
Abstract
OBJECTIVE: To identify limitations of current strategies for intrapartum prophylaxis of neonatal early-onset group B streptococcal infection.
METHODS: Retrospective review of infants with culture-proven early-onset group B streptococcal infection admitted to two nurseries and their mothers from July 1992, when ACOG and AAP guidelines for intrapartum prophylaxis were first issued, through December 2001. Information was recorded regarding clinical risk factors for early-onset group B streptococcal infection, collection and processing of specimens to assess maternal colonization, delivery of prophylaxis, duration of hospitalization before delivery, and outcome.
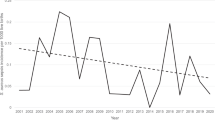
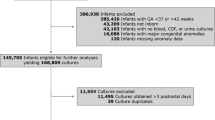
RESULTS: Among 92 infants with early-onset group B streptococcal infection admitted from 23 institutions, 68 had received no intrapartum prophylaxis. Of these 68 who received no prophylaxis, 34 had identifiable risk factors before delivery (32 clinical, two positive maternal culture), while 34 had no risk factors. Prenatal culture for group B streptococcal colonization was performed in 22 of these women. Of the 18 cultures that were negative for group B streptococcus, 15 were obtained using suboptimal culture technique or were collected more than 6 weeks before delivery. Of the 68 with no prophylaxis, 14 required extracorporeal membrane oxygenation and three died. Of the 24 who received some intrapartum prophylaxis, nine had received ≥two doses for ≥4 hours immediately before delivery. Among the 24 receiving some intrapartum prophylaxis, two required extracorporeal membrane oxygenation and one died. No deaths occurred in those who received >4 hours of prophylaxis, although one such infant required extracorporeal membrane oxygenation. After the CDC guidelines were issued in May 1996, there was a decrease both in the number of cases of early-onset group B streptococcal infection (56 versus 36) as well as in the number with clinical risk factors but no intrapartum prophylaxis (24/56 (43%) versus 5/28 (18%)).
CONCLUSIONS: The use of clinical risk factors alone will inevitably result in missed opportunity for intrapartum antibiotic prophylaxis. With maternal screening, false-negative results will be reduced but not necessarily eliminated by assuring that specimens are obtained from proper sites using selective media within 6 weeks of delivery. Better strategies are needed to assure timely administration when prophylaxis is indicated. The nine neonates with early-onset group B streptococcal infection despite intrapartum antibiotics for the recommended duration illustrate that disease may occur even when guidelines are implemented appropriately.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

References
Boyer KM, Gotoff SP . Prevention of early-onset neonatal group B streptococcal disease with selective intrapartum chemoprophylaxis. N Engl J Med 1986;314:1665–1669.
Boyer KM, Gadzala CA, Kelly PD, Gotoff SP . Selective intrapartum chemoprophylaxis of neonatal group B streptococcal early-onset disease. III. Interruption of mother-to-infant transmission. J Infect Dis 1983;148:810–816.
Ohlsson A, Myhr TL . Intrapartum chemoprophylaxis of perinatal group B streptococcal infections: a critical review of randomized controlled trials. Am J Obstet Gynecol 1994;170:910–917.
American College of Obstetricians and Gynecologists. Group B Streptococcal Infections in Pregnancy. Technical Bulletin Number 170. Washington, DC: The American College of Obstetricians and Gynecologists; 1992. p 1–5.
American Academy of Pediatrics, Committee on Infectious Diseases and Committee on Fetus and Newborn. Guidelines for prevention of group B streptococcal infection by chemoprophylaxis. Pediatrics. 1992;90:775–778.
Jafari HS, Schuchat A, Hilsdon R, Whitney C, Toomey K, Wenger J . Barriers to prevention of perinatal group B streptococcal disease. Pediatr Infect Dis J 1995;14:662–667.
American College of Obstetricians and Gynecologists. Survey shows continued confusion over management of GBS in pregnancy. ACOG Newslett 1994;1:10.
Rosenstein N, Schuchat A . Opportunities for prevention of perinatal group B streptococcal disease: a multi-state surveillance analysis. The Neonatal Group B Streptococcal Disease Study Group. Obstet Gynecol 1997;90:901–906.
Mohle-Boetani JC, Schuchat A, Plikaytis BD, Smith JD, Broome CV . Comparison of prevention strategies for neonatal group B streptococcal infection. A population-based economic analysis. JAMA 1993;270:1442–1448.
Centers for Disease Control. Laboratory practices for prenatal group B streptococcal screening and reporting — Connecticut, Georgia, and Minnesota, 1997–1998. MMWR 1999;48:426–428.
Locksmith GJ, Clark P, Duff P . Maternal and neonatal infection rates with three different protocols for prevention of group B streptococcal disease. Am J Obstet Gynecol 1999;180:416–422.
