
Abstract
Aim
To investigate factors affecting refractive outcome following LASIK for myopia.
Method
Six hundred and seventy-four consecutive uncomplicated myopic LASIK surgeries, performed by a single surgeon, either using the Technolas 217 planoscan (n=372) or the NIDEK EC 5000 (n=302), were evaluated. Stratified random sampling was used to match the groups for refractive error, patient age, and gender. The final analysis included 302 patients from each treatment group. Conditions were identical for both surgeries, and pre-operative refractive errors were between −1.00 and −14.00 DS and <−1.50 DC. Refractive success was defined as −0.50 to +0.50 DS of the targeted refraction measured 3 months after surgery. A stepwise logistical regression analysis was used to determine variables associated with refractive failure.
Results
A successful refractive outcome was achieved in 78% (235/302) of surgeries using the Technolas laser and in 88% (266/302) using the NIDEK laser. Predictor variables for not achieving refractive success were pre-operative refractive error of above −5.00 DS, age more than 40 years, and surgery performed with the Technolas laser.
Conclusion
Both the Technolas 217 and the NIDEK EC-5000 excimer lasers achieve a successful refractive outcome in the majority of cases. However, patient and surgical factors can influence refractive outcome.
Similar content being viewed by others

Introduction
LASIK for myopia appears to result in good refractive outcomes with individual excimer laser types;1, 2, 3, 4, 5 however, comparative studies for different excimer lasers have not been reported. This paper aims to compare refractive results obtained using the Technolas 217 Planoscan (Bausch & Lomb Surgical, CA, USA) and the NIDEK EC-5000 (NIDEK Co., Gamagori, Japan) excimer lasers for uncomplicated myopic refractive corrections.
The Technolas 217 Planoscan flying spot 193 nm excimer laser uses up to a 7.0 mm optic zone size, usually 6.0 mm or smaller, with a transition zone size of greater than 8.5 mm.6 The NIDEK EC-5000 instrument is a scanning 193 nm excimer laser, which generally uses a 6.5 mm or smaller optic. The transition zone size can be varied and is usually 1 mm larger than the optic zone size; however, it can be expanded to 9.0 mm with extended zone calibration for myopic corrections if required.7
The NIDEK EC-5000 laser's normal transition diameter is 1.0–1.5 mm larger than the optic zone size, while the Technolas 217 has a larger transition curve that will produce a deeper ablation. The smaller transition zone size usually makes the NIDEK EC-5000 ablations thinner than that of the Technolas 217 for the same optic zone size. Larger ablations with the NIDEK EC-5000 are more likely to result in a greater initial post-operative hypermetropic residual refractive error.8, 9 Conversely, the Technolas 217 Plano scan results in undercorrection, which has since been compensated for in the surgical nomogram.10
Clearly, refractive success following myopic LASIK is modified by multiple factors such as patient characteristics including age and initial refractive error,11, 12, 13 plus changes to corneal stress forces after ablation14, 15 and the wound healing process.16 Multivariable analysis of patient and surgical variables may also demonstrate the contribution of laser type to refractive outcome.
Aim
The aim of the study was to compare refractive outcomes of LASIK surgeries carried out by a single surgeon using the Technolas 217 and the NIDEK EC-5000 excimer lasers in near-identical surgical environments. A successful refractive outcome this study was defined as a manifest refraction measured 3 months after surgery of between −0.50 and +0.50 DS (best sphere) of the targeted refractive result.
Materials and methods
Patients
Six hundred and seventy-four consecutive patients were recruited. LASIK surgery was performed using either the Technolas 217 (n=372) or the NIDEK EC-5000 excimer laser (n=302). Inclusion criteria for patients were as follows:
-
1
A stable pre-operative refractive error for at least 2 years before the LASIK procedure
-
2
Age more than 20 years
-
3
A pre-operative refractive error between −1.00 and −14.00 D sphere and astigmatism less than 1.50 D
-
4
A stable corneal curvature measured over a 3-month period before surgery in prior contact lens wearers
-
5
A normal tear film, defined as greater than 5 mm wetting in 5 min using the Schirmer test (Clement Clarke International Ltd, London, England)
-
6
No corneal irregularities
-
7
No systemic disease.
