
Abstract
Recurrent corneal erosions (RCE) are common. They are characterised by repeated episodes of pain, difficulty in opening the eyes, watering, and photophobia resulting from poor epithelial adhesion. In the majority of patients with RCE, trauma is the initiating factor. Epithelial, stromal, and endothelial corneal dystrophies have all been described in association with RCE. Other causes that may lead to RCE include chemical and thermal injuries, previous herpetic keratitis, meibomian gland dysfunction, ocular rosacea, diabetes mellitus, Salzmann's nodular degeneration, band keratopathy, previous bacterial ulceration, kerato-conjunctivitis sicca, and epidermolysis bullosa. The conditions that are associated with RCE can be either primary or secondary depending on whether the basement membrane complex abnormality is intrinsic or acquired. Primary types tend to be bilateral, symmetrical and develop in multiple corneal locations. The pathogenetic mechanism of this disorder is related to poor adhesion of the corneal epithelium to the underlying stroma. Excessive matrix metalloproteinase (MMP) activity may play a role in the pathogenesis. Although the majority of patients will respond to simple measures such as padding and antibiotic ointment, RCE resistant to simple measures require approaches that are more elaborate. The common goal of these approaches is to encourage proper formation of adhesion complexes between the epithelium and the stroma. The use of long-term contact lenses, autologous serum eye drops, botulinum toxin, induced ptosis, oral MMP inhibitors, diamond burr polishing of Bowman's membrane have been reported with varying degree of success in treating RCE. Anterior stromal puncture with insulin needles or Neodymium : aluminium–yttrium–garnet may enhance the epithelial adhesion to the basement membrane by scar formation and success rates of up to 80% have been reported in the treatment of recalcitrant RCE. Excimer laser photo-therapeutic keratectomy (PTK) is now a well-established treatment modality for RCE and is being used both safely and effectively. Partial ablation of Bowman's layer with PTK gives a smooth surface for the newly generating epithelium to migrate and form adhesion complexes. The pathogenesis, clinical features, and management options of this common disorder are discussed in this review article.
Similar content being viewed by others

Introduction
Traumatic and spontaneous corneal epithelial erosions are common. While most epithelial erosions heal without any sequelae, a small proportion of these recur spontaneously.1 Recurrent corneal erosion is characterised by episodes of pain, redness, photophobia, and tearing. This clinical entity was first described by Hansen in 1872 and was termed ‘intermittent neuralgic vascular keratitis’. Diverse factors have been attributed to the pathogenetic mechanisms, and not surprisingly, a variety of therapeutic approaches have been advocated. The aim of the article is to review current theories on the pathogenesis and management of this common disorder.
Aetiology
The majority of patients presenting with recurrent corneal erosions (RCE) give a history of trauma. This can be trivial such as a glancing blow from a fingernail, leaf of a tree, or even the edge of a piece of paper.2 It is a common misconception that abrasions caused by finger nails, particularly that by a baby's, are more likely to progress to RCE.1, 3, 4 When RCE presents without obvious trauma, an underlying factor should be suspected. Epithelial, stromal, and endothelial corneal dystrophies have all been described in association with RCE.5 Table 1 lists other causes conditions associated with RCE.2, 6, 7, 8, 9 The conditions that are associated with RCE can be classified as either primary or secondary depending on whether the BM complex abnormality is intrinsic or acquired (Table 1). Primary types tend to be bilateral, symmetrical and develop into multiple corneal locations.
