
Abstract
Aim
To compare morphometric data of the eyelid fissure and the levator muscle function (LF) before and up to 6 months after transcutaneous injection with five units of Botox® in patients with upper lid retraction (ULR) from congestive or fibrotic thyroid eye disease (TED).
Methods
Twenty-four patients with ULR from TED were submitted to transcutaneous injection of 5 units (0.1 ml) of Botox in one eye only. Patients were divided into two groups: 12 with congestive-stage TED (CG), and 12 with fibrotic-stage TED (FG). Bilateral lid fissure measurements using digital imaging and computer-aided analysis were taken at baseline and at regular intervals 2 weeks, 1 month, 3 months and 6 months after unilateral Botox injection. Mean values taken at different follow-up points were compared for the two groups.
Results
Most patients experienced marked improvement in ULR, with a mean reduction of 3.81 mm in FG and 3.05 mm in CG. The upper eyelid margin reflex distance, fissure height and total area of exposed interpalpebral fissure were significantly smaller during 1 month in CG and during 3 months in FG. Reduction in LF and in the difference between lateral and medial lid fissure measurements was observed in both groups. The treatment lasted significantly longer in FG than in CG.
Conclusions
A single 5-unit Botox injection improved ULR, reduced LF and produced an adequate lid contour in patients with congestive or fibrotic TED. The effect lasts longer in patients with fibrotic orbitopathy than in patients with congestive orbitopathy.
Similar content being viewed by others


Introduction
Observed in approximately 90% of patients, upper lid retraction (ULR) is the most common clinical sign of both the congestive and the fibrotic stage of thyroid eye disease (TED).1 Although usually mild and self-limited, ULR may lead to a cosmetically unacceptable appearance and exposure keratopathy causing ocular discomfort, tearing, photophobia, conjunctival hyperaemia and occasionally corneal ulceration. Management of ULR depends on the stage of the disease. In the congestive/autoimmune phase of TED treatment of ULR it is generally based on lubricating eye drops for relief of exposure keratopathy. A recent study showed favourable response of triamcinolone injection in four patients with ULR in the congestive stage of TED2 but further studies are necessary to confirm such findings. The use of topical guanetidine eye drops may be considered but the results are generally disappointing due to undercorrection, conjunctival hyperaemia and/or miosis.3, 4 In the fibrotic stage of TED, treatment of ULR is generally surgical and employs techniques for recession of the levator muscle, excision of Müller's muscle, myotomies or the introduction of spacers. However, in spite of the great number of available procedures, the outcome is still largely unpredictable. Patients frequently display under- or overcorrection and inadequate lid contour, so multiple procedures may be required to achieve the desired result.5
Botulinum toxin Type A (BTA) was introduced in the early 1980s by Scott6, 7 as an alternative treatment for ULR and reinforced on small case series by Ebner,8 Biglan,9 Ozkan et al,10 and Traisk and Tallstedt11 with encouraging results. Larger patient series have also supported BTA as a temporary relief treatment of ULR. Uddin et al,3 injected BTA transconjunctivally in 11 patients with stable orbitopathy and obtained an acceptable lid position in 10 subjects. The authors documented a systematic follow-up evaluation at 1 month after the first injection, but longer follow-up results were not reported. Shih et al,12 followed 15 patients with stable orbitopathy for 4–6 months after a transcutaneous injection of Botox® and found a mean difference of −3.1 mm between pre- and post-injection ULR values by the first week. The effect remained for at least 2 months, but all patients recovered to pretreatment levels of ULR before completing the fifth month of follow-up. Dintelman et al,13 evaluated 13 patients with ULR after injection of 5–15 units of Botox and reported that eight patients were satisfied with the results. On the other hand, Morgenstern et al,14 were the first to evaluate a series of patients with TED in the congestive stage. A mean reduction of 2.35 mm was observed 1 week after injection of BTA in 18 patients. However, no follow-up information regarding the duration of the treatment was provided.
