
Abstract
Purpose: The purpose of this study was to assess the educational needs of physicians relating to genetics and genetic counseling in the Denizli region of Turkey.
Methods: Data were collected by questionnaire about physicians' approaches to genetics and genetic counseling.
Results: A total of 60 (60.0%) of 100 physicians working in Denizli province returned a questionnaire. Physicians described “their most knowledgeable subjects” in basic genetic information as chromosome abnormalities (41.8%), in genetic disorders as xeroderma pigmentosum (80.0%), and in genetic counseling as directing the parents of and couples with a risk for having a child affected by a genetic disease to an expert or a genetic counseling center (94.8%). Only 20.7% knew the ethical regulations and techniques related to genetic counseling. Physicians thought that they did not have sufficient knowledge about genetics or genetic counseling, and 83.9% would like to attend an educational course.
Conclusions: As a result of this study, a genetics course is planned for physicians so they can actively participate in the prevention and early diagnosis of genetic diseases.
Similar content being viewed by others

Main
The Human Genome Project is widely believed to be leading to a profound transformation in the practice of medicine and public health by facilitating the identification of genes causing or predisposing one to a host of human disorders, both common and rare. For better or worse, depending on one's point of view, medicine and health care are becoming “geneticized,” and it is expected that genetic considerations will become important in all aspects of disease diagnosis, treatment, and prevention.1 Over recent years there has been much debate about what role primary care physicians will play in genetics, but the field remains wide open. Initially they are likely to be involved in educational activities with their peers.2 In many European countries, general practitioners (GPs) are the primary care providers and act as gatekeepers in the referral of patients to specialist care.3 Several medical specialties serve as primary care providers in the United States, including family practitioners, general internists, general pediatricians, obstetrician-gynecologists, and primary care nurse practioners.4 Genetic diseases are increasingly being recognized in developing countries, such as Pakistan, Iran, Indonesia, Tunisia, Turkey, and India.5 Primary health care practitioners in lower-resource countries undertake a broad range of responsibilities, often in relatively isolated and difficult circumstances, with limited or distant contact with secondary or tertiary services.6 In our country the increased awareness of the importance of early diagnosis of genetic illnesses has given those illnesses priority in primary health care.7 Physicians who work in primary care in Turkey ensure that preventive and therapeutic services are provided. In particular, the physicians work together with midwives to provide maternal–child health care.8 In their mother–child monitoring, midwives refer at-risk cases to physicians.9 The majority of practicing physicians in Turkey's primary care facilities have a knowledge deficit about basic genetics and genetic counseling, which is an important reason why these services are limited.10–17
Therefore, education in genetics is an indispensable base on which to introduce programs to control genetic diseases and congenital disorders.18 The purpose of this study was to assess the educational needs of physicians related to genetic diseases and genetic counseling in the Denizli region of Turkey. The findings from this study will help inform the development of an educational strategy on genetics for primary care.
MATERIALS AND METHODS
Permission was obtained from the Province of Denizli Health Ministry to conduct this study, and they were informed about the contents of the questionnaire. Only volunteers participated in the study, and the data were collected anonymously. The items on the questionnaire were developed on the basis of an article by Erdemir,15 and a study by Mertens et al.19 In addition, basic genetic information and disorders defined by the World Health Organization (WHO) as “point-of-entry” disorders that can be prevented were also included. Questions related to genetic counseling were developed on the basis of WHO criteria in a public health study by Gökkoca10 (see Appendix).
The questionnaire's validity and reliability were not researched because our goal was not to create a tool.
Procedures
All 26 of the health clinics in Denizli province were included in the study, and questionnaires were used. Physicians who worked at these health clinics were included in the study. The self-report method was used for data collection.
Measures
The following categories of information were asked on the questionnaires: sociodemographic information, basic genetic information, theoretical/practical information about some genetic diseases/disorders, genetic counseling experience, and sources for information.
