
Abstract
Purpose
To evaluate the long-term results of Erbium YAG-laser-assisted deep sclerectomy (DS). In this procedure, the delicate dissection of a deep corneoscleral lamella is greatly simplified by using the Erbium YAG-laser.
Methods
Data of 14 consecutive patients (10 male, four female, age 67.7±10.4 years), who underwent surgery from 1999 to 2000 were analysed retrospectively. The procedure was begun as a standard DS. The deep corneoscleral lamella was dissected with a pulsed Erbium YAG-laser (energy: 40–100 mJ, frequency: 5–10 Hz). Schlemm's canal was unroofed and the lamella thinned until aqueous percolated continuously through the membrane.
Results
The mean follow-up time was 50.4±6.8 months. The mean preoperative intraocular pressure (IOP) was 37.7±10.5 mmHg. The mean postoperative IOP was 16.1±3.9 mmHg at 1 month, 15.1±4.3 mmHg at 3 months, 16.4±4.5 mmHg at 12 months, and 17.6±8.7 mmHg at 50.5 months. The complete success rates (IOP⩽21 mmHg+IOP reduction ⩾20% without glaucoma medication) were 83.3% at 3 months and 50% at 12 and 50.5 months. Rates for qualified success (IOP⩽21 mmHg+IOP reduction ⩾20% with glaucoma medication) were 91.7% at 3 months, 92.9% at 12 months, and 78.6% at 50.5 months. The number of glaucoma medications was reduced from 3.07±0.92 preoperatively to 1.14±1.41 at 50.5 months. A single case of anterior-chamber penetration, requiring iridectomy, was the only intraoperative complication.
Conclusions
Erbium YAG-laser-assisted DS has the advantage of a greatly simplified dissection, while offering a successful long-term IOP control comparable to conventional DS.
Similar content being viewed by others


Introduction
Deep sclerectomy (DS) is a nonpenetrating filtering procedure, which is currently advocated as a standard procedure equivalent to trabeculectomy (TE). DS was introduced by Krasnov1 and developed further by Stegmann et al,2 who added viscocanalostomy. Subsequently, various modifications were proposed,3, 4, 5 yielding controversial results: several studies have shown that DS is comparable or less effective,6, 7, 8, 9, 10, 11 others that it is superior to standard TE in the treatment of open-angle glaucoma.2, 3 All authors described fewer early postoperative complications using this nonpenetrating technique than with TE.3, 5, 6, 7, 11
The dissection of the deep corneoscleral lamella is the most difficult part of the procedure. Previous studies showed that the dissection of the deep corneoscleral lamella with the Erbium YAG-laser might greatly simplify this delicate step, resulting only in a small thermal damage zone.12, 13, 14 Purpose of this study was to evaluate the long-term results of Erbium YAG-laser-assisted DS after a follow-up period of up to 56 months.
Materials and methods
From September 1999 to January 2000, 14 eyes of 14 consecutive patients (10 male, four female) eligible for primary DS for medically uncontrolled primary or secondary open-angle glaucoma were enrolled in the study. All patients underwent surgery at the Department of Ophthalmology of the Julius-Maximilians-University of Wuerzburg, Germany. The study was approved by the Local Ethics Committee and informed consent was obtained from all participants. The mean age, diagnosis, preoperative intraocular pressure (IOP), mean number of medical glaucoma treatment prior surgery, and mean preoperative visual acuity are listed in Table 1.
In six patients, argon laser trabeculoplasty had been performed at least 6 months before surgery. All patients had glaucomatous visual field defects in the eye enrolled in the study.