Despite the results mentioned above, several issues regarding the use of BTA for correction of dysthyroid ULR are still open to questioning. For example, it is not clear whether the duration of the effect of BTA is the same in the fibrotic and the congestive stage of the disease. Also, although patients may be given multiple injections, it is important to know what to expect of the first treatment – an issue that has not been properly dealt with in previous studies. Finally, although some studies have reported ptosis in the treated eye and lid retraction in the contralateral eye, no systematic investigation of lid contour abnormalities has been carried out with patients treated with BTA for correction of ULR. The purpose of the present study was therefore to prospectively evaluate the effect of transcutaneous injection of BTA upon lid position and other eyelid fissure contour parameters in patients with dysthyroid ULR followed for 6 months. We also directly compared findings for patients with congestive orbitopathy and patients with fibrotic orbitopathy. Finally, the effect of unilateral use of BTA upon the levator muscle function (LF) of the treated eye and upon contralateral lid position and contour was systematically investigated in both groups of patients.
Patients and methods
This was an interventional prospective study conducted between October 2005 and September 2007. The study followed the principles of the Declaration of Helsinki, approval from the Institutional Review Board Ethics Committee was obtained and all participants gave their informed consent.
The study included 24 eyes of 24 patients (21 women) with a diagnosis of TED established according to previously published criteria.15 To be included in the study subjects were required to be older than 18 years and to have unilateral or bilateral asymmetric ULR secondary to TED either in the congestive/inflammatory or in the fibrotic stage of the disease.
The definition of congestive/inflammatory TED included the presence of conjunctival and eyelid oedema and erythema as well as unstable motility, eyelid position or exophthalmometry measurements. Fibrotic TED patients, on the other hand, were required to have had eye signs for at least 2 years and to have been clinically and hormonally stable for at least 6 months, and absence of inflammatory eye signs.
We excluded patients suffering from optic neuropathy or severe corneal ulcers requiring urgent orbital decompression, as well as patients with restrictive strabismus; pregnancy or any abnormal ocular condition precluding participation in the study. All patients underwent a complete ophthalmic examination.
The eyelid position of both eyes was video-recorded at baseline and at 2 weeks, 1 month, 3 months and 6 months following treatment using a portable digital video-camera connected to a microcomputer. The camera was positioned at a distance of 1 m and the subjects were requested to fixate straight ahead with the head immobilized on a head and chin rest. A millimeter ruler positioned in front of the forehead was used as a reference for the eyelid fissure measurements. The software Pinnacle Studio (version 9.0; Avid technology Inc., Mountain View, CA, USA) was used for video editing. Eyelid fissure measurements were analyzed with the public domain software Image J 1.4 (available at http://rsb.info.nih.gov/ij/). A 1-min video was recorded for each patient and the three images showing the largest eyelid fissure measurements were selected for the study. To reduce the effect of possible variability, the measurements of the three selected images were averaged for further analysis.
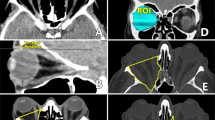
Three eyelid parameters were measured (in millimeters) in both the treated eye and the contralateral eye: a – the palpebral fissure height (FH) (the widest vertical point between the upper and the lower lid margin); b – upper eyelid margin reflex distance (MRD1) (the distance between the upper eyelid margin and the pupil centre); and c – lower eyelid margin reflex distance (MRD2) (the distance between the lower eyelid margin and the pupil centre). At each examination we also calculated the total eyelid fissure area (FA) in the eye submitted to BTA treatment.
The evaluation of the upper eyelid position in patients with TED indicated the existence of enhanced retraction of the lateral aspect of the eyelid, which has been referred to as ‘eyelid flare’.16 To investigate the effect of BTA on the eyelid flare, we performed two eyelid FA measurements: the upper nasal area (UNA) and upper temporal area (UTA) between the upper eyelid margin and a straight line connecting the inner and outer canthi, following a previously described method.17 To divide the upper area of the fissure in two halves (nasal and temporal), a line was drawn from the midportion of the line connecting both canthi up to the upper eyelid margin. We then calculated and compared those areas as well as the difference between them before treatment and at each follow-up examination.
LF was measured in millimeters as the excursion of the upper eyelid from downgaze to upgaze, with the frontalis muscle fixed in position by digital pressure.
