
Abstract
Purpose
To determine the predictive value of early Phase trials (I–II) for the ocular hypotensive efficacy observed in Phases III and IV.
Design
A review of published literature.
Methods
This study evaluated 12 medicines in 65 articles in the literature with at least two phases available.
Results
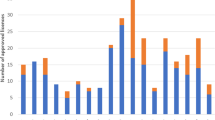
For medicines with Phase I results available (n=3), the average reduction in intraocular pressure (IOP) from untreated baseline was 16%, 26% for Phase II, 26% for Phase III, and 24% for Phase IV. For medicines with Phase II results available (n=6), the average reduction in IOP was 23%, 24% for Phase III, and 23% for Phase IV. For medicines with Phase III results available (n=11), the average reduction in IOP was 25% and 24% for Phase IV.
Conclusion
This study indicates that early phase trials usually approximated the results of later regulatory studies and post-commercialization trials.
Similar content being viewed by others


Introduction
To gain regulatory approval for a new medicine, a pharmaceutical company must take the new product through a series of clinical trials (Phases I–III). A Phase I trial represents the first instance a new product is used in human subjects and is performed primarily to collect safety information. In a Phase II trial, a new product is used for the first time in patients with the target disease to gain dosing and concentration information. At least two Phase III trials are performed and they are expanded in size and duration. These trials typically provide the most information on the efficacy and safety of the new product on which regulatory approval is based. Phase IV studies are those that are performed after commercial release of the medicine.
A pharmaceutical company must make a decision at the end of each phase whether the efficacy and safety information warrants the resources, in money and personnel, to continue clinical development. Consequently, adequately performed early trials (I–II) should predict the results of Phase III and IV studies. However, the limited size and duration, as well as the subject selection, might restrict the early phase trial's ability to accurately predict future results. Unfortunately, little information is available regarding how well Phase I–III trials predict the ultimate commercial efficacy of a new product.
Methods
Using published literature on Pubmed (http://www.ncbi.nlm.nih.gov/entrez/query), we evaluated the Phase I–III trials for glaucoma medicines that became commercially available since 1977, and at least the first five Phase IV trials available. We used the generic and brand name of each included medicine as keywords along with the term ‘glaucoma’. We wished to determine the predictive value of early Phase trials (I–II) for the ocular hypotensive efficacy observed in Phases III and IV.
This study evaluated 12 medicines in 65 articles in the literature with at least two phases available (see Table 1).1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58, 59, 60, 61, 62, 63, 64, 65
Results
For medicines with Phase I results available (n=3), the average reduction in intraocular pressure from untreated baseline was 16%, 26% for Phase II, 26% for Phase III, and 24% for Phase IV. For medicines with Phase II results available (n=6), the average reduction in intraocular pressure was 23%, 24% for Phase III, and 23% for Phase IV. For medicines with Phase III results available (n=11), the average reduction in intraocular pressure was 25%, and it was 24% for Phase IV. For medicines with the earliest results available in Phase I, II, or III, all products were within 10, 12, and 6%, respectively, of Phase IV study efficacy.
Discussion
The results of this review indicate that early phase trials usually approximated the results of later regulatory studies and post-commercialization trials. However, caution is warranted because results still deviated between phases by clinically important amounts in several studies. This was especially apparent with timolol, which demonstrated reduced efficacy over a large number of Phase IV trials compared to earlier phase studies. The reason for this decrease was not apparent by our results.
Nonetheless, the results of this review should give a pharmaceutical company, and the associated investigators, some confidence that a glaucoma medicine effective in early regulatory trials will probably have similar efficacy in the subsequent phases and after commercialization.
However, the results of this study are limited in that it reviewed only products launched commercially. Data and the predictive values of their regulatory trials were not available for the products that failed development. More research is needed, in general, with clinical measures and the development process, to help investigators and pharmaceutical companies know how to most efficiently develop a new glaucoma product.
References
Nagasubramanian S, Hitchings RA, Demailly P, Chuniaud M, Pannarale MR, Pecori-Giraldi J et al. Comparision of apraclonidine and timolol in chronic open-angle glaucoma. A three-month study. Ophthalmology 1993; 100 (9): 1318–1323.