All surgeries were performed under general anaesthesia by a single experienced surgeon (WL) using an operating microscope throughout the procedure. An 8-mm fornix-based conjunctival flap was created and wetfield cautry was used for haemostasis. A 5 × 4 mm scleral flap of two thirds the scleral thickness was advanced approximately 1.0 mm into clear cornea tissue. The ablation of the deep corneoscleral lamella was then performed with a pulsed Erbium YAG-laser (Wavelight, Erlangen, Germany; model: Adagio®; see Table 2 for laser characteristics and settings) in an area of 4 × 3 mm2 (Figure 1). A zirconium fluoride fiberoptic with a quartz fiber tip in a modified vitrectomy hand piece were used to ablate tissue until aqueous humor percolated through the trabeculodescemetic membrane (TDM). During ablation, Schlemm's canal served as a well recognizable guiding landmark in every case, as the laser allows dissection layer by layer. As the wavelength of the Erbium YAG-laser is near the absorption maximum of water, the ablation is self-limited by the percolation of aqueous. To ensure sufficient ablation in the whole field, percolated aqueous had to be dried off the remaining tissue with a swab. A continuous aqueous ‘flow’, was the end point of the laser surgery. High-viscosity sodium hyaluronate (Healon GV®) was instilled into the created scleral lake. The scleral flap was closed with two to four 10-0 Nylon sutures, the conjunctiva was sealed with a running mattress-suture to insure a tight closure. Four milligrams of dexamethasone were injected subconjunctivally.

Surgical field after dissection of the deep corneoscleral lamella with the Erbium YAG-laser.
One young patient with pigmentary glaucoma and another POAG patient with severe allergies received intraoperative topical 5-fluorouracil (5-FU 40 mg/ml) in a sponge that was placed between sclera and Tenon's capsule for 3 min.
When signs of scarring appeared on examination of the filtering bleb (eg cork screw vessels, encapsulation or massive vascularisation), a series of postoperative 5-FU injections was started (5 mg of 5-FU in 0.5 ml balanced saline solution).
Follow-up examinations were done daily during the first week when the patients stayed as inpatients and at 1, 3, 12, and 50 months. Two Patients missed the 3 months appointment.
Complete success was defined as an IOP⩽21 mmHg and 20% pressure reduction without glaucoma medication and qualified success as an IOP⩽21 mmHg and 20% pressure reduction with glaucoma medication.
Results were analysed using the Student's t-test for comparison of means and Kaplan–Meier survival curves for long-term success rate analysis. Visual acuity was transferred to LogMar units for calculating the means and standard deviations. After calculation, the means were retransferred to Snellen format and the standard deviation was converted to lines (after Holladay15).
Results
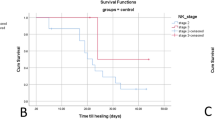
At 50.4±6.8 months of follow-up, surgery achieved a complete success in seven patients (50%) (Figure 2), qualified success in 11 patients, and had failed in three patients (Table 3). IOP was significantly decreased by the procedure (mean 53%), and no significant change in IOP was found from 1 month postoperatively to the last visit (Table 3). The development of visual acuity is listed in Table 4.

Cumulative complete success after Erbium YAG-laser-assisted deep sclerectomy using Kaplan–Meier table analysis.
The complications are listed in Table 5. One perforation of the TDM occurred intraoperatively, which required an iridectomy and conversion of the procedure to a TE (first case in series). Six patients developed cataract during follow-up, four of them had lens opacities before surgery. In all 14 patients filtration blebs developed, in two of them only after suturelysis 1 week after surgery. In 11 patients 5-FU was given subconjunctivally owing to early bleb fibrosis (mean 9.4±3.3 injections, range 4–13 injections). Needling of an encapsulated bleb was performed in two cases (4 weeks after surgery). However, both patients needed medication after 12 and 50 months and IOP was not controlled with medication in one of them. Six patients developed a transient corneal erosion after postoperative 5-FU treatment. In four patients, YAG-goniopuncture was performed (4–6 weeks after surgery) (Table 5). All of them were treated with 5-FU, three of them needed medication after 12 and 50 months.