Informed consent was obtained from all patients, and the investigation was conducted in accordance with the tenets of the Declaration of Helsinki, as revised in 2000, and the study was approved by the University of New South Wales Human Research Ethics Panel.
Surgical procedure
One surgeon performed all the LASIK operations in two near identical surgical environments at two locations. One location used a NIDEK EC-5000 excimer laser and the second a Technolas 217 excimer laser. Patients self-presented at either location and consecutive eligible patients were enrolled over 8 months.
Consistent protocols were followed in all LASIK procedures carried out at both locations. The mean temperature and the humidity of each surgery (Radio Shack 63-1013 thermometer/hygrometer, Inter Tan Australia Ltd, Australia) were the same (Table 1). A 20-s delay between flap lift and ablation was maintained for all procedures to minimize stromal dehydration.17
The optic zone size used was based on leaving at least 250 μm of tissue in the stromal bed and having an optic size larger than the pupil size measured in mesopic light, to eliminate unwanted optical side effects, such as glare. The transition zone size for the NIDEK EC-5000 was 1 mm larger than the optic zone size and was directed by the program. For the Technolas 217, the transition zone measured approximately 9 mm. The Hansatome keratome (Bausch and Lomb surgical, CA, USA) with the 160 and 180 μm plates was available to cut the corneal flaps. With thin corneas, the 130 μm Automated Corneal Shaper (ACS) (Bausch and Lomb Surgical, CA, USA) was used.
The nomogram applied for correcting the spherical and astigmatic component of the refractive error had been modified for the NIDEK from Arturo Chayets' coupling nomogram. The Technolas nomogram was based upon the manufacturer's recommendations. Both nomograms had been modified for each laser based on the analysis of over 1000 previous LASIK surgeries carried out by this surgeon.
Data collection
Refractive outcomes were measured 3 months after the initial surgery to avoid the possible confounding effects of enhancement surgery.
Patient factors assessed included pre-operative manifest refractive error, age, gender, race, intraocular pressure (Perkins hand-held tonometer, Clement Clarke, London, UK), pre- and post-operative corneal curvature (EH2 90 corneal topographer, Alcon, Fort Worth, TX, USA), and pre- and post-operative corneal thickness (SP2000 ultrasound pachometer, Tomey Corporation, Nagoya, Japan). Procedural/surgical variables included the keratome plate thickness, keratome type, laser type, ablation depth (based on the laser algorithm), and optic zone size.
Refractive outcomes that were more than −0.50 or +0.50 DS best sphere from the targeted refraction after 3 months were regarded as a deviation from the expected result. In an attempt to eliminate accommodation, the criterion for the refraction end point was to achieve the best visual acuity with the greatest hypermetropic correction.
Manifest (ie non-cycloplegic) refractions were measured under near-identical photopic conditions at both centres.
Data analyses
Stratified random sampling was used to match the two treatment groups for refractive error, age, and gender, resulting in 302 patients being selected from the Technolas treatment group. Patient demographics for the two groups are shown in Table 1 and differences between the group demographics were evaluated with a grouped t-test, binomial test, or non-parametric comparison, where appropriate. Refractive error, patient age, gender, race, intraocular pressure, post-operative corneal curvature, post-operative corneal thickness, and keratome type were not significantly different between the two treatment groups. There were significant differences between groups in pre-operative corneal thickness, pre-operative corneal curvature, optic zone size, and keratome plate thickness. However, absolute differences were not deemed clinically significant and minor inequalities between groups were adjusted for within the analysis.
