian J Med Res 117:185–197
Gui Q, Qian GS, Huang GJ, Li SP (2003) Study on association between CC16 gene G38A mutation and asthma in the patients of Han population in Chongqing (abstract). China Zhonghua Yi Xue Yi Chuan Xue Za Zhi 20:542–543
Harrod KS, Mounday AD, Stripp BR, Whitsett JA (1998) Clara cell secretory protein decreases lung inflammation after acute virus infection. Am J Physiol 275:L924–L930
Hay JG, Danel C, Chu CS, Crystal RG (1995) Human CC10 gene expression in airway epithelium and subchromosomal locus suggest linkage to airway disease. Am J Physiol 268:L565–L575
Hefferon TW, Groman JD, Yurk CE, Cutting GR (2004) A variable dinucleotide repeat in the CFTR gene contributes to phenotype diversity by forming RNA secondary structures that alter splicing. Proc Natl Acad Sci U S A 101:3504–3509
Huang SK, Mathias RA, Ehrlich E, Plunkett B, Lui X, Cutting GR, Wang XJ, Li XD, Togias A, Barnes KC, Malveaux F, Rich S, Mellen B, Lange E, Beaty TH (2003) Comparative study on the genetics of asthma evidence for asthma susceptibility genes on chromosome 11 in an African-American population. Hum Genet 113:71–75
Johnston CJ, Mango GW, Finkelstein JN, Stripp BR (1997) Altered pulmonary response to hyperoxia in Clara cell secretory protein deficient mice. Am J Respir Cell Mol Biol 17:147–155
Laing IA, Goldblatt J, Eber E, Hayden CM, Rye PJ, Gibson NA, Palmer LJ, Burton PR, Le Souef PN (1998) A polymorphism of the CC16 gene is associated with an increased risk of asthma. J Med Genet 35:463–467
Laing IA, Hermans C, Bernard A, Burton PR, Goldblatt J, Le Souef PN (2000) Association between plasma CC16 levels, the A38G polymorphism, and asthma. Am J Respir Crit Care Med 161:124–127
Lesur O, Bernard A, Arsalane K, Lauwerys R, Begin R, Cantin A, Lane D (1995) Clara cell protein (CC-16) induces a phospholipase A2-mediated inhibition of fibroblast migration in vitro. Am J Respir Crit Care Med 152:290–297
Levin SW, Butler JD, Schumacher UK, Wightman PD, Mukherjee AB (1986) Uteroglobin inhibits phospholipase A2 activity. Life Sci 38:1813–1819
Maalej A, Rebai A, Ayadi A, Jouida J, Makni H, Ayadi H (2004) Allelic structure and distribution of 103 STR loci in a Southern Tunisian population. J Genet 83:65–71
Magdaleno SM, Barrish J, Finegold MJ, DeMayo FJ (1998) Investigating stem cells in the lung. Adv Pediatr 45:363–396
Mango GW, Johnston CJ, Reynolds SD, Finkelstein JN, Plopper CG, Stripp BR (1998) Clara cell secretory protein deficiency increases oxidant stress response in conducting airways. Am J Physiol 275:L348–L356
Mansur AH, Fryer AA, Hepple M, Strange RC, Spiteri MA (2002) An association study between the Clara cell secretory protein CC16 A38G polymorphism and asthma phenotypes. Clin Exp Allergy 32:994–999
Mao XQ, Shirakawa T, Kawai M, Enomoto T, Sasaki S, Dake Y, Kitano H, Hagihara A, Hopkin JM, Morimoto K (1998) Association between asthma and an intragenic variant of CC16 on chromosome 11q13. Clin Genet 53:54–56
Nagarkatti R, Rao CB, Rishi JP, Chetiwal R, Shandilya V, Vijayan V, Kumar R, Pemde HK, Sharma SK, Sharma S, Singh AB, Gangal SV, Ghosh B (2002) Association of IFNG gene polymorphism with asthma in the Indian population. J Allergy Clin Immunol 110:410–412
Nagarkatti R, B-Rao C, Vijayan V, Sharma SK, Ghosh B (2004) Signal transducer and activator of transcription 6 haplotypes and asthma in the Indian population. Am J Respir Cell Mol Biol 31:317–321
Pravica V, Asderakis A, Perrey C, Hajeer A, Sinnott PJ, Hutchinson IV (1999) In vitro production of IFN-gamma correlates with CA repeat polymorphism in the human IFN-gamma gene. Eur J Immunogenet 26:1–3
