
Abstract
A solution of perfluorohexyloctane and silicone oil with a specific gravity of 1.06 g/cm3 (Densiron-68) has similar properties as conventional silicone oil (SO) in terms of the shape of the bubble and its ability to act as an internal tamponade agent. We conducted a case–control study to compare the postoperative intraocular pressure (IOP) in patients treated with Densiron-68 with those treated with SO.
Methods
Seventy-one eyes of 71 patients and 57 eyes of 57 patients who had received Densiron-68 and SO, respectively, were included in our study. Both groups were found to have matched for their preoperative comorbidities (diabetes, glaucoma, phakic status, and refractive errors). IOP at first day, between seventh and fourteenth day, and at 4 week postoperatively was recorded.
Results
The mean IOP was higher in patients treated with Densiron-68 at day 1 and between seventh and fourteenth day postoperatively (P=0.05 and 0.01, respectively). By the 4th week, the IOP difference between the two groups was insignificant (P=0.17). The difference in the two groups could still be clinically significant and the raised IOP in Densiron-68 group was more difficult to treat in some cases.
On day 1, nine eyes (12.7%) in the Densiron-68 group and two eyes (3.5%) in the SO group had IOP greater than 30 mmHg. At 4 weeks, IOP of more than 30 mmHg was seen in nine eyes (12.7%) in the Densiron-68-treated group and in one eye (1.8%) in the SO group.
Conclusion
The use of Densiron-68 was associated with a higher IOP in the early postoperative period when compared with SO.
Similar content being viewed by others
Introduction
Internal tamponade agents such as silicone oil (SO) and long-acting gases used for retinal detachment (RD) are lighter than water and provide good support for the superior retina. Proliferative vitreoretinopathy (PVR), however, has the propensity for the inferior retina.1 Conventional SO does not provide very effective inferior support unless it completely fills the vitreous cavity. Therefore, various heavy tamponade agents with a specific gravity higher than water have been tried in cases of retinal breaks situated in the inferior retina, especially in the presence of PVR.
Perfluorohexyloctane (F6H8) is a clear, homogenous semifluorinated alkane initially introduced as an SO solvent to remove SO droplets adherent to intraocular lenses.2, 3 It is heavier than water and has a low viscosity of 2.5 mPa. It was found to be well tolerated for up to 3 months in a rabbit model.4 In human beings, however, the use of this agent as a long-term tamponade was found to be associated with dispersion, inflammation, and epiretinal membrane formation. These complications were in turn thought to be related to the low viscosity of the agent.5
Densiron-68 is a solution of SO and F6H8. By Adding F6H8 to silicone, the mixture has a specific gravity greater than 1.06 g/cm3 and a viscosity of 1387 cs. It is, therefore, heavier than water and sufficiently viscous to have a much lower propensity for dispersion (compared with F6H8 on its own). We conducted an in vitro study that demonstrated that in a polymethylmethacrylate model eye chamber, a solution with a specific gravity of 1.06 g/cm3 has similar physical properties to SO in terms of the shape of the bubble and its ability to act as an internal tamponade agent.5 This is commercially available as Densiron-68 and occasionally referred to as heavy oil.6
We used this agent and conducted a pilot clinical study on its efficacy and monitored the complications. This pilot study involved 42 cases recruited between Rotterdam and Liverpool.7 In this study, Densiron-68 was used in patients with RD arising from inferior retinal breaks, in patients incapable of sustaining a head-down posture, and in cases complicated by PVR. At 1 week and 1 month after heavy silicone oil (HSO) operation, six patients (14%) had raised intraocular pressure (IOP) and at 3 months after oil removal, three patients (7%) had IOP higher than 30 mmHg. Similarly, Wolf et al found that postoperatively IOP was raised higher than 30 mmHg in four (12%) of 33 eyes treated with Oxane Hd (Baush and Lomb), which is a mixture of silicone and semifluorinated alkenes with a specific gravity of 1.03 g/cm3.8 In a pilot study by Tognetto and co-workers, the authors found an early postoperative ocular hypertension in eight patients (30.7%) treated with HSO, which was easily controlled using topical antiglaucoma medications or systemic carbonic anhydrase inhibitors.9
There is an initial clinical impression that the use of Densiron-68 may be associated with an early postoperative IOP rise. It was not possible to know whether the IOP rise after surgery was due to the surgery or whether it was related to the Densiron-68. We therefore conducted this case–control study to compare patients treated with Densiron-68 with those treated with conventional SO.