Discussion
DS is difficult to master, even for an experienced surgeon. The main difficulty is the dissection of the deep corneoscleral lamella. Perforation of the thin TDM during dissection is reported to occur in 8–33% of patients16, 17 First trials encouraged us to dissect the TDM with an Erbium YAG-laser to improve safety.12 When dissecting with a blade, the major problems are either perforation into the anterior chamber or insufficient tissue removal.18 Laser ablation enables the surgeon to proceed layer by layer in a highly controlled manner. We found Schlemm's canal a valuable landmark in this procedure. A reflux of blood was seen when the roof of Schlemm's canal was ablated. The reflux of aqueous and blood halted the ablation, hence, only the roof could be removed and the lumen of the canal was preserved as a guiding landmark. It is remarkable that the dissection depth of the deep lamella varies dramatically with standard microsurgical technique, even when the procedure is performed by an experienced surgeon.18 Therefore, laser dissection offers improved safety to locate Schlemm's canal and dissect the important structures.
Previously, two studies on the use of Erbium YAG-laser in DS with a follow-up of up to 24 months have been published. Here, we provide long-term results with follow-up of more than 4 years. In 2002, Verges et al13 published excellent results after Erbium YAG-laser-assisted DS, with a complete success rate of 84.78% after 15 months (defined as an IOP⩽18 mmHg without medication), that was better than the results we could achieve. Pallikaris et al14 reported a complete success rate of 50% after 12 months and 37.5% after 24 months (defined as an IOP⩽21 mmHg without medication) with the same technique. At 12 months follow-up, our results are comparable to those of Pallikaris et al; Verges and Pallikaris used mitomycin C (MMC) intraoperatively to compensate for putative additional scarring induced by the laser treatment. In our series, only two patients received 5-FU during surgery, and a general use of MMC might have increased the success rate. On the other hand, the large differences in the results of Verges and Pallikaris argue against the idea that antimetabolites necessarily increase the complete success rate. Our results of IOP reduction, complete and qualified success, and reduction of antiglaucomatous medication are similar to those after standard DS.9, 16, 19 Without using a collagen implant or antimetabolites, DS results in an IOP reduction to the mid to high teens.9 No comparison of Erbium YAG-laser-assisted DS and trabeculectomy is available yet. Most of the studies comparing standard DS and TE reported a more favourable outcome after TE with a higher complete success rate, lower number of antiglaucomatous medications required postoperatively, and a lower IOP level after trabeculectomy.9, 10, 20, 21 Other studies reported DS and TE being equally effective.6, 7, 8, 11 Our results are similar to the results after trabeculectomy as reported in clinical trials comparing viscocanalostomy and TE (follow-up 1 year).10, 20 Regarding a retrospective long-term analysis comparing intensified postoperative care and conventional follow-up, the long-term complete success rate after Erbium YAG-laser-assisted deep sclerectomy is superior to the results after conventional follow-up and inferior to intensified postoperative care after trabeculectomy.22
The concept of reducing early postoperative complications from penetrating glaucoma surgery by performing DS was confirmed in most studies evaluating nonpenetrating procedures.3, 5, 6, 7, 8, 9, 11 In our study, the rate of complications was low. The single patient with intraoperative perforation of the TDM and subsequent iridectomy developed a flat anterior chamber and choroidal detachment. One other patient had a flat anterior chamber and a mild hyphaema. Three further patients had a transient choroidal detachment. The rate of choroidal detachment, hyphema, and shallowing of the anterior chamber is comparable to the data in the literature (range: 0–33%).11, 13, 14, 17, 23
Average preoperative BCVA was low in our study group, as two patients had poor visual fields, two patients developed cataracts and pre-existing cataracts progressed in another four patients. Other studies with a long-term follow-up have shown similar cataract progression rates compared to our study.24, 25 The rate of newly developed cataract is slightly higher in our study compared to published data, but might be biased by our relatively small sample size.16, 23
The main postoperative concern in our study was filtering bleb scarring. All 14 patients developed a filtering bleb, which is in line with other studies.9, 11, 13, 14 Eleven of them required 5-FU injections due to signs of bleb fibrosis. This indicates a role of subconjunctival aqueous drainage in IOP reduction after DS or laser-assisted DS. Others reported 5-FU injection rates between 6 and 50%.8, 13, 14, 16 The number of YAG-goniopunctures performed in our study is lower compared to published data,16, 19, 24 which might be owing to the exact dissection with the laser, resulting in a very thin TDM.