Sengler C, Heinzmann A, Jerkic SP, Haider A, Sommerfeld C, Niggemann B, Lau S, Forster J, Schuster A, Kamin W, Bauer C, Laing I, LeSouef P, Wahn U, Deichmann K, Nickel R (2003) Clara cell protein 16 (CC16) gene polymorphism influences the degree of airway responsiveness in asthmatic children (abstract). J Allergy Clin Immunol 111:515–519
Sham PC, Curtis D (1995) An extended transmission/disequilibrium test (TDT) for multi-allele marker loci. Ann Hum Genet 59:323–336
Sharma S, Nagarkatti R, B-Rao C, Niphadkar PV, Vijayan V, Sharma SK, Ghosh B (2004) A_16_C haplotype in FcɛRIβ gene confers higher risk for atopic asthma in Indian population. Clin Genet 66:417–425
Shijubo N, Itoh Y, Yamaguchi T, Sugaya F, Hirasawa M, Yamada T, Kawai T, Abe S (1999) Serum levels of Clara cell 10-kDa protein are decreased in patients with asthma. Lung 177:45–52
Simon Thomas N, Wilkinson J, Lonjou C, Morton NE, Holgate ST (2000) Linkage analysis of markers on chromosome 11q13 with asthma and atopy in a United Kingdom population. Am J Respir Crit Care Med 162:1268–1272
Smith KR (2000) Inaugural article: national burden of disease in India from indoor air pollution. Proc Natl Acad Sci U S A 97:13286–13293
Spielman RS, McGinnis RE, Ewens WJ (1993) Transmission test for linkage disequilibrium: the insulin gene region and insulin-dependent diabetes mellitus (IDDM). Am J Hum Genet 52:506–516
Stephens M, Donnelly P (2003) A comparison of bayesian methods for haplotype reconstruction from population genotype data. Am J Hum Genet 73:1162–1169
Suarez BK, Hampe CL (1994) Linkage and association. Am J Hum Genet 54:554–559
Van Vyve T, Chanez P, Bernard A, Bousquet J, Godard P, Lauwerijs R, Sibille Y (1995) Protein content in bronchoalveolar lavage fluid of patients with asthma and control subjects. J Allergy Clin Immunol 95:60–68
Yao XL, Ikezono T, Cowan M, Logun C, Angus CW, Shelhamer JH (1998) Interferon-gamma stimulates human Clara cell secretory protein production by human airway epithelial cells. Am J Physiol 274:L864–L869
Young RP, Sharp PA, Lynch JR, Faux JA, Lathrop GM, Cookson WO, Hopkin JM (1992) Confirmation of genetic linkage between atopic IgE responses and chromosome 11q13. J Med Genet 29:236–238
Acknowledgements
We thank our collaborating physicians Dr. S. K. Sharma, Dr. Brajen Lahker, Dr. Aditi Sinha, Dr. Virender Kumar, Dr. N. K. Bhatia, and Dr. P. V. Niphadkar for helping us in sample collection. We also thank all patients, their family members, and healthy volunteers for participating in this study. We thank Ms. Mamta Sharma, Mr. Amrendra Gupta, Ms. Sanober Nahid, and Ms. Sangeeta Goswami for assistance. We acknowledge the Functional Genomics Unit of IGIB, Delhi, for helping in sequencing and genotyping. The financial support from the Council of Scientific and Industrial Research (CSIR), Govt. of India, is greatly acknowledged.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sharma, S., Ghosh, B. Association of an intragenic microsatellite marker in the CC16 gene with asthma in the Indian population. J Hum Genet 49, 677–683 (2004). https://doi.org/10.1007/s10038-004-0206-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10038-004-0206-8
Keywords
This article is cited by
-
CC16 polymorphisms in asthma, asthma subtypes, and asthma control in adults from the Agricultural Lung Health Study
Respiratory Research (2022)
-
The Indian Genome Variation database (IGVdb): a project overview
Human Genetics (2005)
-
A novel (TG) n (GA) m repeat polymorphism 254 bp downstream of the mast cell chymase (CMA1) gene is associated with atopic asthma and total serum IgE levels
Journal of Human Genetics (2005)
-
Lack of association of histamine-N-methyltransferase (HNMT) polymorphisms with asthma in the Indian population
Journal of Human Genetics (2005)