Materials and methods
A case–control study was carried out comparing 71 eyes of 71 patients with RD who received Densiron-68 with 57 eyes of 57 patients with RD who received conventional SO. All the surgeries in the Densiron-68 group were performed between January 2003 and March 2005, whereas those in the conventional SO group were before November 2004. The inclusion criteria consisted of rhegmatogenous or tractional retinal detachment with or without PVR. The exclusion criteria were severe systemic disease, pregnancy, and ocular disease other than retinal detachment.
Thirty patients with RD in conventional SO group were complicated by PVR: seven eyes PVR A, 10 eyes PVR B, and 13 eyes PVR CP. Thirty-two patients with RD in Densiron-68 group were complicated by PVR: three eyes PVR A, nine eyes PVR B, and 20 eyes PVR CP. All the operations were performed by consultants or vitreoretinal fellows using Alcon Accurus®. Densiron-68 (Fluoron Company, Neu-Ulm, Germany) with an interfacial tension against water of 40.82 mN/m at 25°C, a specific gravity of 1.06 g/cm3 and a viscosity of 1387 cs was used. Conventional SO used was of 1000, 5000, or 5700 cs viscosity at 25°C with a specific gravity of 0.965 g/cm3 and an interfacial tension against water of 35.5 mN/m at 25°C.
In the Densiron-68 group, pars plana vitrectomy (PPV) was performed in 56 eyes; 15 of the 71 eyes had conventional SO already in situ and the surgery involved first removing this oil, performing the surgery on the retina, and injecting the Densiron-68. The surgery-involved epiretinal membrane peeling was carried out in seven eyes and PPV was combined with phacoemulsification with intraocular lens implant in five eyes and lensectomy in two eyes. Two eyes underwent removal of subretinal bands.
In the conventional SO group, PPV was performed in 52 eyes. In the other five eyes, there was oil in situ, which was first removed. PPV was combined with phacoemulsification and intraocular lens implantation in five eyes and lensectomy in one eye. Two eyes had epiretinal membrane peeling.
IOP was recorded using the Goldmann applanation tonometer on day 1, between seventh and fourteenth day, and at 4 weeks postoperatively in all patients. Surgical success was defined as complete retinal attachment after oil removal. Statistical analysis was performed using χ2-test, student's t-test and analysis of variance (SPSS ver12.0.01). As this work was performed as an audit, our hospital did not require the study to have a specific ethical approval.
Results
Matching
The mean age of patients who received Densiron-68 was 58.1±17.9 years (range 13–87 years) and those who received conventional SO was 54.8±18.4 years (range 15–81 years). Both groups of patients were well matched preoperatively for age, gender, and other features including diabetes, preexisting glaucoma, rubeosis, peripheral iridectomy, lens status (phakic, pseudophakic, and aphakic), and refractive error (hypermetropia and myopia). There was, however, a significant difference in the extent of RD preoperatively in each treatment group as shown in Table 1. The surgery performed on both groups was similar, except that there was a higher percentage of patients (42.3%, 30 patients) treated with retinectomy in the Densiron-68 group as compared with the conventional SO group (22.8%, 13 patients). Additionally, three patients had encirclement in the conventional SO group and none in the Densiron-68-treated group.