A frequent use of 5-FU in postoperative care might indicate a scar promoting effect of the laser treatment, although the tissue damage caused by Erbium YAG-laser is minimal in histological studies (10–30 μm).12, 26 Use of an Excimer laser may be beneficial as it inflicts no significant thermal tissue damage27, 28 and has been used successfully in deep sclerectomy. On the other hand, the Erbium YAG-laser is less costly (approx. 60 000€) and offers several functional opportunities, for example, in plastic surgery.29 Running costs range at approximately 5€ for a disposable sleeve to cover the fiberoptic.
Our long-term results indicate, that Erbium YAG-laser dissection in DS provides similar long-term results as mechanical dissection,9, 16, 19 while greatly facilitating the surgery. This is of particular interest to surgeons with a lower case load, who wish to have the advantage of less early postoperative complications that DS offers.
References
Krasnov MM . Microsurgery of glaucoma. Indications and choice of technique. Am J Ophthalmol 1969; 67: 857–864.
Stegmann R, Pienaar A, Miller D . Viscocanalostomy for open-angle glaucoma in black African patients. J Cataract Refract Surg 1999; 25: 316–322.
Zimmerman TJ, Kooner KS, Ford VJ, Olander KW, Mandlekorn RM, Rawlings EF et al. Trabeculectomy vs nonpenetrating trabeculectomy: a retrospective study of two procedures in phakic patients with glaucoma. Ophthalmic Surg 1984; 15: 734–740.
Arenas E . Trabeculectomy ab externo. Highlights Ophthalmol 1991; 9: 59.
Carassa RG, Bettin P, Fiori M, Brancato R . Viscocanalostomy: a pilot study. Eur J Ophthalmol 1998; 8: 57–61.
Gianoli F, Schnyder CC, Bovey E, Mermoud A . Combined surgery for cataract and glaucoma: phacoemulsification and deep sclerectomy compared with phacoemulsification and trabeculectomy. J Cataract Refract Surg 1999; 25: 340–346.
Mermoud A, Schnyder CC, Sickenberg M, Chiou AG, Hediguer SE, Faggioni R . Comparison of deep sclerectomy with collagen implant and trabeculectomy in open-angle glaucoma. J Cataract Refract Surg 1999; 25: 323–331.
EL Sayyad F, Helal M, El-Kholify H, Khalil M, El-Maghraby A . Nonpenetrating deep sclerectomy versus trabeculectomy in bilateral primary open-angle glaucoma. Ophthalmology 2000; 107: 1671–1674.
Chiselita D . Non-penetrating deep sclerectomy versus trabeculectomy in primary open-angle glaucoma surgery. Eye 2001; 15: 131–132.
Jonescu-Cuypers C, Jacobi P, Konen W, Krieglstein G . Primary viscocanalostomy versus trabeculectomy in white patients with open-angle glaucoma: A randomized clinical trial. Ophthalmology 2001; 108: 254–258.
Schwenn O, Springer C, Troost A, Yun SH, Pfeiffer N . Deep sclerectomy using a hyaluronate implant versus trabeculectomy. A comparison of two glaucoma operations using mitomycin C. Ophthalmologe 2004; 101: 696–704.
Klink T, Lieb W, Grehn F . Erbium-YAG laser-assisted preparation of deep sclerectomy. Graefes Arch Clin Exp Ophthalmol 2000; 238: 792–796.
Verges C, Llevat E, Bardavio J . Laser-assisted deep sclerectomy. J Cataract Refract Surg 2002; 28: 758–765.