Data analysis
In this cross-sectional and descriptive study, data were analyzed using the Statistical Package Program for the Social Sciences (version 13.0; SPSS Inc., Chicago, IL). Descriptive statistics, including mean ± standard deviation, frequencies, and percentages, were calculated in the current study. To determine the relationship between two categorical variables, the chi-square test was used. The statistical significance was set at the 5% level (P ≤ 0.05).
RESULTS
Response rate and demographic characteristics
A total of 60 of the 100 physicians who work full time in the 26 health clinics in the province answered the questionnaire (response rate of 60.0%) and were included in the study. The majority of our respondents were male (56.7%). The age of the 60 physicians who answered the questionnaire ranged from 28 to 58 years, with a mean of 37.4 ± 6.11 years. The length of time in their profession ranged from 3 to 26 years with a mean of 12.64 ± 5.62 years (Table 1).
Genetic knowledge
The examination of basic genetic information showed that the highest percentage (41.8%, n = 23) knew about chromosome abnormalities and that the lowest percentage (3.8%, n = 2) knew about polygenic inheritance (Table 2).
The examination of the sources of information about some genetic abnormalities and illnesses showed that the highest percentage (80.0%, n = 44) knew about xeroderma pigmentosum and that the lowest percentage (12.7%, n = 7) knew about diabetes mellitus (Table 3).
Knowledge associated with genetic counseling
For answers related to genetic counseling the highest percentage was 94.8% (n = 55) for directing at risk couples or parents to an expert or a genetic counseling center. The lowest was 20.7% (n = 12) for those who knew the ethical regulations and techniques related to genetic counseling. In addition, 21.1% were able to develop a family tree by learning the genetic history of individuals in whom a genetic disorder was suspected, 22.8% were able to organize a screening program for genetic diseases, 27.3% knew about the genetic counseling center in Denizli, and 55.4% stated that they knew about genetic diseases common in the region. The majority of the physicians (83.9%) stated that they would like to participate in an educational program (Table 4).
Sources of knowledge
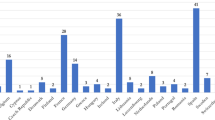
The distribution of answers to the multiple-choice question about physicians' sources of information was, in order: class in medical school (n = 51), book (n = 49), press (n = 12), word-of-mouth (n = 2), course (n = 20), seminar (n = 22), conference (n = 23), and the Internet (n = 9).
DISCUSSION
Deficiency of genetic knowledge
Basic genetic counseling is both feasible and increasingly necessary in primary health care (WHO 1999).20 Minimally, physicians will need sufficient knowledge about genetics to answer questions, identify at-risk patients, and refer appropriately.21 In this study, most of the participants reported having insufficient knowledge about ethics of human genetics, genetic screening, counseling, engineering, and polygenic inheritance. Practicing physicians do not think they have enough information about genetic diseases or genetic counseling and recognize their need for more education. McGovern et al.22 found that 79% of genetic counselors participated in the general education of physicians about genetic testing. The need for this education and its benefits in primary care have been defined by Kolb et al.23 and Kirk.24 In another study by Tomatır et al.,9 the need for this education in primary care was emphasized.
With the rapid development of many potential gene therapies just on the horizon, all physicians will have major continuing medical education needs in the area of genetic diseases.25 Primary care physicians need more education about the genetic component of many diseases to directly provide and appropriately refer for genetics services.26
Primary care providers and GPs are under increasing pressure from professionals involved in the delivery of genetics services to become more knowledgeable about genetics and more aware of the need to counsel and refer patients for genetic testing when appropriate. There have been several studies of GPs' knowledge of genetics and genetic services and of their receptiveness to an increased emphasis on genetics and genetic counseling in primary care. The majority of these studies have been undertaken in the United States and United Kingdom.27 Watson et al.28 believe there is a need to develop and evaluate a model for the delivery of genetic services that incorporates a realistic role for primary care and takes the views of primary health care professionals into account. Hunter et al.29 found that a majority of physicians considered their knowledge of genetics to be adequate, but that a minority were confident to provide genetic counseling in simple genetic scenarios. Relatively few had actually made use of DNA diagnostic services, and there was relatively poor knowledge of what services were available. Menasha et al.30 found that further education for physicians is required for them to accurately convey the risks and benefits of genetic testing to their patients. No similar studies conducted in Turkey were found in a review of the literature.