The entire data set was analysed using a multivariate logistic regression analysis. Logistic regression does not require homogeneity of variance, making it an appropriate and powerful analysis for this type of data (http://www2.chass.ncsu.edu/garson/pa765/logistic.htm) and is normally recommended as the method of choice when the independent variables do not satisfy the multivariate normal assumption.18 A logistic regression was selected as the method of choice as the outcome was a binary variable (success/deviation from target or failure), and fewer assumptions were required than that for other methods such as multiple regression analysis. Variables were selected for inclusion in the model in a sequential manner using a forward stepwise method. The goodness of fit of the final model was assessed by the Hosmer-Lemeshow test using SPSS 10 (SPSS Inc., Chicago, IL, USA) using the classification table, which shows the proportion of correct classification. To determine the generalization of the classification accuracy of the failures across samples, the model was fitted to 80% of the whole sample (the analysis sample) and that model was then applied to the remaining 20% (cross-validation sample). The STATA (STATA 7, Stata Corporation, TX, USA) program was also used to estimate the sensitivity and specificity of the analysis and to estimate the area under the receiver operating characteristic (ROC) curve.19
Results
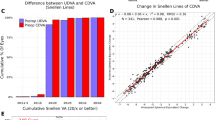
A successful refractive outcome was achieved in 78% (235/302) of surgeries using the Technolas laser and in 88% (266/302) of surgeries using the NIDEK laser. Figure 1 shows the distribution of refractive outcomes for each of the lasers. Of those showing a deviation from the target, 70% (47/67) of the Technolas cases had myopic residual refractive errors, whereas 81% (29/36) of cases with the NIDEK laser had hypermetropic residual errors. Patient and surgical characteristics for those patients (n=103) who did not achieve refractive success are shown in Table 2. No subject in either treatment group lost two lines or more of best-corrected visual acuity.

Refractive outcome distribution for NIDEK and Technolas lasers.
Multivariate model
The variables included in the final model were patient age, laser type, pre-operative refractive error, and keratome plate thickness. Table 3 shows variables associated with a failed refractive outcome, their respective odds ratios, and weighting within the model. The area under the ROC curve was estimated at 0.71. An area between 0.7 and 0.8 was considered to be an acceptable discrimination within the model.19 The Hosmer and Lemeshow's Goodness of Fit Test was not significant (χ2=5.31, P=0.622) implying that the model's estimates fitted the data.
When controlling for all other variables, patients above 50 years old had a 2.7 × (95% CI 1.3–6.4) greater risk of a poor refractive outcome when compared to those below 40 years (referent group). Patients between 40 and 49 years of age were also 2.6 × (95% CI 1.5–4.4) more likely to fail when compared to the referent group. The NIDEK laser was associated with a 0.48-fold lower risk of failure (95% CI 0.3–0.8) compared to that of the Technolas laser. Refractive errors of less than –5.00 DS had 0.41 × (95% CI 0.2–0.7) lower risk of failure when compared to the pre-operative refractive errors higher than −5.00 DS.
Variables not significantly associated with a failed outcome were patient's gender, pre-operative central corneal thickness, pre-operative intraocular pressure, pre-operative corneal curvature, keratome plate thickness, keratome type, and optic zone size.
Discussion
This study demonstrates that refractive success, defined as a residual refractive error of between −0.50 and +0.50 DS measured 3 months after LASIK surgery, can be achieved in up to 88% of LASIK procedures for myopia. However, deviation from target outcome with the Technolas 217 excimer laser tended to residual myopia and with the NIDEK EC-5000 to residual hypermetropia, which is consistent with previous reports.8, 10 Factors associated with non-targeted refractive outcomes included larger refractive errors, increased patient age, and Technolas procedure. Similar risk factors have been identified previously.10, 11
Refractive success in this study is slightly lower than that reported by Montes et al,20 which would be expected given the inclusion of higher pre-operative refractive errors in this study. The 88% success rate reported here is consistent with published reports in the same pre-operative range.11, 21, 22, 23, 24
The multivariable analysis demonstrated a significant trend to increased refractive failure with increasing patient age. This finding is consistent with previous clinical studies,11, 12, 13 and would suggest that stromal changes with age modulate post-operative healing and should be further investigated to improve the predictability of the procedure.