Abrams DA, Robin AL, Pollack IP, deFaller JM, DeSantis L . The safety and efficacy of topical 1% ALO 2145 (p-aminoclonidine hydrochloride) in normal volunteers. Arch Ophthalmol 1987; 105 (9): 1205–1207.
Strahlman E, Tipping R, Vogel R . A double-masked, randomized 1-year study comparing dorzolamide (Trusopt), timolol, and betaxolol. International Dorzolamide Study Group. Arch Ophthalmol 1995; 113 (8): 1009–1016.
Berry Jr DP, Van Buskirk EM, Shields MB . Betaxolol and timolol. A comparison of efficacy and side effects. Arch Ophthalmol 1984; 102 (1): 42–45.
Weinreb RN, Caldwell DR, Goode SM, Horwitz BL, Laibovitz R, Shrader CE et al. A double-masked three-month comparison between 0.25% betaxolol suspension and 0.5% betaxolol ophthalmic solution. Am J Ophthalmol 1990; 110 (2): 189–192.
Feghali JG, Kaufman PL . Decreased intraocular pressure in the hypertensive human eye with betaxolol, a beta 1-adrenergic antagonist. Am J Ophthalmol 1985; 100 (6): 777–782.
Caldwell DR, Salisbury CR, Guzek JP . Effects of topical betaxolol in ocular hypertensive patients. Arch Ophthalmol 1984; 102 (4): 539–540.
Feghali JG, Kaufman PL, Radius RL, Mandell AI . A comparison of betaxolol and timolol in open angle glaucoma and ocular hypertension. Acta Ophthalmol (Copenh) 1988; 66 (2): 180–186.
DuBiner H, Cooke D, Dirks M, Stewart WC, VanDenburgh AM, Felix C . Efficacy and safety of bimatoprost in patients with elevated intraocular pressure: a 30-day comparison with latanoprost. Surv Ophthalmol 2001; 45 (Suppl 4): S353–S360.
Sherwood M, Brandt J, Bimatoprost Study Groups 1 and 2. Six-month comparison of bimatoprost once-daily and twice-daily with timolol twice-daily in patients with elevated intraocular pressure. Surv Ophthalmol 2001; 45 (Suppl 4): S361–S368.
Cohen JS, Gross RL, Cheetham JK, VanDenburgh AM, Bernstein P, Whitcup SM . Two-year double-masked comparison of bimatoprost with timolol in patients with glaucoma or ocular hypertension. Surv Ophthalmol 2004; 49 (Suppl 1): S45–S52.
Walters TR, DuBiner HB, Carpenter SP, Khan B, VanDenburgh AM, Bimatoprost Circadian IOP Study Group. 24-H IOP control with once-daily bimatoprost, timolol gel-forming solution, or latanoprost: a 1-month, randomized, comparative clinical trial. Surv Ophthalmol 2004; 49 (Suppl 1): S26–S35.
Laibovitz RA, VanDenburgh AM, Felix C, David R, Batoosingh A, Rosenthal A et al. Comparison of the ocular hypotensive lipid AGN 192024 with timolol: dosing, efficacy, and safety evaluation of a novel compound for glaucoma management. Arch Ophthalmol 2001; 119 (7): 994–1000.
Brubaker RF, Schoff EO, Nau CB, Carpenter SP, Chen K, Vandenburgh AM . Effects of AGN 192024, a new ocular hypotensive agent, on aqueous dynamics. Am J Ophthalmol 2001; 131 (1): 19–24.
Stewart WC, Stewart JA, Day D, Sharpe ED . Efficacy and safety of timolol maleate/latanoprost fixed combination versus timolol maleate and brimonidine given twice daily. Acta Ophthalmol Scand 2003; 81 (3): 242–246.
Liu CJ, Ko YC, Cheng CY, Chiu AW, Chou JC, Hsu WM et al. Changes in intraocular pressure and ocular perfusion pressure after latanoprost 0.005% or brimonidine tartrate 0.2% in normal-tension glaucoma patients. Ophthalmology 2002; 109 (12): 2241–2247.