Limitations of the study
Our response rate of 60% was below our expectations. Nevertheless, the number and distribution of our responses were sufficient for analysis. In Turkey, practicing physicians do not have the role of “gatekeeper” because of differences in the health care systems. Because there is inadequate knowledge about screening and counseling even in areas with abundant genetic services in Turkey, intervention at the primary care level is limited.
CONCLUSIONS
In this study, physicians who are actively giving genetic counseling recognize their knowledge deficits, and a large percentage request participation in an educational program. The prevention of genetic diseases before birth and the early diagnosis after birth could be a result of educational programs on this subject. This education could be provided by the Health Ministry in cooperation with university instructors and clinical geneticists. International cooperation on this subject could also be arranged. The WHO works with various nongovernmental organizations and collaborating centers that support implementation of genetics approaches to disease control in countries. In addition to the recognition of genetic services in the region and the country, consideration of medical genetics services and the application of their supporting genomic technologies should be an integral part of education in genetics at all levels. Genetic education needs to be provided not only to the primary care providers but also to the medical students who will soon join their ranks. Finally, the most efficient and effective methods for providing information and heightening awareness need to be determined through additional research.
References
Epstein CJ . Genetics in primary care: what do we expect? (book review). Nat Genet 2001; 29: 13–14.
Kavalier F, Kent A . Genetics and the general practitioner. BMJ 2003; 327: 2–3.
Baars MJH, Henneman L, Ten Kate LP . Deficiency of knowledge of genetics and genetic tests among general practitioners, gynecologists, and pediatricians: a global problem. Genet Med 2005; 7: 605–610.
Burke W . Genetic testing in primary care. Annu Rev Genomics Hum Genet 2004; 5: 1–14.
Alwan A, Modell B . Recommendations for introducing genetics services in developing countries. Nat Rev Genet 2003; 4: 61–68.
Christianson A, Modell B . Medical genetics in developing countries. Annu Rev Genomics Hum Genet 2004; 5: 219–265.
Tunçbilek E . Genetik hastalıkların görülme sıklığında birinci basamak sağlık hizmetlerinin etkisi var mıdır? (Is there an effect of primary health care services on the incidence of genetic diseases?). Sürekli Tıp Eğitimi Dergisi 1998; 7: 21–24.
Turkish Ministry of Health, Basic Health Services, General Directorate. Directive Number 8597 Concerning the Implementation of Health Care Services dated 2001; 12–20.
Tomatır AG, Özşahin A, Sorkun HÇ, Demirhan H, et al. 2006. Midwives' approach to genetic diseases and genetic counseling in Denizli, Turkey. J Genet Couns 2006; 15: 191–198.
Gökkoca FZU . Genetik hastalıklar: Korunma, örgütlenme ve temel sağlık hizmetleri (Genetic diseases: protection, organization and basic health services). Hacettepe Toplum Hekimliği Bülteni 2000; 2: 10–12.
Hızel S . Kalıtsal metabolik hastalıklarda danışmanlık ve hasta izleminde birinci basamak sağlık personelinin katkısı (Counseling in inherited metabolic diseases and the contribution of primary health care personnel in patient follow-up). Sürekli Tıp Eğitimi Dergisi 1995; 7: 403–404.
Genç Z, Erdemir AD . Genetik sorunlar ve tıbbi etik (Genetik Danışma) (Genetic problems and medical ethics [Genetic Counseling]), 1st ed. İstanbul: Nobel Tıp Kitabevleri Ltd şti, 1997.
