
Abstract
Aims
To evaluate the relation between higher-order aberration of the eye and contrast sensitivity function in eyes with keratoconus.
Methods
In 22 eyes of 14 patients with keratoconus (age 30.5±8.4 years, means±SD) and 26 eyes of 13 normal controls (age 29.2±6.7 years), ocular higher-order wavefront aberration for a 6-mm pupil was measured with the Hartmann-Schack aberrometer (KR-9000 PW, Topcon). The root mean square (RMS) of third- and fourth-order Zernike coefficients was used to represent higher-order aberrations. The letter-contrast sensitivity was examined using the CSV-1000LV contrast chart (Vector Vision).
Results
In the keratoconus group, the letter-contrast sensitivity showed significant correlation with third-order (Spearman's correlation coefficient r=−0.736, P<0.001) and fourth-order aberrations (r=−0.464, P<0.05). There was borderline correlation between log MAR BSCVA and third-order (r=0.413, P=0.070) and fourth-order aberrations (r=0.394, P=0.086). In the normal group, the letter-contrast sensitivity had no significant correlation with third-order (r=−0.170, P=0.411) and fourth-order aberrations (r=−0.088, P=0.673), and log MAR best spectacle-corrected visual acuity (BSCVA) showed no correlation with third-order (r=0.063, P=0.762) and fourth-order aberrations (r=−0.282, P=0.165).
Conclusions
In eyes with keratoconus, there is significant correlation between contrast sensitivity and ocular higher-order wavefront aberrations.
Similar content being viewed by others
Introduction
Keratoconus is a chronic, non-inflammatory disease of the cornea associated with progressive thinning and anterior protrusion of the central cornea.1, 2 Irregular astigmatism is often the first and most apparent clinical finding in keratoconus, and this is evidenced by a distortion of the corneal image as noted with the placido disc, retinoscope, keratometer, keratoscope, and computerized videokeratograph. Previous studies using videokeratography have quantitatively demonstrated that corneal irregular astigmatism is significantly greater in eyes with keratoconus than in normal eyes.3, 4, 5, 6 In addition, recent studies using wavefront analysis technology showed that ocular and corneal higher-order aberration, particularly coma aberration, is significantly increased in keratoconus.7, 8, 9, 10 Maeda et al11 reported that corneal topographic indices significantly correlated with letter-contrast sensitivity in eyes with keratoconus. Applegate et al7 reported significant correlation between corneal aberration and contrast sensitivity in 91 eyes with a variety of corneal conditions, including 8 eyes with keratoconus, but such correlation in eyes with keratoconus was not assessed. To the best of our knowledge, the influence of ocular higher-order aberration on contrast sensitivity function in eyes with keratoconus has not been investigated. We conducted the current study to investigate the relationship between ocular wavefront aberration and letter-contrast sensitivity in keratoconus.
Methods
We examined 22 eyes of 14 patients with keratoconus. There were seven men and seven women, and their age averaged 30.5±8.4 years old. They were diagnosed with slit lamp biomicroscopy and corneal videokeratography. Eyes with corneal scarring or cataract were excluded from the subjects. The best spectacle-corrected visual acuity (BSCVA) ranged from 25/20 to 20/40. Twenty-six eyes of 13 patients served as age-matched normal controls. There were eight men and five women, and their age averaged 29.2±6.7 years old. The BSCVA was 20/20 or better.
Ocular wavefront aberrations for 6-mm pupils were measured using a Hartmann–Shack wavefront analyser (KR-9000 PW, Topcon Corp., Tokyo, Japan) after the pupils were fully dilated with 1% tropicamide. Measurements were repeated three times for each subject, and the mean of the measurements was used for data analyses. All of the Hartmann images were revised to the pupil centre images.12, 13, 14 The obtained data were expanded into the set of orthogonal Zernike polynomials. The root mean square of third-order (Z3−3 to Z33) and fourth-order (Z4−4 to Z44) Zernike components were used to represent higher-order aberrations.15, 16, 17, 18, 19
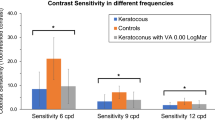
Letter-contrast sensitivity was measured with CSV-1000LV chart (Vector Vision, Columbus, OH, USA). This instrument uses letter optotypes all of which were the same size and of low spatial frequency (2.4 cycle/°).20 There were eight contrast levels (standard, 35.5, 17.8, 8.9, 6.3, 4.5, 2.2, and 1.1%), and each contrast level had three letters. The measurements were performed at 2.5 m distance under full spectacle correction. The mean luminance was 81 cd/m2. The test results were recorded, not as the contrast threshold or contrast sensitivity, but as the number of correctly identified letters out of 24 letters.11, 21
The study followed the tenets of the Declaration of Helsinki, and prestudy informed consent was obtained from all subjects after explanation of the nature and possible consequences of the study. The patients with keratoconus were instructed to refrain from wearing contact lenses for at least 2 weeks before the study examinations. A single experienced investigator performed all measurements.