Intraocular pressure
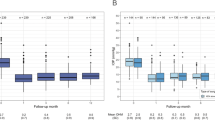
The mean, range, and standard deviations of the IOP in the Densiron-68 group and the conventional SO group are summarized in Table 2. IOP was significantly higher in the group treated with Densiron-68 compared with the group treated with conventional SO at day 1 and between the seventh and fourteenth postoperative days. The difference was not significant at 4 weeks.
On day 1, nine eyes (12.7%) in the Densiron-68 group and two eyes (3.5%) in the conventional SO group had IOP greater than 30 mmHg (Table 3). Between 7 and 14 days, 14 eyes (19.7%) in the Densiron-68 group and three eyes (5.3%) in the conventional SO group had IOP greater than 30 mmHg. At 4 weeks, IOP of more than 30 mmHg was seen in nine eyes (12.7%) in the Densiron-68-treated group and one eye (1.8%) in the conventional SO group. On day 1, the median IOP in the Densiron-68 group was 20 mmHg (range 8–58 mmHg) as compared with 19 mmHg (range 8–32 mmHg) in the conventional SO group. At 4 weeks, the median in Densiron-68 group was 18 mmHg (range 5–48 mmHg) while that in conventional SO group was 16 mmHg (range 7–37 mmHg). In both groups, some patients improved while others worsened over the period of 4 weeks.
The patients in the Densiron-68 group did not require more frequency and duration of steroid use as compared with the conventional SO group, although there were a higher percentage of patients with severe inflammation in the Densiron-68 group.
Postoperatively, 30 patients (42.3%) in the Densiron-68 group required topical antiglaucoma medication to control IOP. The patients were started on treatment when their IOP was greater than 26 mmHg. Of these, six patients required one medication, 12 patients required two medications, eight patients required three medications, three patients required four medications, and one patient required five medications. In addition, two patients were treated with cyclodiode therapy on day 4 and day 24, and one patient required partial removal of oil to control IOP on day 1. Of the 30 patients who were started on treatment, nine patients (30%) did not respond well to the treatment. More medications and treatments were added after the first 4 weeks and IOP was then controlled. Of these nine patients, one patient had a history of glaucoma.
In the conventional SO group, 13 patients (22.8%) required topical antiglaucoma drops to control IOP. None of the patients required any surgical intervention and all responded well to the treatment.
Only one of the three patients in the Densiron-68 group with rubeosis had high IOP postoperatively and it was well controlled on medication. None of the patients in the conventional SO group had rubeosis.
Postoperative inflammation
On the first postoperative day, the majority of patients had mild inflammation: 43 eyes (60.6%) in the Densiron-68 group and 34 eyes (59.6%) in the conventional SO group (P=0.916) (Table 4). There were six eyes (8.5%) in the Densiron-68 group and one eye (1.8%) in the conventional SO group with +++ to ++++ postoperative inflammation (P=0.098).
Postoperative anterior chamber shallowing, iris bombe, and oil in the AC
Postoperatively, the anterior chamber (AC) was shallow in three eyes (4.2%) in the Densiron-68-treated group and three (5.3%) eyes in the conventional SO-treated group (Table 4). All of these eyes were pseudophakic. Iris bombe was seen postoperatively in two eyes (2.8%) treated with Densiron-68 and in two eyes (3.5 %) treated with the conventional SO. Eleven eyes (15.5%) in the Densiron-68 group and none in the conventional SO group had oil in AC as small bubbles, within the first week after the surgery. Of these 11 eyes in the Densiron-68 group, two were aphakic and nine were pseudophakic. No attempt was made to make the oil return to the posterior segment as it was present only in form of small bubbles.
Anatomical results
At surgery, complete re-attachment of retina was achieved in all cases in both the groups. The retina was attached in 58 (81.7%) eyes in the Densiron-68 group and 39 (68.4%) eyes in the conventional SO group at the last follow-up. There was no statistically significant difference (P=0.098).