Genç Z, Erdemir AD . Genetik danışmanlığın tıbbi etik açısından önemi ve bazı sonuçları (The importance of genetic counseling from the point of view of medical ethics and some results). T Klin Tıbbi Etik 1997; 5: 73–77.
Genç Z . Tıbbi biyolojide genetik danışmanlığa genel bir bakış (A general overview of genetic counseling in medical biology). Sendrom 1998; 10: 15–21.
Erdemir AD . Genetik danışmana gerek duyulan genetik hastalıklar ve tıbbi etikteki yeri (Genetic diseases in need of genetic counseling and their importance in medical ethics). T Klin Tıbbi Etik 1998; 6: 73–82.
Gökkoca FZU, Etiler NB . Çocukluk döneminde genetik hastalıkların epidemiyolojisi ve kontrolü (Epidemiology and control of genetic disorders in childhood). Sağlık ve Toplum 1999; 3: 19–26.
Tomatır AG . Genetik hastalıklardan korunma (Protecting against genetic diseases). Sendrom 2003; 15: 44–52.
World Health Organization 2005. Control of genetic diseases. (Executive Board EB116/3). Geneva: World Health Organization.
Mertens TR, Hendrix JR, Morris MM . Nursing educators: perceptions of the curricular role of human genetics/bioethics. J Nurs Educ 1984; 23: 98–104.
World Health Organization (1999). Services for the prevention and management of genetic disorders and birth defects in developing countries. Report of the joint WHO/WAOPBDmeeting (WHO/HGN/GL/WAOPBD/99.1). Geneva: World Health Organization.
Caulfield T . Gene testing in the biotech century: are physicians ready?. CMAJ 1999; 161: 1122–1123.
McGovern MM, Benach M, Zinberg R . Interaction of genetic counselors with molecular genetic testing laboratories: implications for non-geneticist health care providers. Am J Med Genet 2003; 119A: 297–301.
Kolb SE, Aguilar MC, Dinenberg M, Kaye CI . Genetics education for primary care providers in community health settings. J Health Commun 1999; 24: 45–59.
Kirk M . Genetics, ethics and education: considering the issues for nurses and midwives. Nurs Ethics 2000; 7: 215–226.
Williamson PS . Genetic testing. Am Fam Physician 2000; 61: 2968, 2970–2972.
Hayflick SJ, Eiff PE, Carpenter L, Steinberg J . Primary care physicians utilization and perceptions of genetics services. Genet Med 1998; 1: 13–21.
Robins R, Metcalfe S . Integrating genetics as practices of primary care. Soc Sci Med 2004; 59: 223–233.
Watson EK, Shickle D, Qureshi N, Emery J, et al. The ‘new genetics' and primary care. GPs' views on their role and their educational needs. Fam Pract 1999; 16: 420–425.
Hunter A, Wright P, Cappelli M, Kasaboski A, et al. Physician knowledge and attitudes towards molecular genetic (DNA) testing of their patients. Clin Genet 1998; 53: 447–455.
Menasha JD, Schechter C, Willner J . Genetic testing: a physician's perspective. Mt Sınai J Med 2000; 67: 144–151.
Acknowledgements
We thank all the physicians who participated in the survey. We also thank the Turkish Ministry of Health for giving us permission to use the questionnaire and make this work possible.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors declare no conflict of interest.
A supplementary Appendix is available via the ArticlePlus feature at www.geneticsinmedicine.org. Please go to the February issue and click on the ArticlePlus link posted with the article in the Table of Contents to view this material.
Rights and permissions
About this article
Cite this article
Tomatir, A., Sorkun, H., Demirhan, H. et al. Genetics and genetic counseling: Practices and opinions of primary care physicians in Turkey. Genet Med 9, 130–135 (2007). https://doi.org/10.1097/GIM.0b013e3180306880
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1097/GIM.0b013e3180306880