Pallikaris IG, Kozobolis VP, Christodoulakis EV . Erbium: YAG laser deep sclerectomy: An alternative approach to glaucoma surgery. Ophthalmic Surg Lasers Imaging 2003; 34: 375–380.
Holladay JT . Proper method for calculating average visual acuity. J Refract Surgery 1997; 13: 388–391.
Karlen ME, Sanchez E, Schnyder CC, Sickenberg M, Mermoud A . Deep sclerectomy with collagen implant: medium term results. Br J Ophthalmol 1999; 83: 6–11.
Drolsum L . Conversion from trabeculectomy to deep sclerectomy. Prospective study of thefirst 44 cases. J Cataract Refract Surg. 2003; 29: 1378–1384.
Dietlein TS, Luke C, Jacobi PC, Konen W, Krieglstein GK . Variability of dissection depth in deep sclerectomy: morphological analysis of the deep scleral flap. Graefes Arch Clin Exp Ophthalmol 2000; 238: 405–409.
Shaarawy T, Mermoud A . Deep sclerectomy in one eye vs deep sclerectomy with collagen implant in the contralateral eye of the same patient: long-term follow-up. Eye 2005; 19: 298–302.
Luke C, Dietlein TS, Jacobi PC, Konen W, Krieglstein GK . A prospective randomized trial of viscocanalostomy versus trabeculectomy in open-angle glaucoma: a 1-year follow-up study. J Glaucoma 2002; 11: 294–299.
O'Brart DP, Shiew M, Edmunds B . A randomised, prospective study comparing trabeculectomy with viscocanalostomy with adjunctive antimetabolite usage for the management of open angle glaucoma uncontrolled by medical therapy. Br J Ophthalmol 2004; 88: 1012–1017.
Marquardt D, Lieb WE, Grehn F . Intensified postoperative care versus conventional follow-up: a retrospective long-term analysis of 177 trabeculectomies. Graefes Arch Clin Exp Ophthalmol 2004; 242: 106–113.
Lachkar Y, Neverauskiene J, Jeanteur-Lunel MN, Gracies H, Berkani M, Ecoffet M et al. Nonpenetrating deep sclerectomy: a 6-year retrospective study. Eur J Ophthalmol 2004; 214: 26–36.
Shaarawy T, Mansouri K, Schnyder C, Ravinet E, Achache F, Mermoud A . Long-term results of deep sclerectomy with collagen implant. J Cataract Refract Surg 2004; 30: 1225–1231.
Shaarawy T, Karlen M, Schnyder C, Achache F, Sanchez E, Mermoud A . Five-year results of deep sclerectomy with collagen implant. J Cataract Refract Surgery 2001; 27: 1770–1778.
Bende T, Seiler T, Wollensak J . Photoablation with the Er:YAG laser in ocular tissues. Fortschr Ophthalmol 1991; 88: 12–16.
Argento C, Sanseau AC, Badoza D, Casiraghi J . Deep sclerectomy with a collagen implant using the excimer laser. J Cataract Refract Surg 2001; 27: 504–506.
Maldonado-Bas A, Maldonado-Junyent A . Filtering glaucoma surgery using an excimer laser. J Cataract Refract Surg 2001; 27: 1402–1409.
Lieb WE, Klink T, Muennich S . CO2 and Erbium YAG laser in eyelid surgery: a comparison. Ophthalmologe 2000; 97: 835–841.
Author information
Authors and Affiliations
Corresponding author
Additional information
None of the authors has a financial or proprietary interest in any material, instrument or method mentioned.
None of the authors has received public or private financial support for the study.
Rights and permissions
About this article
Cite this article
Klink, T., Schlunck, G., Lieb, W. et al. Long-term results of Erbium YAG-laser-assisted deep sclerectomy. Eye 22, 370–374 (2008). https://doi.org/10.1038/sj.eye.6702641
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702641