Results
Measurement results are shown in the Table 1. The eyes with keratoconus showed significantly larger values than the normal controls in both third-order (P<0.0001, Wilcoxon rank-sum test) and fourth-order aberrations (P<0.0001). The log MAR BSCVA was significantly worse in eyes with keratoconus (0.037±0.169) than in the normal controls (−0.118±0.063) (P<0.001). The letter-contrast sensitivity was significantly lower in eyes with keratoconus (17.4±3.8 letters) than in the normal controls (21.8±1.4 letters) (P<0.0001). A total of 5 out of 26 eyes (19.2%) in the normal group could read all 24 letters, while no eye in the keratoconus group scored full marks.
The relation between visual function and higher-order aberration was evaluated. In the keratoconus group, there was borderline correlation between log MAR BSCVA and third-order (Spearman's correlation coefficient r=0.413, P=0.070; Figure 1) and fourth-order aberrations (r=0.394, P=0.086; Figure 2). The letter-contrast sensitivity showed significant correlation with third-order (r=−0.736, P<0.001; Figure 3) and fourth-order aberrations (r=−0.464, P<0.05; Figure 4).

There was borderline correlation between log MAR BSCVA and third-order aberration (Spearman's correlation coefficient r=0.413, P=0.07) in eyes with keratoconus.

There was borderline correlation between log MAR BSCVA and fourth-order aberration (Spearman's correlation coefficient r=0.394, P=0.086) in eyes with keratoconus.

Significant correlation was found between letter-contrast sensitivity and third-order aberration (Spearman's correlation coefficient r=−0.736, P<0.001) in eyes with keratoconus.

Significant correlation was found between letter-contrast sensitivity and fourth-order aberration (Spearman's correlation coefficient r=−0.464, P<0.05) in eyes with keratoconus.
In the normal group, there was no significant correlation between log MAR BSCVA and third-order (r=0.063, P=0.762) and fourth-order aberrations (r=−0.282, P=0.165). The letter-contrast sensitivity also showed no significant correlation with third-order (r=−0.170, P=0.411) and fourth-order aberrations (r=−0.088, P=0.673).
Discussion
Our study showed that ocular third- and fourth-order aberrations were significantly larger in eyes with keratoconus than in the normal controls. Previous studies also reported that coma and spherical aberrations significantly increased in eyes with keratoconus, with larger increases in coma aberration.7, 8, 9, 10 Maeda et al8 found that coma aberration was 2.32 times larger than spherical aberration in eyes with keratoconus, and Barbero et al9 reported that coma aberration was 3.74 times higher in eyes with keratoconus than in normal controls. In the current study, third-order coma aberration was 3.25 times larger than fourth-order spherical aberration in eyes with keratoconus, and third-order aberration was 6.29 times higher in eyes with keratoconus than in the normal controls.
We found that letter-contrast sensitivity was significantly deteriorated in eyes with keratoconus, and both third- and fourth-order aberrations showed significant correlation with letter-contrast sensitivity. In normal controls, letter-contrast sensitivity did not correlate with either third- or fourth-order aberrations. In the CLEK study, it has been reported that low-contrast acuity deteriorated more rapidly than high-contrast visual acuity in eyes with keratoconus.22 Pesudovs et al23 demonstrated that while visual acuity is an excellent test for comparing normal, keratoconus, and post-penetrating keratoplasty groups, additional useful information can be provided by low-contrast visual acuity and Pelli-Robson contrast sensitivity. Judging from these previous and current findings, it seems that contrast sensitivity testing is a highly sensitive measure to evaluate visual disturbance caused by increases in higher-order aberration of the eye.