Clinical features
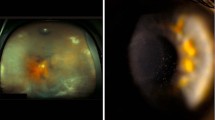
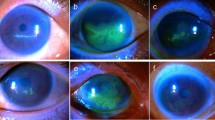
Symptoms of pain, redness, photophobia, and tearing, typically occur on waking and may be related to rapid eye movements during sleep10, 11, 12 or rapid opening of the eyelids. Delayed epithelialisation, persistent sloughing of the newly formed epithelium, and recurrent episodes of epithelial loss are common problems. The duration of symptoms may vary depending on the type of erosion. Corneal infiltrates may develop at the site of corneal erosions.13 The incidence of recurrence was shown to be 1 : 150 cases following traumatic abrasion.1 Chandler4, in 1945, divided the syndrome of RCE into macroform and microform types (Table 2). Microform erosions are less severe, last for hours, but occur more frequently; sometimes every night or morning.6 Macroform erosions, however, persist for several days (1–21 days).12 With microform erosions, the epithelial breakdown is small compared to macroform erosions, where the break is larger with surrounding loosely adherent epithelium. Microform erosions may be spontaneous and are associated with epithelial basement membrane dystrophy (EBMD), unlike macroform erosions that are traumatic in origin.10 (Figure 1).

Recurrent corneal erosions can be macroform (a and b) or microform types (c and d). In macroform erosions, the epithelial breakdown is large with surrounding loosely adherent epithelium compared to microform erosions, where the break is small and blister like.
The appearance of the affected cornea varies from loosely adherent and elevated epithelium, epithelial microcysts, or corneal epithelial defects, to stromal infiltrates and opacities.3, 14, 15 The majority of acute corneal erosions occur within the lower half of the cornea, irrespective of the aetiology.2 It has been suggested that recurrences occur in close proximity to the Hudson-Stahli line.16 In moderate and large-sized erosions involving the central cornea, the last area to re-epithelialise is in the midline below the horizontal meridian. This is because the centripetally moving convex fronts of healing epithelium meet at the apex, and the integration of different fronts of basement membrane takes longest at this point, thus predisposing it to subsequent breakdown.17 Other factors such as upper lid movement across the ocular surface and local tear film drying are also most likely to disrupt the surface at this site.2
Occasionally frank bacterial keratitis can develop in a patient with RCE. Prolonged use of bandage contact lenses and topical steroids may predispose to bacterial corneal ulcers.
Pathogenesis
Pathological anatomy
Epithelial cells rest on the basement membrane. The normal adhesion of the corneal epithelium is maintained by structures known as adhesion complexes that are composed of hemidesmosomes, the lamina densa, and the lamina lucida of the basement membrane, anchoring fibrils, laminin, fibronectin, and type IV and VII collagen.18 Numerous hemidesmosomes, a major constituent of the adhesion complex, are scattered on the basal side of the epithelial cells. Fine fibrils radiate from the hemidesmosomes into the basement membrane to join them together. Immediately after the removal of the corneal epithelium, the denuded stroma in the area of the epithelial defect is coated with fibronectin. This provides a platform for the adjacent viable epithelial cells to slide and migrate to cover the denuded area, and to proliferate to form the superficial cells. The basal cells form adhesion complexes with the underlying structure.
The status of the BM at the time of initial injury could, however, influence the outcome of epithelial healing. Animal studies have shown that in epithelial injuries that involve removal of basement membranes, both the epithelial cell migration is delayed and it takes several weeks to become adherent to the underlying stroma. In contrast, with an intact BM, epithelial cells migrate onto the old BM and form adhesion complexes with subsequent stable epithelial adhesion in a few days.
Formation of defective junctional complexes following epithelial trauma has been observed in RCE. This observation of delayed adhesion of epithelial cells to underlying structures in certain types of injuries has become the basis of the investigation of the role of adhesion complexes in RCE. Reattachment of corneal epithelium following an initial abrasion appears to be faulty in RCE.19, 20 In RCE, a variety of adhesion complex defects have been observed that include: reduplication of BM, loculation of connective tissues, absence of BM and hemidesmosomes.20, 21, 22 The corneal epithelium may contain pale, swollen basal epithelial cells. Pseudocystic collections of cellular and amorphous debris are found within the epithelium and are thought to be due to entrapment of the epithelium by aberrant basement membrane. This feature may be due to the abnormal BM adhesion complexes leading to a periodic elevation of the epithelium and the accumulation of underlying debris before erosions occur. This leads to further formation of abnormal basement membrane and the cycle is self-perpetuating. It has been postulated that the epithelial separation is maximal at night time due to superficial epithelial oedema induced by hypotonicity of the tears due to lack of evaporation.4 During sleep and lid closure, the surface tension of the tears may cause adherence between the lids and corneal epithelium. Opening the eye quickly gives a shearing force, which is greater than the force of adherence of the affected area of epithelium, and this may result in epithelial avulsion.