Mercer BM, Ramsey RD, Sibai BM . Prenatal screening for group B streptococcus. I. Impact of antepartum screening on antenatal prophylaxis and intrapartum care. Am J Obstet Gynecol 1995;173:837–841.
Gilbert GL, Isaacs D, Burgess MA et al. Prevention of neonatal group B streptococcal sepsis: is routine antenatal screening appropriate. Aust NZ J Obstet Gynecol 1995;35:120–126.
Centers for Disease Control. Prevention of perinatal group B streptococcal disease: a public health perspective. MMWR 1996;45(RR-7):1–24.
Schrag S, Zywicki S, Farley MM, et al. Group B streptococcal disease in the era of intrapartum antibiotic prophylaxis. N Engl J Med 2000;342:15–20.
Centers for Disease Control. Adoption of hospital policies for prevention of perinatal group B streptococcal disease — United States, 1997. MMWR 1998;47:665–670.
Whitney CJ, Plikaytis BD, Gozansky WS, Wenger JD, Schuchat A . Prevention practices for perinatal group B streptococcal disease: A multi-state surveillance analysis. Neonatal Group B Streptococcal Disease Study Group. Obstet Gynecol 1997;89:28–32.
Factor SH, Whitney CG, Zywicki SS, Schuchat A . Effects of hospital policies based on 1996 group B streptococcal disease consensus guidelines. The Active Bacterial Core Surveillance Team. Obstet Gynecol 2000;95:377–382.
Centers for Disease Control. Adoption of perinatal group B streptococcal disease prevention recommendations by prenatal care providers — Connecticut, and Minnesota, 1998. MMWR 2000;49:228–232.
Philipson A, Sabath LD, Charles D . Transplacental passage of erythromycin and clindamycin. N Engl J Med 1973;288:1219–1221.
Schuchat A, Deaver-Robinson K, Plikaytis BD, Zangwill KM, Mohle-Boetani J, Wenger JD . Multi-state case–control study of maternal risk factors for neonatal group B streptococcal disease. The Active Surveillance Study Group. Pediatr Infect Dis J 1994;13:623–629.
Gibbs RS, McDuffie RS, McNabb F, Fryer GE, Miyoshi T, Merenstein G . Neonatal group B streptococcal sepsis during 2 years of a universal screening program. Obstet Gynecol 1994;84:496–500.
Boyer KM, Gadzala CA, Kelly PD, Burd LI, Gotoff SP . Selective intrapartum chemoprophylaxis of neonatal group B streptococcal early-onset disease. II. Predictive value of prenatal cultures. J Infect Dis 1983;148:802–809.
Brozanski BS, Jones JG, Krohn MA, Sweet RL . Effect of a screening-based prevention policy on prevalence of early-onset group B streptococcal sepsis. Obstet Gynecol 2000;95:496–501.
Weiner GM, Barks JDE, Wright EJ, Faix RG . Improving the timing of antibiotic administration to high-risk newborns. J Perinatol 1998;18:230–233.
Meadow WL, Lantos J, Tanz RR, Mendez D, Unger R, Wallskog P . Ought “standard care” be the “standard of care”? A study of the time to administration of antibiotics in children with meningitis. Am J Dis Child 1993;147:40–44.
Bryan CS, Reynolds KL, Crout L . Promptness of antibiotic therapy in acute bacterial meningitis. Ann Emerg Med 1986;15:544–547.
Talan DA, Guterman JJ, Overturf GD, Singer C, Hoffman JR, Lambert B . Analysis of emergency department management of suspected bacterial meningitis. Ann Emerg Med 1989;18:856–862.
Pearlman MD, Pierson CL, Faix RG . Frequent resistance of clinical group B streptococci isolates to clindamycin and erythromycin. Obstet Gynecol 1998;92:258–261.
Ascher DP, Becker JA, Yoder BA et al. Failure of intrapartum antibiotics to prevent culture-proved neonatal group B streptococcal sepsis. J Perinatol 1993;13:212–216.
Centers for Disease Control and Prevention. Prevention of perinatal group B streptococcal disease. Revised guidelines from CDC. MMWR 2002;55(RR-11):1–23.
Schimmel MS, Samueloff A, Eidelman AI . Prevention of neonatal group B streprococcal infections. Is there a rational prevention strategy? Clin Perinatol 1998;25:687–697.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Pinto, N., Soskolne, E., Pearlman, M. et al. Neonatal Early-onset Group B Streptococcal Disease in the Era of Intrapartum Chemoprophylaxis: Residual Problems. J Perinatol 23, 265–271 (2003). https://doi.org/10.1038/sj.jp.7210899
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.jp.7210899
This article is cited by
-
Risk factors for group B streptococcal disease in neonates of mothers with negative antenatal testing
Journal of Perinatology (2017)
-
Prevention of Early-onset GBS Sepsis: Evaluation of a Changing Paradigm
Journal of Perinatology (2003)
