
Abstract
Purpose
To determine the relationship between ocular hypertension and glaucoma in patients with Graves' orbitopathy.
Methods
A total of 107 patients with a diagnosis of Graves' orbitopathy, followed at the Oculoplasty sector of the University Hospital, Medical School of Ribeirão Preto, were evaluated by applanation tonometry, computed visual campimetry (Humphrey 30-2, Full Threshold) and analysis and photographic documentation of the optic nerve. The patients considered to have the suspicion of glaucoma were re-evaluated 1 year later for diagnostic confirmation or exclusion.
Results
A 3.74% prevalence of ocular hypertension (four patients) and a 2.8% prevalence of glaucoma (three patients) was observed. When considering only patients older than 40 years, the prevalence of ocular hypertension was 5.4% (four patients) and the prevalence of glaucoma was 4.76% (three patients).
Conclusion
The present study did not reveal a statistically significant difference in the prevalence of ocular hypertension or glaucoma between patients with Graves' orbitopathy and the general population.
Similar content being viewed by others


Introduction
Graves' orbitopathy (GO) is an autoimmune disease characterized by the presence of eyelid retraction, proptosis and restrictive strabismus.1, 2 Most patients with GO have autoimmune thyroid dysfunctions, especially hyperthyroidism or Graves' disease (GD), which occurs in 90% of the cases.3 Although there is a strong temporal relationship between the onset of hyperthyroidism and orbitopathy,4 a large number of patients with GD only show minimal signs of orbitopathy. Depending on the sensitivity of the method of orbitopathy detection the prevalence of eye disease in unselected patients with GD ranges from 25 to 70%.1, 5
Intraocular hypertension is a common finding in some patients with GO. Several mechanisms have been implicated in the raise of intraocular pressure. Hypertrophy of the extraocular muscles may induce a marked orbital congestion and increase the episcleral venous pressure.6, 7 Restrictive fibrosis of the inferior rectus muscle causes mechanical compression in the primary position of gaze, which leads to abnormal pressure readings in the slit lamp. Another mechanism that may also contribute to the increase in intraocular pressure, is the accumulation of mucopolysaccharides in the network of aqueous drainage, which would reduce drainage of the aqueous humor.7
The prevalence of ocular hypertension and glaucoma in patients with GO has been studied, with controversial results.
The objective of the present study was to determine the prevalence of glaucoma and ocular hypertension in patients with a diagnosis of GO.
Materials and methods
We evaluated 107 consecutive patients with a diagnosis of Graves' orbitopathy seen at the Oculoplasty sector of the University Hospital, Medical School of Ribeirão Preto. The diagnosis of GO was based on the criteria of Bartley and Gorman,2 which establish the clinical diagnosis of GO in patients who present eyelid retraction associated with at least one of the following signs: thyroid dysfunction, proptosis, strabismus or optic neuropathy, after the exclusion of other possible causes When there is no eyelid retraction, the diagnosis of GO can be considered if some of the signs mentioned above are associated with thyroid dysfunction in the absence of other causal factors.
A comprehensive ophthalmic evaluation was performed in all patients including aplanation tonometry, biomicroscopy of the optic nerve head with digital photography and visual campimetry (Humphrey campimeter, 30-2 full threshold strategy). All examinations were performed by one examiner and the findings were re-evaluated by three glaucoma specialists who divided the sample in three categories: normal, glaucoma and glaucoma suspect.
The diagnosis of glaucoma was based on the presence of two of the following parameters: indicative signs of glaucoma in optic nerve head, ocular hypertension and, or visual field losses. The criteria for inclusion in ocular hypertension group was intraocular pressure above 21 mmHg without other parameters indicative of glaucoma.
The patients who received a diagnosis of glaucoma suspect (borderline) continued to be followed at the responsible outpatient sectors of the University Hospital and were re-evaluated about 1 year later by evaluation of GD status, refraction examination, determination of risk factors, repeated tonometry and campimetry and a new photographic documentation of the optic nerve. These new tests were again evaluated by the examiners together with the previous tests for the observation of possible progression of the optic nerve alterations, and/or visual field losses, characteristic of glaucoma.
Statistical analysis was performed using Fisher exact test and, when one of the numbers was less than five, the χ2 test.
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during this research.
Results
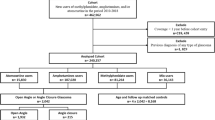
Of the 107 patients with GO submitted to exams for the diagnosis of glaucoma, 20 (18.7%) were males and 87 (81.3%) were females. Mean age was 41.57 years and median age 42 years (range: 10–74 years).