Role of meibomian gland dysfunction
Hope-Ross et al6observed a higher incidence of meibomian gland dysfunction in patients with RCE that are nontraumatic in origin. They observed that recurrent corneal erosion most commonly occurred at the inferior cornea, which has maximum contact with the tear film, rather than at the site of the injury.6 Extensive meibomian gland dysfunction and acne rosacea was seen in patients with recalcitrant RCE.6 This was in the form of inspissation of meibomian glands, reduced tear film break-up time, conjunctival injection, and accompanying facial cutaneous changes such as facial erythema, flushes, papules, and pustules.6 Current evidence suggest the pathogenesis of impaired epithelial healing may be multifactorial. Staphylococcus epidermidis colonisation of the lid margins of acne rosacea patients have been well documented and this has a tendency to produce higher levels of bacterial lipases.23 Lipases act upon wax and sterol esters from meibomian secretions, thus producing toxic free fatty acids. Increased fatty acid levels in tears have been postulated to interfere with the healing process, and subsequent formation of incompetent hemidesmosomes and junctional complexes that predispose to RCE.24, 25, 26 Furthermore, elevated concentrations of interleukin-1 and MMP-9 in the tears have been found in acne rocacea-related meibomian gland dysfunction.27 It therefore appears that meibomian gland inflammation affects the health of the corneal epithelium and these findings have therapeutic implications.
Role of MMP activity
Extracellular matrices provide the structural organisation to the cornea, and a key component of balanced wound healing involves extra-cellular matrix production and later, extra-cellular matrix degradation. In the cornea, the matrices include the stroma, Bowman's layer, Descemet's membrane, and the corneal epithelial basement membrane. The matrices undergo constant, slow remodelling during health and rapid remodelling during repair.28, 29, 30, 31, 32 Corneal stromal remodelling during wound healing is mediated by a group of zinc containing degradative enzymes known as matrix metalloproteinases (MMPs).33, 34 They appear in a precisely controlled sequence that suggest they perform specific roles.33, 34 Corneal epithelial cells and fibroblasts are the sources of MMP.33, 34 MMPs have been further implicated in cytokine activation, cleavage of cell adhesion molecules, and the creation of biologically active fragments.35, 36, 37 During corneal wound-healing, matrix metalloproteinase-9, (MMP9) also known as gelatinase-B (Gel-B), up-regulation is responsible for degradation of damaged matrix during re-epithelialisation, and for stromal remodelling after the epithelialisation is complete.33, 34 Elevated levels of MMP-2 and MMP-9 have been observed in the tear fluid of patients with RCE. Higher than required levels of MMPs may dissolve old and newly forming BM. Mechanical adhesion provided by this malformed BM may be inadequate, thus resulting in RCE.38, 39
Differential diagnosis
Recurrent breakdown of corneal epithelium may be seen in self-inflicted corneal injury, exposure keratitis, recurrence of herpes simplex keratitis, neurotropic keratitis, roughening of the tarsal plate and foreign bodies under the tarsal plate. Presentations of recurrent corneal epithelial defects due to self-inflicted injury are rare but the authors have encountered two such patients; one female and the other male and both in their late thirties. Recurrent epithelial defects due to neurotropic keratitis are painless. Recurrent herpes simplex stromal keratitis may show an epithelial defect. Past history of dendritic ulceration, gradual onset of pain and deep stromal infiltration are features that may differentiate herpes related disorders from true recurrent corneal erosion.