The higher risk of deviation from targeted refractive outcome with the Technolas laser compared to that of the NIDEK has not been previously reported. This is clearly not related to poor nomogram adjustment, but may be related to how the different lasers deliver energy to the tissue. The cornea rapidly thins during laser surgery because of dehydration and changes induced by biomechanical stress.17, 25 It is conceivable that smaller areas of ablation may suffer from greater change during the procedure, and ablating a larger area per pulse, as with the NIDEK, may limit unwanted tissue change. Increasing the laser scanning frequency and refocussing the laser may have a similar effect; however, increasing the laser frequency may cause heating of the tissue. Larger areas ablated per pulse can, however, cause islands of tissue,26 and small flying spot ablations are attractive to avoid irregular ablations. If the rate of changes to tissue induced by dehydration or biomechanical alterations can be incorporated into the laser algorithm, this may allow this hypothesis to be tested.
Clinical observations indicate that the NIDEK ablates distinct rings as the aperture opens to the programmed zone sizes, while the flying spot Technolas laser ablates a noticeably smoother ablation.27 This observation might suggest that the Technolas has the potential to achieve a more accurate change in corneal curvature than the NIDEK. However, factors other than smoothness of the ablation curve influence refractive outcome following laser ablation.
High myopic refractive corrections are associated with poorer refractive outcomes.8, 21, 28, 29, 30, 31, 32, 33 This study has confirmed in a multivariable analysis that low myopic corrections (<−5.00 DS) are 2.5 × more likely to achieve a result close to the target compared to corrections higher than −5.00 DS. Deeper ablations are associated with longer stromal exposure and this may result in increased water loss from the tissue.17 As water content varies, the laser ablation rate per scan also varies.34, 35 Stromal water content varies with depth. The anterior stroma has a lower water content than the posterior stroma,36, 37 such that deeper ablations may encounter variable tissue hydration. Individual variations in stromal water content may also exist resulting in possible inconsistencies in stromal ablation. Physically drying the stroma during the procedure causes an unstable refractive outcome or refractive regression.38 It is conceivable that the more change the stroma undergoes during the procedure, the greater the opportunity for unpredictable ablation and achieving the desired refractive outcome.
Previous studies have identified additional factors influencing refractive outcome, which were not significantly associated with deviation from targeted outcome, including pre-operative corneal curvature.9, 39 Extreme pre-operative corneal curvatures did not present in the current study and perhaps would not have been expected to influence outcome. Additionally, previous studies have frequently examined factors in isolation and have examined correlations between each single factor and the refractive outcome, rather than considering a multivariable analysis.
A potential limitation of this study was that patients self-selected at the two locations and could not be randomized. However, we believe that stratified random sampling to match subjects between groups was an appropriate strategy to overcome this limitation. The use of logistic multivariate analysis controls for some difference between groups within the analysis. The greatest limitation in this statistical approach occurs where there are outliers in the data or if the study sample is low. In the current study, however, the distribution of the two treatment groups was almost identical (Table 1) and outliers were not apparent. Unlike multivariate regression analysis, logistic regression does not require linear relationships between the independent and the dependent variables and is highly suited to data in this form.
Poor refractive outcomes following LASIK may be attributed to multiple factors not evaluated in this study. The consistency of the delivery of laser energy to the cornea may vary with different lasers under different conditions. Individual variations in corneal birefringence may cause unpredictable filtering of the polarized laser energy.40 Post-operative corneal shape may be affected by unpredictable release of biomechanical stress, stromal dehydration, an abnormal wound healing response, or stromal inhomogeneity. Identification of these factors is not possible in a clinical setting; however, further in vitro study would help to understand their influence on refractive outcomes following LASIK surgery.