Kampik A, Arias-Puente A, O’Brart DP, Vuori ML, European Latanoprost Study Group. Intraocular pressure-lowering effects of latanoprost and brimonidine therapy in patients with open-angle glaucoma or ocular hypertension: a randomized observer-masked multicenter study. J Glaucoma 2002; 11 (2): 90–96.
Konstas AG, Stewart WC, Topouzis F, Tersis I, Holmes KT, Stangos NT . Brimonidine 0.2% given two or three times daily versus timolol maleate 0.5% in primary open-angle glaucoma. Am J Ophthalmol 2001; 131 (6): 729–733.
Schuman JS . Clinical experience with brimonidine 0.2% and timolol 0.5% in glaucoma and ocular hypertension. Surv Ophthalmol 1996; 41 (Suppl 1): S27–S37.
LeBlanc RP . Twelve-month results of an ongoing randomized trial comparing brimonidine tartrate 0.2% and timolol 0.5% given twice daily in patients with glaucoma or ocular hypertension. Brimonidine Study Group 2. Ophthalmology 1998; 105 (10): 1960–1967.
Katz LJ . Brimonidine tartrate 0.2% twice daily vs timolol 0.5% twice daily: 1-year results in glaucoma patients. Brimonidine Study Group. Am J Ophthalmol 1999; 127 (1): 20–26.
Schuman JS, Horwitz B, Choplin NT, David R, Albracht D, Chen K . A 1-year study of brimonidine twice daily in glaucoma and ocular hypertension. A controlled, randomized, multicenter clinical trial. Chronic Brimonidine Study Group. Arch Ophthalmol 1997; 115 (7): 847–852.
Derick RJ, Robin AL, Walters TR, Barnebey HS, Choplin N, Schuman J et al. Brimonidine tartrate: a one-month dose response study. Ophthalmology 1997; 104 (1): 131–136.
Shin DH, Feldman RM, Sheu WP, Fixed Combination Latanoprost/Timolol Study Group. Efficacy and safety of the fixed combinations latanoprost/timolol versus dorzolamide/timolol in patients with elevated intraocular pressure. Ophthalmology 2004; 111 (2): 276–282.
Konstas AG, Papapanos P, Tersis I, Houliara D, Stewart WC . Twenty-four-hour diurnal curve comparison of commercially available latanoprost 0.005% versus the timolol and dorzolamide fixed combination. Ophthalmology 2003; 110 (7): 1357–1360.
Konstas AG, Papapanos P, Tersis I, Houliara D, Stewart WC . Twenty-four-hour diurnal curve comparison of commercially available latanoprost 0.005% versus the timolol and dorzolamide fixed combination. Ophthalmology 2003; 110 (7): 1357–1360.
Strohmaier K, Snyder E, DuBiner H, Adamsons I . The efficacy and safety of the dorzolamide–timolol combination versus the concomitant administration of its components. Dorzolamide–Timolol Study Group. Ophthalmology 1998; 105 (10): 1936–1944.
Clineschmidt CM, Williams RD, Snyder E, Adamsons IA . A randomized trial in patients inadequately controlled with timolol alone comparing the dorzolamide-timolol combination to monotherapy with timolol or dorzolamide. Dorzolamide–Timolol Combination Study Group. Ophthalmology 1998; 105 (10): 1952–1959.
O’Donoghue EP . A comparison of latanoprost and dorzolamide in patients with glaucoma and ocular hypertension: a 3 month, randomised study. Ireland Latanoprost Study Group. Br J Ophthalmol 2000; 84 (6): 579–582.
Lippa EA, Carlson LE, Ehinger B, Eriksson LO, Finnstrom K, Holmin C et al. Dose response and duration of action of dorzolamide, a topical carbonic anhydrase inhibitor. Arch Ophthalmol 1992; 110 (4): 495–499.
Heijl A, Strahlman E, Sverrisson T, Brinchman-Hansen O, Puustjarvi T, Tipping R . A comparison of dorzolamide and timolol in patients with pseudoexfoliation and glaucoma or ocular hypertension. Ophthalmology 1997; 104 (1): 137–142.
Kitazawa Y, Azuma I, Iwata K, Tsukahara S, Shiose Y, Araie M et al. Dorzolamide, a topical carbonic anhydrase inhibitor: a two-week dose-response study in patients with glaucoma or ocular hypertension. J Glaucoma 1994; 3: 275–279.