Botulinum toxin A (Botox, Allergan Inc., Irvine, CA, USA) injection was administered on an outpatient basis. Each vial (100 U) was diluted in 2 ml of non-preserved saline solution. The concentration obtained was 5 U/0.1 ml. After skin antisepsis, the drug was injected transcutaneously with a tuberculin syringe and a 30-gauge needle into the suborbicularis space in the middle third of the upper eyelid 3 mm above the centre of the superior tarsal border.
Only one eye of each patient was treated. In patients with bilateral retraction, injection was administered in the eye with the larger eyelid fissure. If no effect on the lid was observed 1 week after treatment, a second 2.5-unit injection was applied at the same location.
Descriptive statistics included mean values±SD for normally distributed variables. We used χ2 test, Fisher's exact test and Mann–Whitney's test to assess the homogeneity between the two study groups (CG and FG). Friedman's non-parametric test was used to compare the eyelid fissure measurements and LF at each examination. P-values under than 0.05 was considered statistically significant.
Results
Twenty-four patients with TED were divided into two groups: 12 with congestive-stage group TED (CG), and 12 with fibrotic-stage TED (FG). The mean age±SD age was 43.6±15.2 years in CG and 38.0±13.1 years in FG. Ten patients in CG and 11 in FG were female. Nine patients in CG and six in FG had unilateral lid retraction. No statistically significant differences were found between CG and FG regarding the above-mentioned variables. Only two patients in CG required a second toxin application to produce the desired effect.
Most of the patients experienced considerable improvement in ULR (Figure 1). Eyelid fissure measurements of the treated eye before and after Botox injection are shown for each group of patients in Table 1 and Figure 2. Compared to baseline measurements, FH had decreased by 3.05 mm in CG and by 3.81 mm in FG 2 weeks after injection. At 1 month, the corresponding reduction was 2.85 and 3.54 mm, respectively. In CG a statistically significant reduction was found for FH and MRD1 values between baseline and 2 weeks or months after treatment. No significant difference was observed between baseline and findings 3 or 6 months after treatment. In FG a significant difference was found for FH and MRD1 values between baseline and 2 weeks, 1 month or 3 months after treatment. No significant difference was observed between baseline measurements and findings after 6 months of treatment. Likewise, no significant difference was observed in the pre and post-treatment MRD2 values for either group.

Example of improvement in upper eyelid retraction in a patient with unilateral right eyelid retraction in the fibrotic stage of thyroid eye disease. Above: before treatment; below: 1 month after transcutaneous injection of five units of botulinum toxin A in the right eye.

Graph representing mean upper eyelid margin reflex distance (MRD1) values before and after botulinum toxin A treatment in 24 eyes of 24 patients with thyroid eye disease. Left: treated (injected) eye; right: contralateral (non-injected) eyes; dashed line: group of patients in the congestive disease; continuous line: group of patients with fibrotic disease.
Table 2 and Figure 2 show eyelid measurements of untreated, contralateral eyes before and after BTA injection. On the average, FH had increased by 0.57 mm in CG and by 0.93 mm in FG 2 weeks after injection. In the same period MRD1 values increased 0.43 and 0.55 mm in CG and FG, respectively. FH and MRD1 varied significantly in both groups between baseline and 2 weeks after treatment. No statistically significant difference was found between measurements taken at baseline and at 1, 3 or 6 months. MRD2 values did not vary significantly in either group or at any moment.
Mean FA values±SD (in square millimeters) of treated eyes in CG before treatment and 2 weeks, 1 month, 3 months and 6 months post-injection were 230.30±20.79, 184.02±24.95, 196.71±30.59, 205.72±28.84 and 216.93±32.73, respectively. The corresponding figures for FG were 255.66±47.43, 185.06±37.28, 204.30±38.99, 227.75±43.40 and 235.14±52.82, respectively. In CG FA was significantly reduced between baseline and 2 weeks or 1 month after treatment. No significant difference was observed between measurements taken at baseline and findings 3 or 6 months after BTA injection. In FG, baseline FA values differed significantly from FA values at 2 weeks, 1 month and 3 months after treatment. No significant difference was observed between baseline measurements and findings 6 months after BTA injection.