In eyes with keratoconus, letter-contrast sensitivity had greater correlation with third-order coma aberration (r=−0.736) than with fourth-order spherical aberration (r=−0.464). This result seems to reflect the fact that coma aberration dominates over spherical aberration in eyes with keratoconus.8 In keratoconus, the apex is usually displaced from the centre of the cornea, resulting in asymmetry in corneal power distribution. The increases in topographic indices such as the inferior–superior24 and surface asymmetry index25 values represent the asymmetric power distribution in the cornea, which are in good agreement with the increase in coma aberration in keratoconus. The eyes with keratoconus often have their cones in the inferior part of the cornea, leading to relatively slower wavefront in the inferior part of the cornea and advanced wavefront in the superior area of the cornea.8
The current study has several weaknesses. First, only 22 eyes were tested in the keratoconus group. To exclude the influence of non-optical factors on the visual performance, eyes with corneal scarring or cataract were not included in the subjects. Moreover, many subjects did not agree to participate in the current study, which entails time-consuming examinations, such as contrast sensitivity measurements and wavefront analysis. Second, the CSV-1000LV chart with which letter-contrast sensitivity was measured has some imperfection. This instrument uses eight contrast levels, but each level does not have equal interval between them. When the per cent contrast threshold is converted to logarithm of contrast sensitivity, the steps will be 0.45, 0.75, 1.05, 1.20, 1.35, 1.65, and 1.95. Some steps are 0.30 log units apart, and others are 0.15 log units apart. A chart having linear step increments will be more favourable to evaluate the subtle changes in visual function.
The relationship between contrast sensitivity and ocular higher-order aberration has been studied in a variety of ocular diseases.7, 12, 16, 26, 27, 28 Eyes with cataract have decreased contrast sensitivity and increased higher-order aberration.12 Applegate et al16 reported that the area under the contrast sensitivity function decreases as the wavefront variances increase after radial keratotomy. A study using aberroscopy demonstrated that low-contrast visual acuity and glare visual acuity were adversely influenced by the increases in total ocular aberrations after photorefractive keratectomy.26 Yamane et al27 demonstrated that conventional laser in situ keratomileusis significantly increases ocular higher-order aberrations, which compromise the postoperative contrast sensitivity functions. The current study represents the first report of significant association between ocular higher-order aberration and contrast sensitivity in eyes with keratoconus. One of the clinical significances of our data is that an objective parameter (ocular higher-order aberration) correlated with subjective visual function, which has long been the only source of information to decide surgical intervention. Further refinements in the objective means to assess disease severity and progression would be of high clinical benefits in the practice of gradually progressive diseases, which deteriorates quality of vision.
References
Krachmer JH, Feder RS, Belin MW . Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol 1984; 28: 293–322.
Kennedy RH, Bourne WM, Dyer JA . A 48-year clinical and epidemiologic study of keratoconus. Am J Ophthalmol 1986; 101: 267–273.
Oshika T, Tomidokoro A, Maruo K, Tokunaga T, Miyata N . Quantitative evaluation of irregular astigmatism by Fourier series harmonic analysis of videokeratography data. Invest Ophthalmol Vis Sci 1998; 39: 705–709.
Tomidokoro A, Oshika T, Amano S, Higaki S, Maeda N, Miyata K . Changes in anterior and posterior corneal curvatures in keratoconus. Ophthalmology 2000; 107: 1328–1332.
Oshika T, Tanabe T, Tomidokoro A, Amano S . Progression of keratoconus assessed by Fourier analysis of videokeratography data. Ophthalmology 2002; 109: 339–342.
Tanabe T, Tomidokoro A, Samejima T, Miyata K, Sato M, Kaji Y et al. Corneal regular and irregular astigmatism assessed by Fourier analysis of videokeratography data in normal and pathologic eyes. Ophthalmology 2004; 111: 752–757.
Applegate RA, Hilmantel G, Howland HC, Tu EY, Starck T, Zayac EJ . Corneal first surface optical aberrations and visual performance. J Refract Surg 2000; 16: 507–514.
Maeda N, Fujikado T, Kuroda T, Mihashi T, Hirohara Y, Nishida K et al. Wavefront aberrations measured with Hartmann–Shack sensor in patients with keratoconus. Ophthalmology 2002; 109: 1996–2003.
Barbero S, Marcos S, Merayo-Lloves J, Moreno-Barriuso E . Validation of the estimation of corneal aberrations from videokeratography in keratoconus. J Refract Surg 2002; 18: 263–270.
Shah S, Naroo S, Hosking S, Gherghel D, Mantry S, Bannerjee S et al. Nidek OPD-scan analysis of normal, keratoconic, and penetrating keratoplasty eyes. J Refract Surg 2003; 19: S255–S259.
Maeda N, Sato S, Watanabe H, Inoue Y, Fujikado T, Shimomura Y et al. Prediction of letter contrast sensitivity using videokeratographic indices. Am J Ophthalmol 2000; 129: 759–763.