Higginbotham EJ, Feldman R, Stiles M, Dubiner H, Fixed Combination Investigative Group. Latanoprost and timolol combination therapy vs monotherapy: one-year randomized trial. Arch Ophthalmol 2002; 120 (7): 915–922.
Larsson LI . Effect on intraocular pressure during 24 h after repeated administration of the fixed combination of latanoprost 0.005% and timolol 0.5% in patients with ocular hypertension. J Glaucoma 2001; 10 (2): 109–114.
Watson P, Stjernschantz J . A six-month, randomized, double-masked study comparing latanoprost with timolol in open-angle glaucoma and ocular hypertension. The Latanoprost Study Group. Ophthalmology 1996; 103 (1): 126–137.
Camras CB . Comparison of latanoprost and timolol in patients with ocular hypertension and glaucoma: a six-month masked, multicenter trial in the United States. The United States Latanoprost Study Group. Ophthalmology 1996; 103 (1): 138–147.
Hedman K, Larsson LI . The effect of latanoprost compared with timolol in African-American, Asian, Caucasian, and Mexican open-angle glaucoma or ocular hypertensive patients. Surv Ophthalmol 2002; 47 (Suppl 1): S77–S89.
Sponsel WE, Mensah J, Kiel JW, Remky A, Trigo Y, Baca W et al. Effects of latanoprost and timolol-XE on hydrodynamics in the normal eye. Am J Ophthalmol 2000; 130 (2): 151–159.
Sponsel WE, Paris G, Trigo Y, Pena M . Comparative effects of latanoprost (Xalatan) and unoprostone (Rescula) in patients with open-angle glaucoma and suspected glaucoma. Am J Ophthalmol 2002; 134 (4): 552–559.
Tsukamoto H, Mishima HK, Kitazawa Y, Araie M, Abe H, Negi A, Glaucoma Study Group. A comparative clinical study of latanoprost and isopropyl unoprostone in Japanese patients with primary open-angle glaucoma and ocular hypertension. J Glaucoma 2002; 11 (6): 497–501.
Kobayashi H, Kobayashi K, Okinami S . A comparison of intraocular pressure-lowering effect of prostaglandin F2 -alpha analogues, latanoprost, and unoprostone isopropyl. J Glaucoma 2001; 10 (6): 487–492.
Aung T, Chew PT, Yip CC, Chan YH, See JL, Khng CG et al. A randomized double-masked crossover study comparing latanoprost 0.005% with unoprostone 0.12% in patients with primary open-angle glaucoma and ocular hypertension. Am J Ophthalmol 2001; 131 (5): 636–642.
Saito M, Takano R, Shirato S . Effects of latanoprost and unoprostone when used alone or in combination for open-angle glaucoma. Am J Ophthalmol 2001; 132 (4): 485–489.
Netland PA, Landry T, Sullivan EK, Andrew R, Silver L, Weiner A et al. Travoprost compared with latanoprost and timolol in patients with open-angle glaucoma or ocular hypertension. Am J Ophthalmol 2001; 132 (4): 472–484.
Nagasubramanian S, Sheth GP, Hitchings RA, Stjernschantz J . Intraocular pressure-reducing effect of PhXA41 in ocular hypertension. Comparison of dose regimens. Ophthalmology 1993; 100 (9): 1305–1311.
Alm A, Villumsen J . PhXA34, a new potent ocular hypotensive drug. A study on dose-response relationship and on aqueous humor dynamics in healthy volunteers. Arch Ophthalmol 1991; 109 (11): 1564–1568.
Villumsen J, Alm A . PhXA34−a prostaglandin F2 alpha analogue. Effect on intraocular pressure in patients with ocular hypertension. Br J Ophthalmol 1992; 76 (4): 214–217.
Alm A, Villumsen J, Tornquist P, Mandahl A, Airaksinen J, Tuulonen A et al. Intraocular pressure-reducing effect of PhXA41 in patients with increased eye pressure. A one-month study. Ophthalmology 1993; 100 (9): 1312–1316 discussion 1316–1317.