Mean difference of UTA–UNA measurements±SD (in square millimeters) of treated eyes in CG before treatment and 2 weeks, 1 month, 3 months and 6 months post-injection were 27.87±8.65, 16.10±5.33, 18.27±6.88, 16.77±8.88 and 20.35±8.78, respectively. The corresponding figures for FG were 30.09±7.25, 14.76±7.46, 16.07±7.65, 17.30±7.65 and 18.94±7.97, respectively. The difference between UTA and UNA measurements in both groups revealed a significant difference between baseline values and findings 2 weeks, 1 month and 3 month after treatment in both groups, indicating a beneficial effect on lid contour in both groups during at least 3 months.
LF measurements in both the treated and the contralateral eye, along with their variation during follow-up, can be seen in Table 3. In the treated eye of patients in the CG, measurements differed significantly only between baseline and 2 weeks after treatment, not thereafter. However, in FG a significant difference was observed in the LF of the treated eye between baseline and 2 weeks or 1 month post-treatment. No significant difference was observed between baseline and any other measurements in the untreated eye of either study group.
Temporary (lasting less than 30 days) side effects resulting from BTA injection include partial ptosis in five eyes (20.8%) and lagophthalmos and ecchymosis at the injection site in one patient each (4.2%). No difference was observed between the study groups with regard to the observed side effects.
Discussion
The current investigation confirms several previous studies reporting favourable results with BTA in the treatment of ULR3, 6, 8, 10, 13, 14 and suggests that BTA may come to play an important role in the management of ULR secondary to TED. Considering the lack of treatment options for congestive-stage ULR, the long preoperative waiting time and the often unpredictable results of surgical treatment (including the frequent occurrence of abnormalities in lid contour) in the fibrotic-stage, the addition of a relatively simple treatment option such as BTA injection is a welcome initiative. However, although BTA has long been employed in the management of ULR and is universally available, it has not gained wide acceptance as an adjuvant in the management of patients with TED. Uncertainty regarding action, mode of administration and duration of treatment along with concern about the possibility of under- or overcorrection partly account for the limited use of BTA and point to the need of further well-controlled studies on the subject.
In the current study, we address some of the above-mentioned issues in a systematic way to explore the effect and duration of BTA therapy. For example, unlike authors3, 8, 13, 14 using a variable dose of BTA depending on the severity of ULR and repeating injections according to post-treatment findings, we decided to use only five units of BTA in patients with unilateral or asymmetric ULR and investigate its effects on the injected eye and the contralateral eye over a 6-month follow-up period, avoiding re-injections during the study period. We also found it relevant to compare findings for patients with congestive and fibrotic TED, an approach which, to our knowledge, has not been tested before. Furthermore, instead of using direct measurements of lid fissure parameters, we used mean values of three digital images obtained by computer-aided analysis. Finally, we believe to be the first to include a sequential evaluation of the LF in the injected eye before BTA injection and at 2 weeks, 1 month, 3 months and 6 months post-treatment.
Owing to variations in dose and number of injections, few previous studies can be compared directly with our results with regard to degree of lid retraction correction. Shih et al,12 also administered a single transcutaneous injection of Botox (usually five, but occasionally six units) to correct lid retraction in patients with TED in the fibrotic stage. The authors observed a 3.1-mm reduction in ULR by the first week, the effect of which remained for at least 2 months, although no actual figures were provided regarding this period. Biglan9 reported one patient in whom the injection of five units of BTA lead control of eyelid retraction for 4 months, although the author did not report the amount of correction in millimeters. Traisk and Tallstedt11 injected three patients with five units of BTA and found an average reduction of ULR of 4.5 mm (range, 3.0–5.0 mm), but did not report the exact duration of treatment. Our study demonstrates that a transcutaneous injection of five units of BTA can produce an average reduction in ULR of 3.81 mm in patients with fibrotic TED and 3.05 mm in patients with congestive TED 2 weeks after treatment. The effect decreased to 3.54 and 2.85 mm, respectively, at 1 month, and progressively thereafter. The effect lasts at least for 3 months in patients with fibrotic orbitopathy but has a shorter duration of patients with congestive orbitopathy (Table 1, Figure 2). However, it should be pointed out that most of our patients had moderate ULR. Thus, while the dose tested appeared to be appropriate for our patients, subjects with milder or more severe ULR may require different regimens. Comparable studies testing different doses will help clarify the issue in the future.