Management of RCE
Regardless of the aetiology of RCE, the common fault is the basic incompetence of the basement membrane and its failure in stabilising epithelial adhesion to the underlying stroma. In addition to pain relief during the acute phase, the aim of the management of RCE is directed towards promoting re-epithelialisation and re-establishment of a competent basement membrane complex. The healed epithelium should remain intact for a sufficient length of time to allow the reformation of adhesion complexes. Various conservative non-surgical and more aggressive surgical modalities have been found to be therapeutically useful (Table 3).
In the majority of cases the acute episode can be successfully managed by patching, cycloplegia and topical antibiotic ointment.2, 3, 4, 38 It is a common practice to use non-steroidal anti-inflammatory drops to relieve pain. Although these drops are effective analgesics, they should be administered cautiously as non-steroidal anti-inflammatory drops may delay epithelial healing.40 Conservative treatment in the form of topical lubrication, hypertonic agents and soft bandage contact lenses are usual initial therapeutic choices to prevent recurrences.2, 3, 4, 6, 12, 38 Lubrication is the mainstay of treatment, which can be in the form of drops, gels or ointment. The bedtime application of ointment prevents desiccation of the epithelium overnight and protects the epithelium from the shearing action of the eyelid on wakening. Hypertonic sodium chloride, either drops or ointment, has been advocated to promote epithelial adherence by decreasing epithelial oedema, which tends to occur overnight when the lids are shut. Most patients do well with conservative treatments12 which are effective in relieving the pain and initial healing, but do not appear to reduce the recurrence rate of RCE2 and in fact may worsen the prognosis.11 Further studies are necessary to evaluate the efficacy of prophylactic night time ointment. Patients commonly wake with their eyes closed and are fearful of opening them. It is our experience that advice to move the eyes slowly to the left and right before opening them, anecdotally reduces the frequency of recurrent erosions. The rationale is that the cornea is separated from the tarsal plate slowly prior to rapid eyelid opening.
Non invasive management of recalcitrant cases
RCE resistant to simple measures requires more elaborate approaches. Non invasive options include the use of long term contact lenses, autologous serum eye drops, botulinum toxin induced ptosis, and the administration of oral MMP inhibitors.41
General measures and care of associated lid pathology
Meibomian gland dysfunction has a profound effect on the health of the ocular surface. Chronic blepharitis is associated with the release of bacterial lipases, fatty acids, interleukins and MMPs from the inflamed meibomian glands that may impair corneal epithelial healing. Previous studies have shown that RCE are associated with chronic blepharitis and acne rosacea.6, 42 Appropriate therapeutic measures such as lid hygiene and oral tetracyclines are useful in reducing episodes of RCE.6, 42 Tetracylines not only reduce the free fatty acids in the tear pool of patients with meibomian gland dysfunction, but also reduce the number of colony forming units cultured from the eyelids. Oral tetracyclines, in low doses. are effective in controlling meibomian gland dysfunction and need to be continued at least for three months. Blepharitis associated with acne rosacea may require treatment for prolonged lengths of time, as discontinuation of tetracyclines is commonly associated with recurrences of rosacea.