Discussion
Postoperative IOP rise, however, is not uncommon after vitrectomy and SO injection. In the literature, the reported incidence varied from 3 to 40%.10, 11, 12, 13 Silicone study report 4 observed a prevalence of chronically elevated IOP of 8% in patients treated with conventional SO.14 We were not sure whether there was an increased incidence with Densiron-68, thus we were prompted to carry out this case–control study.
The matching of preoperative clinical features was good, although the Densiron-68 group of patients had less extensive retinal detachment (less than two quadrants).
The results suggested that IOP was indeed higher in eyes treated with Densiron-68 as compared with those treated with conventional SO on day 1 and between day 7 and day 14. The difference between the mean IOP was small and although it was statistically different at these time points, was the difference clinically significant? Let us assume that an IOP greater than 30 mmHg was clinically significant. Then this pressure occurred more frequently in Densiron-68 patients than conventional SO patients. The proportion of patients with IOP of 30 mmHg or more on day 1 was 12.7% for Densiron-68 and 3.5% for conventional SO. The raised IOP also seemed to be difficult to treat. Thirty Densiron-68 patients were treated for the raised IOP, nine (30%) did not respond; a number of patients had increasing number of medication; cyclodiode was necessary in two patients and at 4 weeks, there were still 12.7% of patients with IOP greater than 30 mmHg.
What could account for the differences in IOP observed? More Densiron-68 patients were treated by retinectomy during the surgery. Retinectomy is generally associated with postoperative hypotony in the long term. In the immediate postoperative period, however, there may be increased inflammation due to the breakdown of blood-ocular barrier or bleeding associated with cutting the retina. We did observe a higher incidence of severe inflammation in patients treated with Densiron-68. This might be related to the retinectomy or it might be related intrinsically to the Densiron-68. Theelan and Tilanus observed an inflammatory response associated with the use of high-density SO.15
The oil was seen in AC in 11 (15.5%) eyes in the Densiron-68 group and none of the eyes in the conventional SO group. The incidence of this complication was much higher than previously reported in earlier studies by Wong et al7 (7%) and Wolf et al8 (0%). Theoretically, Densiron-68 should have less of a tendency to come into AC because it has a higher interfacial tension against aqueous compared with SO. In the past, we have reported on pupil block glaucoma associated with conventional SO in the AC in phakic and pseudophakic eyes and speculated that this was caused by overfilling of the globe at the end of surgery.16 Oil in AC usually occurs in aphakic eyes and is often associated with hypotony.16 The fact that nine of the 11 eyes were pseudophakic also suggested that the eyes were overfilled.16 When oil was present in AC, high IOP usually ensued and the raised pressure could be difficult to treat.16
In summary, there did seem to be a difference in the IOP response to Densiron-68 as compared with conventional SO. The difference could be clinically significant and the raised IOP could be difficult to treat. This warrants caution for the use of Densiron in the glaucomatous eyes. The cause of raised IOP may be multifactorial including, inflammation and overfilling; the latter at least should be avoided.
References
Singh AK, Glaser BM, Lemor M, Michels RG . Gravity-dependent distribution of retinal pigment epithelial cells dispersed into the vitreous cavity. Retina 1986; 6: 77–80.
Dick HB, Augustin AJ . Solvent for removing silicone oil from intraocular lenses: experimental study comparing various biomaterials. J Cataract Refract Surg 2000; 26: 1667–1672.
Zeana D, Becker J, Kuckelkorn R, Kirchhof B . Perfluorohexyloctane as a long term vitreous tamponade in the experimental animal. Experimental perfluorohexyloctane substitution. Int Ophthalmol 1999; 23 (1): 17–24.
Hiscott P, Magee RM, Colthurst M, Lois N, Wong D . Clinicopathological correlation of epiretinal membranes and posterior lens opacification following perfluorohexyloctane tamponade. Br J Ophthalmol 2001; 85 (2): 179–183.