Ocular hypertension in at least one eye was detected in four patients (3.74%; Confidence interval 95: 1.03–9.30%), all of them females. The physical comorbidities presented are anaemia (2) and hepatitis (1).
The tests and retinographies of these patients were evaluated by three examiners (specialists in glaucoma) and, on the basis of the diagnosis of at least two examiners, 84 were considered to be normal, 22 suspected and one received a diagnosis of glaucoma.
The 22 patients considered to be suspected were then submitted to a new evaluation 1 year later to verify the evolution of GD and to determine or exclude the diagnosis of glaucoma. Eighteen of these 22 patients do not present progression of the GD; GD became more severe in one patient; and three patients were submitted to orbital decompression surgery. The examiners evaluated again the glaucoma tests together with the previous ones and concluded that two of the 22 patients re-evaluated had a diagnosis of glaucoma. Thus, of the total number of 107 patients with GO evaluated, three had a diagnosis of glaucoma, corresponding to 2.80% (Confidence Interval 95: 0.58–7.98%) of the total population. When only patients older than 40 years were considered, the prevalence of intraocular hypertension was 5.4% and the frequency of glaucoma was 4.76%.
Discussion
Glaucoma is the second most frequent cause of blindness in the world. The estimate is that by 2010 there will be 60.5 million people with glaucoma, with the number increasing to 79.6 million in 2020, and that bilateral blindness due to glaucoma will affect 8.4 million people by 2010 and 11.2 million by 2020.8
Several studies on the prevalence of glaucoma have been conducted in different countries, but the frequency of glaucoma in the general population is estimated at 1.5–2%.9 In the US, the prevalence of open angle glaucoma in the population older than 40 years is estimated at 1.86%.10 In a study conducted in Spain on persons aged 40–79 years, the prevalence of primary open angle glaucoma was found to be 2.1%.11
In Brazil there are no multicenter studies for the determination of the prevalence of glaucoma. Two studies were conducted in the Southeast and South regions of the country. In the first, a prevalence of 1.48% was observed among 8061 patients starting at 40 years of age, increasing to 2.07% above the age of 50 years.12 In the second, conducted on 1953 patients older than 40 years, 79 cases of glaucoma were detected (4.05%), with 73 being patients with primary open angle glaucoma and six (0.31%) having a diagnosis of secondary glaucoma or narrow angle glaucoma.13
In the present study, there was a 3.74% prevalence of ocular hypertension and a 2.80% prevalence of glaucoma in patients with GO, values similar to those observed in the general population. Considering only the patients older than 40 years the prevalence was found to be higher than the other studies, except the one carried out by Sakata et al.13
In a retrospective study of 482 patients with GO, Kalmann and Mourits14 detected a 3.9% prevalence of intraocular hypertension in these patients compared to a prevalence of 1.6% in the general population. A study15 carried out in Pittsburgh on 500 patients with GO revealed a 24% prevalence of ocular hypertension compared to 5% in the general population. In that study15 only seven patients were classified as glaucomatous and two patients showed progressive abnormalities of the visual field and optic disc. Ohtsuka and Nakamura observed a 22% prevalence of ocular hypertension in patients with GO16 and a 13% prevalence of glaucoma in patients with GD (Table 1).17
Despite the controversial results obtained thus far, intraocular pressure should be carefully monitored in patients with GO. It is necessary to point out that the number of participants of the present study is small, and it is a limitation. However, the results indicate that the progressive glaucomatous changes of the optic nerve and visual fields are probably not more common among these patients than in the general population.
Treatment of GO, particularly orbital decompression, may have a beneficial effect on intraocular pressure. Patients with ocular hypertension should be monitored for changes in the optic disc and visual field. Anti-glaucoma medical therapy may be necessary, but surgical treatment of glaucoma is not necessary for most patients with GO and ocular hypertension.18, 19, 20
References
Burch HB, Wartofsky L . Graves' ophthalmopathy: current concepts regarding pathogenesis and management. Endocr Rev 1993; 14: 747–793.
Bartley GB, Gorman CA . Diagnostic criteria for Graves' ophthalmopathy. Am J Ophthalmol 1995; 119: 792–795.
Bartley GB, Fatourechi V, Kadrmas EF, Jacobsen SJ, Ilstrup DM, Garrity JA et al. Chronology of Graves' ophthalmopathy in an incidence cohort. Am J Ophthalmol 1996; 121: 426–434.
Gorman CA . Temporal relationship between onset of Graves' ophthalmopathy and diagnosis of thyrotoxicosis. Mayo Clin Proc 1983; 58: 515–519.