We do not have an exact explanation for the difference in results obtained for patients with congestive and fibrotic orbitopathy. At least two explanations are possible: First, it is conceivable that the drug was absorbed due to increased vascular circulation in the congestive stage of the disease leading to a reduced local effect. Second, ULR may have worsened during the follow-up period, counteracting the effect of Botox in the lid, although a comparison of ULR values at baseline and at the end of the follow-up period does not support this hypothesis.
In the current study, we also systematically investigated the effect of unilateral BTA treatment on the contralateral eyelid. Our study confirmed previous reports of the occurrence or worsening of lid retraction after use of BTA in the opposite eye attributed to the effect of Hering's law on the eyelid retractor muscles.18 In our study, some patients did in fact present lid retraction, or worsening of lid retraction, in the contralateral eye, but the effect did not extend beyond 2 weeks after treatment (Table 2). Thus, the effect in the contralateral eye lasted much less than the effect of Botox in the injected eye, suggesting that adaptative mechanisms in the neuronal inputs to the non-injected eyelid may occur.
Four other parameters were included in our study that had not been reported in earlier investigations of this type: lower eyelid position, fissure area, effect on lid flare and effect on levator muscle function. We found no effect of BTA in the lower (non-injected) eyelid in either eye, which was in fact expected though not previously evaluated. The average eyelid FA at baseline was 231.30 mm2 in CG and 255.66 mm2 in FG. Two weeks after treatment with BTA, the corresponding values were 184.02 and 185.60 mm2. As the difference in FA was significant, we believe the symptoms of corneal exposure experienced by many patients are probably better correlated to the FA parameter than to the exophthalmometry measurements or eyelid position alone, although the matter was not dealt in detail in this study.
Our study indicated a favourable effect of BTA treatment on temporal lid flare. A previous study suggested that because the lateral fibres of the levator muscle are more numerous and hypertrophied in TED, they may be the primary reason for the flare observed in such patients.17 Our data support this concept in that the UTA was significantly greater than the UNA in both groups of patients. Following BTA injection we observed a marked reduction in the difference between UTA and UNA. As UTA was more reduced than UNA, post-injection appearance was usually closer to normal appearance, with a dramatic reduction in temporal eyelid flare. Presumably, BTA improved lid contour positioning simply by reducing excessive LF.
Finally, this study is the first to investigate the effect of BTA on the levator function. Our data show a reduction in LF after BTA in both study groups, indicating that the effect of the drug occurs at least in part by neuromuscular blockade of this muscle.
According to the literature, BTA injection in the lid may uncommonly be associated with side effects such as ecchymosis and oedema at the application site, dry eye, epiphore, ptosis and diplopia.3 In the current study, partial ptosis was observed in five out of 24 patients and lagophthalmos and ecchymosis at the injection site in one out of 24 patients. The percentage of post-treatment ptosis reported in the literature varies considerably, ranging from none out of 10 patients in one series11 up to 50% in one case series.8 We believe this disparity is largely the result of variation in treatment regimens and in degree of eyelid retraction. Our data indicate that when five units of BTA are used, the percentage of patients developing ptosis is small and the manifestation is usually short-lived.
In conclusion, our study shows that five units of BTA injected into the upper eyelid is effective at reducing ULR and eyelid FA and at improving upper eyelid contour by reducing excessive LF. Our study also indicates that BTA is effective in both the congestive and the fibrotic stage of the disease, although less so in the former. Although treatment is usually temporary, it is easy to administer as an outpatient procedure and is associated with very few side effects. Thus, BTA injection represents an attractive alternative for improving cosmesis as well as the symptoms related to corneal exposure in patients with eyelid retraction from TED who decline or are ineligible for eyelid surgery.