Wetterquist C, Wong D, Williams R, Stappler T, Herbert E, Freeman S . Tamponade efficiency of perfluorohexyloctane and silicone oil solutions in a model eye chamber. Br J Ophthalmol 2004; 88: 692–696.
Bhisitkul RB, Gonzalez VH . ‘Heavy oil’ for intraocular tamponade in retinal detachment surgery. Br J Ophthalmol 2005; 89 (6): 649–650.
Wong D, Van Meurs JC, Stappler T, Groenwald C, Pearce IA, McGalliard JN et al. A pilot study on the use of a perfluorohexyloctane/silicone oil solution as a heavier than water internal tamponade agent. Br J Ophthalmol 2005; 89: 662–665.
Wolf S, Schon V, Meier P, Wiedemann P . Silicone oil –RNM 3 mixture (heavy silicone oil) as internal tamponade for complicated retinal detachment. Retina 2003; 23: 335–342.
Togenetto D, Minutola D, Sanguinetti G, Ravalico G . Anatomical and functional outcomes after heavy silicone oil tamponade in vitreoretinal surgery for complicated retinal detachment. Ophthalmology 2005; 112: 1574–1578.
Azen SP, Scott IU, Flynn Jr HW, Lai MY, Schwartz S, Trese MT . Silicone oil in the repair of complex retinal detachments. A prospective observational multicenter study. Ophthalmology 1998; 105 (9): 1587–1597.
Honavar SG, Goyal M, Majji AB, Sen PK, Naduvilath T, Dandoma L . Glaucoma after pars plana vitrectomy and silicone oil injection for complicated retinal detachments. Ophthalmology 1999; 106 (1): 169–176.
Al-Jazzaf AM, Netland PA, Charles S . Incidence and management of elevated intraocular pressure after silicone oil injection. J Glaucoma 2005; 14 (1): 40–46.
Henderer JD, Budenz DL, Flynn HW, Schiffman JC, Feuer WJ, Murray TG . Elevated intraocular pressure and hypotony following silicone oil retinal tamponade for complex retinal detachment: incidence and risk factors. Arch Ophthalmol 1999; 117 (2): 189–195.
Barr CC, Lai MY, Lean JS, Linton KL, Trese M, Abrams G et al. Postoperative intraocular pressure abnormalities in the silicone study. Silicone study Report 4. Ophthalmology 1993; 100 (11): 1629–1635.
Theelen T, Tilanus MA, Klevering BJ . Intraocular inflammation following endotamponade with high-density silicone oil. Graefes Arch Clin Exp Ophthalmol 2004; 242 (7): 617–620.
Jackson TL, Thiagarajan M, Murthy R, Snead MP, Wong D, Williamson TH . Pupil block glaucoma in phakic and pseudophakic patients after vitrectomy with silicone oil injection. Am J Ophthalmol 2001; 132 (3): 414–416.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wong, D., Kumar, I., Quah, S. et al. Comparison of postoperative intraocular pressure in patients with Densiron-68 vs conventional silicone oil: a case–control study. Eye 23, 190–194 (2009). https://doi.org/10.1038/sj.eye.6703055
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6703055
Keywords
This article is cited by
-
Anatomical and functional outcomes of short-term DensironXTRA heavy silicone oil for rhegmatogenous retinal detachments: a comparative case series
Scientific Reports (2023)
-
Outcomes of Heavy Silicone Oil (Densiron) compared to Silicone Oil in primary rhegmatogenous retinal detachment: a multivariable regression model
International Journal of Retina and Vitreous (2022)
-
Biocompatibility of intraocular liquid tamponade agents: an update
Eye (2021)
-
Outcome of pediatric retinal detachment using high-density silicone oil
International Ophthalmology (2021)
-
Clinical complications of Densiron 68 intraocular tamponade for complicated retinal detachment
Eye (2010)