Feldon SE . Graves' ophthalmopathy. Is it really thyroid disease? Arch Intern Med 1990; 150: 948–950.
Dallow RL, Netland PA . Management of thyroid ophthalmology (Graves' disease). In: Albert DM, Jakobiek FA (eds). Principles and Practice of Ophthalmology. WB Saunders: Philadelphia, 1994, pp 1905–1922.
Higginbotham EJ . Glaucoma associated with increased episcleral venous pressure. In: Albert DM, Jakobiek FA, Azar DT, Gragoudas E, Power SM, Robinson NL (eds). Principles and Practice of Ophthalmology. WB Saunders: Philadelphia, 2000, pp 2781–2792.
Quigley HA, Broman AT . The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol 2006; 90: 262–267.
Giampani J . Hereditariedade e Genética. In: Susanna Junior R (eds). Glaucoma (Manual CBO). Cultura Médica: Rio de Janeiro, 1999, pp 9–12.
Friedman DS, Wolfs RC, O'Colmain BJ, Klein BE, Taylor HR, West S et al. Prevalence of open-angle glaucoma among adults in the United States. Arch Ophthalmol 2004; 122: 532–538.
Anton A, Andrada MT, Mujica V, Calle MA, Portela J, Mayo A . Prevalence of primary open-angle glaucoma in a Spanish population: the Segovia study. J Glaucoma 2004; 13: 371–376.
Ghanem CC . Levantamento de casos de Glaucoma em Joinville—Santa Catarina. Arq Bras Oftalmol 1989; 52: 40–43.
Sakata K, Scapucin L, Sakata LM, Carvalho ACA, Selonke I, Sakata VM et al. Projeto glaucoma—resultados parciais 2000 na região de Piraquara—PR. Arq Bras Oftalmol 2002; 65: 333–337.
Kalmann R, Mourits MP . Prevalence and management of elevated intraocular pressure in patients with Graves' orbitopathy. Br J Ophthalmol 1998; 82: 754–757.
Cockerham KP, Pal C, Jani B, Wolter A, Kennerdell JS . The prevalence and implications of ocular hypertension and glaucoma in thyroid-associated orbitopathy. Ophthalmology 1997; 104: 914–917.
Ohtsuka K . Intraocular pressure and proptosis in 95 patients with Graves ophthalmopathy. Am J Ophthalmol 1997; 124: 570–572.
Ohtsuka K, Nakamura Y . Open-angle glaucoma associated with Graves disease. Am J Ophthalmol 2000; 129: 613–617.
King JS, Netland PA . Glaucoma in thyroid eye disease. In: Dutton JJ, Haik BG (eds). Thyroid Eye Disease, Diagnosis and Treatment. Marcel Dekker Inc.: New York, 2002, pp 319–324.
Danesh-Meyer HV, Savino PJ, Deramo V, Sergott RC, Smith AF . Intraocular pressure changes after treatment for Graves'orbitophathy. Ophthalmology 2001; 108: 145–150.
Crespi J, Rodriguez F, Bull JA . Presión intraocular post-tratamiento de la oftalmolpatia tireoidea. Arch Soc Esp Ophthalmol 2007; 82: 691–696.
Acknowledgements
This study was financially supported by CAPES, Brazil. We acknowledge our collaboration with Professor Dr Jayter Silva de Paula, Professor Dr Eduardo Melani Rocha and Dr Daniela Felipe Crosta.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
da Silva, F., de Lourdes Veronese Rodrigues, M., Akaishi, P. et al. Graves' orbitopathy: frequency of ocular hypertension and glaucoma. Eye 23, 957–959 (2009). https://doi.org/10.1038/eye.2008.155
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2008.155
Keywords
This article is cited by
-
The outcomes of endoscopic orbital decompression combined with fat decompression for thyroid-associated ophthalmopathy
BMC Ophthalmology (2023)
-
Ocular hypertension in patients with active thyroid-associated orbitopathy: a predictor of disease severity, particularly of extraocular muscle enlargement
Graefe's Archive for Clinical and Experimental Ophthalmology (2022)
-
Evaluation of the corneal biomechanical properties and corneal thickness in patients with Graves’ orbitopathy
International Ophthalmology (2022)
-
Atopic dermatitis as a risk factor for severe visual field loss in youth—a retrospective cohort study of glaucoma under steroid treatment
Graefe's Archive for Clinical and Experimental Ophthalmology (2021)
-
Thyroid-stimulating immunoglobulins indicate the onset of dysthyroid optic neuropathy
Journal of Endocrinological Investigation (2015)