In summary, refractive success is achieved in a high proportion of patients following LASIK surgery for myopia. For a single surgeon in two near identical surgical environments, refractive outcome is influenced by patient age, size of refractive error, and laser type.
References
Gimbal HV, Basti S, Kaye GB, Ferensowicz M . Experience during the learning curve of laser in situ keratomileusis. J Cataract Refract Surg 1996; 22: 542–550.
Pallikaris IG, Siganos DS . Laser in situ keratomileusis to treat myopia: early experience. J Cataract Refract Surg 1997; 23: 39–49.
Gris O, Guell JL, Muller A . Keratomileusis update. J Cataract Refract Surg 1996; 22: 620–623.
Pallikaris IG, Siganos DS . Excimer laser in situ keratomileusis and photorefractive keratectomy for correction of high myopia. J Refract Corneal Surg 1994; 10: 498–510.
Rashad KM . Laser in situ keratomileusis retreatment for residual myopia and astigmatism. J Refract Surg 2000; 16: 170–176.
Chiron 217C Technical Manual. Bausch & Lomb: Dornach, Germany, 1999.
NIDEK EC-5000 Technical Manual. Nidek Co. Ltd: Bunkyo-Ku, Tokyo, Japan, 1999.
Tsai RJ-F . Laser in situ keratomileusis for myopia of −2 to −25 diopters. J Refract Surg 1997; 13: S427–S429.
Feltham MH, Wolfe RW . Some variables to consider to avoid the need for LASIK surgical enhancements. Clin Exp Optom 2000; 83 (2): 76–81.
Balazsi G, Mullie M, Lasswell L, Lee PA, Duh YJ . Laser in situ keratomileusis with a scanning excimer laser for the correction of low to moderate myopia with and without astigmatism. J Cataract Refract Surg 2001; 27: 1942–1951.
Ditzen K, Handzel A, Pieger S, Ing D . Laser in situ keratomileusis nomogram development. J Refract Surg 1999; 15: S197–S201.
Roudakova TE, Kourenkov VV, Polounine GS . Planned undercorrection with laser in situ keratomileusis and photorefractive keratectomy for myopes over age 40. J Refract Surg 2000; 16: S261–263.
Huang D, Stulting RD, Carr JD, Thompson KP, Waring III GO . Multiple regression and vector analysis of laser in situ keratomileusis for myopia and astigmatism. J Refract Surg 1999; 15: 538–549.
Roberts C . The cornea is not a piece of plastic. J Refract Surg 2000; 16: 407–413.
Huang D, Steven S, Seffo F, Meisier DM, Krueger RR . Surgically-induced astigmatism after laser in situ keratomileusis for spherical myopia. J Refract Surg 2000; 16: 515–518.
Schults GS . Modulation of corneal wound healing. In: Krachmer JY, Mannis MJ, Holland EJ (eds). Fundamentals of Cornea and External Disease. Vol 1. Mosby: Missouri, 1997. pp 183–197.
Feltham MH, Stapleton F . Change in central corneal thickness following LASIK in myopia. Clin Exp Ophthal 2000; 28: 185–187.
Sharma S . Applied Multivariate Technique. Wiley: New York, 1996, pp 317–341.
Hosmer DW, Lemeshow S . Applied Logistic Regression. Wiley: New York, 2000, p 160.
Montes M, Chayet A, Gomez L, Magallanes R, Robledo N . Laser in situ keratomileusis for myopia of −1.50 to −6.00 Diopters. J Refract Surg 1999; 15: 106–110.
Salah T, Waring GO, El-Maghraby A, Moadel K, Grimm SB . Excimer laser in situ keratomileusis (LASIK) under a corneal flap for myopia of 2 to 20 D. Am J Ophthalmol 1996; 121: 143–155.