Kuroda T, Fujikado T, Maeda N, Oshika T, Hirohara Y, Mihashi T . Wavefront analysis in eyes with nuclear or cortical cataract. Am J Ophthalmol 2002; 134: 1–9.
Kuroda T, Fujikado T, Maeda N, Oshika T, Hirohara Y, Mihashi T . Wavefront analysis of higher-order aberrations in patients with cataract. J Cataract Refract Surg 2002; 28: 438–444.
Ninomiya S, Fujikado T, Kuroda T, Maeda N, Tano Y, Oshika T et al. Changes of ocular aberration with accommodation. Am J Ophthalmol 2002; 134: 924–926.
Howland HC, Howland B . A subjective method for the measurement of monochromatic aberrations of the eye. J Opt Soc Am 1977; 67: 1508–1518.
Applegate RA, Howland HC, Sharp RP, Cottingham AJ, Yee RW . Corneal aberrations and visual performance after radial keratotomy. J Refract Surg Jul-Aug 1998; 14: 397–407.
Martinez CE, Applegate RA, Klyce SD, McDonald MB, Medina JP, Howland HC . Effect of pupillary dilation on corneal optical aberrations after photorefractive keratectomy. Arch Ophthalmol 1998; 116: 1053–1062.
Oshika T, Klyce SD, Applegate RA, Howland HC, El Danasoury MA . Comparison of corneal wavefront aberrations after photorefractive keratectomy and laser in situ keratomileusis. Am J Ophthalmol 1999; 127: 1–7.
Oshika T, Klyce SD, Applegate RA, Howland HC . Changes in corneal wavefront aberrations with aging. Invest Ophthalmol Vis Sci 1999; 40: 1351–1355.
Pelli DG, Robson G, Wilkins AJ . The designed of a new letter chart for measuring contrast sensitivity. Clin Vis Sci 1988; 2: 187–199.
Elliott DB, Bullimore MA, Bailey IL . Improving the reliability of the Pelli-Robson contrast sensitivity test. Clin Vis Sci 1991; 6: 471–475.
Davis LJ, Schechtman KB, Wilson BS, Rosenstiel CE, Riley CH, Libassi DP et al. Collaborative Longitudinal Evaluation of Keratoconus (CLEK) Study Group. Longitudinal changes in visual acuity in keratoconus. Invest Ophthalmol Vis Sci 2006; 47: 489–500.
Pesudovs K, Schoneveld P, Seto RJ, Coster DJ . Contrast and glare testing in keratoconus and after penetrating keratoplasty. Br J Ophthalmol 2004; 88: 653–657.
Rabinowitz YS, McDonnell PJ . Computer-assisted corneal topography in keratoconus. Refract Corneal Surg 1989; 5: 400–408.
Maeda N, Klyce SD, Smolek MK, Thompson HW . Automated keratoconus screening with corneal topography analysis. Invest Ophthalmol Vis Sci 1994; 35: 2749–2757.
Seiler T, Kaemmerer M, Mierdel P, Krinke HE . Ocular optical aberrations after photorefractive keratectomy for myopia and myopic astigmatism. Arch Ophthalmol 2000; 118: 17–21.
Yamane N, Miyata K, Samejima T, Hiraoka T, Kiuchi T, Okamoto F et al. Ocular higher-order aberrations and contrast sensitivity after conventional laser in situ keratomileusis. Invest Ophthalmol Vis Sci 2004; 45: 3986–3990.
Tanabe T, Miyata K, Samejima T, Hirohara Y, Mihashi T, Oshika T . Influence of wavefront aberration and corneal subepithelial haze on low-contrast visual acuity after photorefractive keratectomy. Am J Ophthalmol 2004; 138: 620–624.
Acknowledgements
This work is supported in part by grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology, Japan.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Okamoto, C., Okamoto, F., Samejima, T. et al. Higher-order wavefront aberration and letter-contrast sensitivity in keratoconus. Eye 22, 1488–1492 (2008). https://doi.org/10.1038/sj.eye.6702902
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702902
Keywords
This article is cited by
-
A novel tool for quantitative measurement of distortion in keratoconus
Eye (2023)
-
The Characteristics of Quick Contrast Sensitivity Function in Keratoconus and Its Correlation with Corneal Topography
Ophthalmology and Therapy (2023)
-
Contrast sensitivity and higher-order aberrations in Keratoconus subjects
Scientific Reports (2021)
-
Comparison of visual quality after Femto-LASIK and TransPRK in patients with low and moderate myopia
International Ophthalmology (2020)
-
Die Wellenfrontanalyse in der ophthalmologischen Diagnostik
Der Ophthalmologe (2008)
