
Abstract
Purpose
To report a series of patients with ocular complications associated with laser-assisted eyebrow hair removal.
Patients and methods
Case reports of three patients with eye pain and photophobia following laser epilation of the eyebrow region. The eye examination included visual acuity, slit-lamp examination, tonometry and fundoscopy. The follow-up period was 3 months.
Results
Each patient had conjunctival hyperaemia in one or both eyes and anterior chamber pigmentary cells. One patient presented with posterior synechiae, which did not respond to treatment.
Conclusions
Laser epilation of the eyebrows may result in anterior uveitis as well as irreversible damage to the iris.
Similar content being viewed by others


Introduction
Laser-assisted epilation is currently the most efficient long-term method for body and facial hair removal. Various laser systems are available for this use, such as ruby laser (694 nm), alexandrite (755 nm), diode (800 nm), and neodymium-YAG (1064 nm).1 Periocular (eyebrow) laser hair removal is rarely associated with complications. We present three cases of ocular complications caused by diode laser-assisted removal of eyebrow hair.
Case reports
Case 1
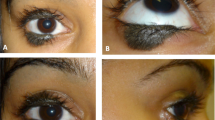
A 27-year-old healthy lady with mild myopia had undergone laser epilation of both eyebrows. She had shut her eyes during the treatment. 2 days later, she complained of severe pain and photophobia in both eyes. Eye examination revealed multiple pigmentary cells in both anterior chambers and posterior synechiae in both eyes (Figure 1). She received topical steroid and topical cyclopentolate, with no improvement. A subconjunctival injection of atropine (0.01 mg) and adrenaline (0.01 mg) to the left eye had no effect. The eye condition had not altered at the 1-week and 3-month follow-up examination: her anterior chambers were clear but the dilated pupil and posterior synechiae in the left eye persisted, (Figure 2) as did the severe photophobia.

Posterior synechiae in the left eye of Case 1.

The posterior synechiae in the left eye of Case 1 is still present at the 3-month follow-up examination.
Case 2
A 35-year-old healthy lady with no previous eye problems, presented with the complaints of pain and redness in her right eye 1 week after undergoing eyebrow laser epilation. Protective shields had been used during most of the treatment, but she was instructed to cover her eyes with two fingers because of difficulties in treating the lower eyebrow region. On examination, her uncorrected visual acuity was 6/6 in both eyes. The right eye had moderate conjunctival injection, multiple pigmentary cells in the anterior chamber, and pigment on the anterior capsule of the lens. Both the pupils were round and reactive, and the left eye was quiet. Treatment with topical steroids and cycloplegic drops led to resolution of the signs and symptoms within 2 weeks. The 3-month follow-up examination was normal apart from pigment on the anterior lens capsule of the right eye.
Case 3
A 24-year-old healthy lady with no previous eye problems, presented with complaints of pain, photophobia, and redness in her left eye 1 day after undergoing eyebrow laser epilation. She complained that she experienced severe photophobia and glare as soon as the laser treatment was over. Her uncorrected visual acuity was 6/6 in both eyes. There was moderate conjunctival injection and multiple pigmentary cells in the anterior chamber of the left eye. The left pupil was dilated to 4 mm and partly reactive to light. Treatment consisted of topical steroids. The uveitis cleared within 1 week but the pupil remained dilated; it became round and reactive at the 6-week follow-up and remained so at the 3-month follow-up.
Comment
Laser epilation, based on selective thermolysis, is an increasingly popular method of long-term hair removal. The chromophore melanin of the hair follicle at the dermis level absorbs the delivered energy, rather than the more superficial epidermal melanin, which would result in depigmentation of the skin. The instruments used for dermatologic purposes are therefore planned to penetrate to a depth of 3–4 mm. The probe is supposed to be firmly placed on the treated skin to reach this depth, but this might be difficult to achieve on the inferior border of the eyebrow due to the structure of the orbital bones. The tendency to close the eyes during the procedure results in the eyes moving upwards under the closed eyelids (Bell′s phenomenon), causing the pigmented iris to reach the laser penetration range and leading to a variety of clinical presentations, such as iritic atrophy, anterior uveitis and posterior synechiae.2, 3
Our MEDLINE search yielded several published case reports on this subject. Halkiadanis et al2 described a 30-year-old lady who presented with iritic atrophy and posterior synechiae after eyebrow laser epilation. Her condition was unchanged 6 months after the procedure. Herbold et al3 reported a more severe case associated with iritic atrophy and cataract that eventually reduced visual acuity. The patients in the above cited cases had removed their protective goggles to facilitate hair removal from the lower part of the eyebrow. Shikh et al4 described a patient suffering from uveitis and visual field defect after photoepilation of the upper eyelid despite using protective shields.
We wish to raise the ophthalmologists' level of awareness of this form of cosmetic treatment as an iatrogenic cause of ocular damage. Individuals contemplating laser-assisted eyebrow hair removal must be advised of the potential risks to their eyes.
References
Liew SH . Laser hair removal: guidelines for management. Am J Clin Dermatol 2002; 3: 107–115.
Halkiadakis I, Skouriotis S, Stefanaki C, Patsea E, Papakonstatndinou D, Amariotakis A et al. Iris atrophy and posterior synechiae as a complication of eyebrow laser epilation. J Am Acad Dermatol 2007; 57 (2 Suppl): S4–S5.
Herbold TM, Busse H, Uhlig CE . Bilateral cataract and corectopia after laser eyebrow [corrected] epilation. Ophthalmology 2005; 112: 1634–1635. Erratum in: Ophthalmology 2006; 113(6): 984.
Sheikh A, Hodge W, Coupland S . Diode laser-induced uveitis and visual field defect. Ophthal Plast Reconstr Surg 2007; 23: 321–322.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shulman, S., Bichler, I. Ocular complications of laser-assisted eyebrow epilation. Eye 23, 982–983 (2009). https://doi.org/10.1038/eye.2008.436
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2008.436
Keywords
This article is cited by
-
Anterior uveitis associated with laser epilation of eyebrows
Journal of Ophthalmic Inflammation and Infection (2013)