El Danasoury MA, El Maghraby A, Klyce SD, Mehrez K . Comparison of photorefractive keratectomy with excimer laser in situ keratomileusis in correcting low myopia (from −2.00 to −5.50 diopters). A randomized study. Ophthalmology 1999; 106: 411–421.
Lavery F . Laser in situ keratomileusis for myopia. J Refract Surg. 1998; 14: S177–178.
Hardten DR, Lindstropm RL, Samuelson TW, Chu YR . Laser in situ keratomileusis for myopia. Med J Allina 1999; 8: 1.
Dupps WJ, Roberts C . Effect of acute biomechanical changes on corneal curvature after photokeratectomy. J Refract Surg 2001; 17: 658–669.
Wilson SE . LASIK: Management of common complications. Cornea 1998; 17: 459–467.
Argento C, Valenzuela G, Huck H, Cremona G, Cosentino MJ, Gale MFR . Smoothness of ablation on acrylic by four different excimer lasers. J Refract Surg 2001; 17: 43–45.
Pesando PM, Ghiringhello MP, Tagliavacche P . Excimer laser in situ keratomileusis for myopia. J Refract Surg 1997; 13: 521–527.
Dada T, Sudan R, Sinha R, Ray M, Sethi H, Vajpayee RB . Results of laser in situ keratomileusis for myopia of −10 to −19 diopters with a Technolas 217 laser. J Refract Surg 2003; 19: 44–47.
Knorz MC, Liermann A, Seiberth V, Steiner H, Wiesinger B . Laser in situ keratomileusis to correct myopia −6.00 to −29.00 diopters. J Refract Surg 1996; 12: 576–584.
Guell JL, Muller A . Laser in situ keratomileusis (LASIK) for myopia from −7 to −18 diopters. J Refract Surg 1996; 12: 222–228.
Moniz N, Fernandes T, Kutty K, Narayana KK, Sreedhar A . Visual outcome in high myopia after laser in situ keratomileusis. J Refract Surg 2000; 16: S247–S250.
Maldonado-Bas A, Onnis R . Results of in situ keratomileusis in different degrees of myopia. Ophthalmology 1998; 105: 606–611.
Dougherty PJ, Kent L, Wellish MD, Maloney K . Excimer laser ablation and corneal hydration. Am J Ophthalmol 1994; 118: 169–176.
Feltham MH, Stapleton F . The effect of water content on the 193 nm excimer laser ablation. Clin Exp Ophthal 2002; 30: 99–103.
Muller LJ, Pels E, Gils FJM . The specific architecture of the anterior stroma accounts for maintenance of corneal curvature. Br J Ophthalmol 2001; 85: 437–443.
Lee G, Wilson G . Non-uniform swelling properties of the corneal stroma. Curr Eye Res 1981; 8: 457–461.
Kim W-S, Jo J-M . Corneal hydration affects ablation laser in situ keratomileusis surgery. Cornea 2001; 20: 394–397.
Rao S, Cheng AC, Fan DS, Leung AT, Lam DS . Effect of preoperative keratometry on refractive outcomes after laser in situ keratomileusis. J Cataract Refract Surg 2001; 27: 297–302.
Greenfield DS, Knighton RW, Huang X-R . Effect of corneal polarisation axis on assessment of retinal nerve fibre layer thickness by scanning laser polarimetry. Am J Ophthalmol 2000; 129: 715–722.
Acknowledgements
We thank Dr A Low FRCO and Professor Brian Brown and Dr Serina Stretton for paper review. This study was supported by the Australian Federal Government through the Cooperative Research Centres Programme (FS and RW).
Author information
Authors and Affiliations
Corresponding author
Additional information
Proprietary/competing interests: none
Rights and permissions
About this article
Cite this article
Feltham, M., Wong, R., Wolfe, R. et al. Variables affecting refractive outcome following LASIK for myopia. Eye 22, 1117–1123 (2008). https://doi.org/10.1038/sj.eye.6702856
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702856