References
Bartley GB, Fatourechi V, Kadrmas EF, Jacobsen SJ, Ilstrup DM, Garrity JA et al. Clinical features of Graves' ophthalmopathy in an incidence cohort. Am J Ophthalmol 1996; 121: 284–290.
Chee E, Chee SP . Subconjunctival injection of triamcinolone in the treatment of lid retraction of patients with thyroid eye disease: a case series. Eye 2008; 22: 311–315.
Uddin JM, Davies PD . Treatment of upper eyelid retraction associated with thyroid eye disease with subconjunctival botulinum toxin injection. Ophthalmology 2002; 109: 1183–1187.
Gay AJ, Wolkstein MA . Topical guanethidine therapy for endocrine lid retraction. Arch Ophthalmol 1966; 76: 364–367.
Hurwitz JJ, Rodgers KJ . Prevention and management of postoperative lateral upper-lid retraction in Graves' disease. Can J Ophthalmol 1983; 18: 329–332.
Scott AB . Injection treatment of endocrine orbital myopathy. Doc Ophthalmol 1984; 58: 141–145.
Scott AB, Rosenbaum A, Collins CC . Pharmacologic weakening of extraocular muscles. Invest Ophthalmol 1973; 12: 924–927.
Ebner R . Botulinum toxin type A in upper lid retraction of Graves' ophthalmopathy. J Clin Neuroophthalmol 1993; 13: 258–261.
Biglan AW . Control of eyelid retraction associated with Graves' disease with botulinum A toxin. Ophthalmic Surg 1994; 25: 186–188.
Ozkan SB, Can D, Soylev MF, Arsan AK, Duman S . Chemodenervation in treatment of upper eyelid retraction. Ophthalmologica 1997; 211: 387–390.
Traisk F, Tallstedt L . Thyroid associated ophthalmopathy: botulinum toxin A in the treatment of upper eyelid retraction--a pilot study. Acta Ophthalmol Scand 2001; 79: 585–588.
Shih MJ, Liao SL, Lu HY . A single transcutaneous injection with Botox for dysthyroid lid retraction. Eye 2004; 18: 466–469.
Dintelmann T, Sold J, Grehn F . Botulinum toxin injection-treatment of upper lid retraction in thyroid eye disease. Ophthalmologe 2005; 102: 247–250.
Morgenstern KE, Evanchan J, Foster JA, Cahill KV, Burns JA, Holck DE et al. Botulinum toxin type a for dysthyroid upper eyelid retraction. Ophthal Plast Reconstr Surg 2004; 20: 181–185.
Bartley GB, Gorman CA . Diagnostic criteria for Graves' ophthalmopathy. Am J Ophthalmol 1995; 119: 792–795.
Cruz AA, Coelho RP, Baccega A, Lucchezi MC, Souza AD, Ruiz EE . Digital image processing measurement of the upper eyelid contour in Graves disease and congenital blepharoptosis. Ophthalmology 1998; 105: 913–918.
Cruz AA, Akaishi PM, Coelho RP . Quantitative comparison between upper eyelid retraction induced voluntarily and by Graves orbitopathy. Ophthal Plast Reconstr Surg 2003; 19: 212–215.
Gay AJ, Salmon ML, Windsor CE . Hering's law, the levators, and their relationship in disease states. Arch Ophthalmol 1967; 77: 157–160.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Costa, P., Saraiva, F., Pereira, I. et al. Comparative study of Botox® injection treatment for upper eyelid retraction with 6-month follow-up in patients with thyroid eye disease in the congestive or fibrotic stage. Eye 23, 767–773 (2009). https://doi.org/10.1038/eye.2008.165
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2008.165
Keywords
This article is cited by
-
Nonsurgical treatment for upper eyelid retraction in patients with inactive Graves’ orbitopathy
International Ophthalmology (2023)
-
Thyroid eye disease: current and potential medical management
International Ophthalmology (2020)
-
A Comparative Study of Full-Thickness Blepharotomy Versus Transconjunctival Eyelid Lengthening in the Correction of Upper Eyelid Retraction in Graves’ Orbitopathy
Aesthetic Plastic Surgery (2018)