Alm A, Stjernschantz J . Effects on intraocular pressure and side effects of 0.005% latanoprost applied once daily, evening or morning. A comparison with timolol. Scandinavian Latanoprost Study Group. Ophthalmology 1995; 102 (12): 1743–1752.
Racz P, Ruzsonyi MR, Nagy ZT, Bito LZ . Maintained intraocular pressure reduction with once-a-day application of a new prostaglandin F2 alpha analogue (PhXA41). An in-hospital, placebo-controlled study. Arch Ophthalmol 1993; 111 (5): 657–661.
Larsson LI, Mishima HK, Takamatsu M, Orzalesi N, Rossetti L . The effect of latanoprost on circadian intraocular pressure. Surv Ophthalmol 2002; 47 (Suppl 1): S90–S96.
Camras CB, Wax MB, Ritch R, Weinreb R, Robin AL, Higginbotham EJ et al. Latanoprost treatment for glaucoma: effects of treating for 1 year and of switching from timolol. United States Latanoprost Study Group. Am J Ophthalmol 1998; 126 (3): 390–399.
Watson PG . Latanoprost. Two years’ experience of its use in the United Kingdom. Latanoprost Study Group. Ophthalmology 1998; 105 (1): 82–87.
Rulo AH, Greve EL, Geijssen HC, Hoyng PF . Reduction of intraocular pressure with treatment of latanoprost once daily in patients with normal-pressure glaucoma. Ophthalmology 1996; 103 (8): 1276–1282.
Mishima HK, Masuda K, Kitazawa Y, Azuma I, Araie M . A comparison of latanoprost and timolol in primary open-angle glaucoma and ocular hypertension. A 12-week study. Arch Ophthalmol 1996; 114 (8): 929–932.
Stewart WC, Leland TM, Cate EA, Stewart JA . Efficacy and safety of timolol solution once daily versus timolol gel in treating elevated intraocular pressure. J Glaucoma 1998; 7 (6): 402–407.
Schenker HI, Silver LH . Long-term intraocular pressure-lowering efficacy and safety of timolol maleate gel-forming solution 0.5% compared with Timoptic XE 0.5% in a 12-month study. Am J Ophthalmol 2000; 130 (2): 145–150.
Stewart RH, Kimbrough RL, Ward RL . Betaxolol vs timolol. A six-month double-blind comparison. Arch Ophthalmol 1986; 104 (1): 46–48.
Zimmerman TJ, Kass MA, Yablonski ME, Becker B . Timolol maleate: efficacy and safety. Arch Ophthalmol 1979; 97 (4): 656–658.
Zimmerman TJ, Kaufman HE . Timolol. A beta-adrenergic blocking agent for the treatment of glaucoma. Arch Ophthalmol 1977; 95 (4): 601–604.
Katz IM, Hubbard WA, Getson AJ, Gould AL . Intraocular pressure decrease in normal volunteers following timolol ophthalmic solution. Invest Ophthalmol 1976; 15 (6): 489–492.
LeBlanc RP, Saheb NE, Krip G . Timolol: long-term Canadian multicentre study. Can J Ophthalmol 1985; 20 (4): 128–130.
Stewart WC, Stewart JA, Holmes KT, Leech JN . Differences in ocular surface irritation between timolol hemihydrate and timolol maleate. Am J Ophthalmol 2000; 130 (6): 712–716.
Sakurai M, Araie M, Oshika T, Mori M, Masuda K, Ueno R et al. Effects of topical application of UF-021, a novel prostaglandin derivative, on aqueous humor dynamics in normal human eyes. Jpn J Ophthalmol 1991; 35 (2): 156–165 erratum in Jpn J Ophthalmol 1992;36(4):491.
Azuma I, Masuda K, Kitazawa Y, Takase M, Yamamura H . Double-masked comparative study of UF-021 and timolol ophthalmic solutions in patients with primary open-angle glaucoma or ocular hypertension. Jpn J Ophthalmol 1993; 37 (4): 514–525.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Stewart, W., Jenkins, J. Predictive value of the efficacy of glaucoma medications in regulatory trials: Phase I–III to post-marketing studies. Eye 22, 985–988 (2008). https://doi.org/10.1038/sj.eye.6702913
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702913