Inhibitors of MMP
A combination of oral doxycycline and topical steroids can be used successfully in recalcitrant cases of RCE.43 This approach is based on biochemical evidence implicating increased levels of MMP activity in the pathogenesis of this condition.31, 38, 44 Doxycycline has been shown to produce a 70% decrease in the activity of metalloproteinase-9 in unstimulated human corneal epithelial cultures.45 Both topical steroids and oral doxycycline were reported to decrease the frequency of RCE in one randomised controlled clinical trial.42 The corneal epithelium produces gelatinase B (metalloproteinase −9) an enzyme that plays a role in the wound healing process.44, 46 Gelatinase B has been detected in the corneal basal epithelial cells at the edges of non-healing corneal ulcers in humans. This suggests that excessive production or inadequate neutralisation of the enzyme can have pathological consequences.31 Garrana et al reported that the expression of metalloproteinase-2 was upregulated in corneas with recurrent erosions. These findings suggest that MMPs may be responsible for the breakdown of the anchoring molecules in the basement membrane during epithelial healing, and this is the basis for the use of inhibitors of MMP in the treatment of RCE.43
The therapeutic effects of doxycycline and corticosteroids may also be due to their anti-inflammatory properties. Doxycycline decreases the synthesis and bioactivity of interleukin-1 produced by cultured human epithelial cells.47 Thus, a combination of medications that inhibits MMP-9 has the potential to produce rapid resolution and prevents further recurrence in cases with RCE.43 Although steroids are effective in treating RCE they should be used cautiously, particularly in patients with a thin corneal stroma as they may inhibit collagen synthesis.
Autologous serum
Autologous serum supplies the eye surface with several substances that are essential for recovery of the injured epithelium such as vitamin A, epidermal growth factor, transforming growth factor, fibronectin, and many other cytokines. Autologous serum has a composition similar to that of tears and provides the ocular surface with the basic nutrients for epithelial renewal that are lacking in commercial preparations. Fibronectin promotes epithelial cell migration and anchorage.48 The oil present in the serum may act as a substitute for the lipid components produced by meibomian glands, and prealbumen contributes to the stability of the tear film.49 The treatment is safe with no secondary effects.50 However, further studies are needed on larger series and with longer follow-up to determine the ideal duration of treatment and the mechanism of action.
Therapeutic bandage contact lenses
A therapeutic bandage contact lens may be placed if the epithelial defect is large. Therapeutic contact lenses promote epithelial migration, basement membrane regeneration, and epithelial–stromal adhesion by protecting the ocular surface from the sweeping action of the upper lid.51 Collagen corneal bandage lenses have also been reported to accelerate re-epithelialisation and to prevent relapses of recurrent erosions.52, 53 However, long-term continuous use of contact lenses may predispose to bacterial keratitis, vascularisation, and scarring.54, 55 Therapeutic contact lenses should be used under close supervision in recurrent corneal erosion and, to be effective, a bandage contact lens should be worn for a minimum of 6 weeks to several months.2 This may enable the formation of stable junctional complexes. Long-term wear is, however, associated with corneal infection and neovascularisation.2 A prospective trial of contact lenses vs lubrication in patients with RCE found that contact lenses were inferior and showed a higher complication rate.16 The authors have a similar experience, and we generally do not use bandage contact lenses for more than a week in the presence of an epithelial defect.
Surgical management of RCE
In patients, who do not respond to medical treatment, surgical therapy can be very successful. Diamond burr polishing of Bowman's membrane, anterior stromal puncture with an insulin needle or by means of Neodymium : aluminum–yttrium–garnet (YAG) laser, and excimer laser photo-therapeutic keratectomy(PTK) are the surgical modalities reported to be most successful when medical treatments fail. Given the relatively high success rate and low risk of surgical treatment for RCE, medical treatment should not be prolonged when unsuccessful. Although there are no clear guidelines for surgical indication, significant erosions more than once a month warrant consideration for surgical intervention.56
Debridement of loose epithelium
Debridement of loose epithelium is believed to promote healing from the healthy edge. Epithelial debridement may be performed under topical anaesthesia with the slit-lamp biomicroscope. The loosely adherent epithelium may be removed either with a sterile sponge or a number 15 BP blade. Topical antibiotics are necessary to prevent secondary infection. A therapeutic bandage contact lens may be placed if the epithelial defect is large. Cyclopentolate drops and oral analgesics may be prescribed to relieve pain. However, there is no current evidence to suggest that epithelial debridement alone can reduce the recurrences of epithelial erosions.2, 3, 12 We believe that epithelial debridement is indicated only when the epithelium is loose and freely mobile on the underlying stroma. The underlying stroma should not be disturbed to avoid scarring.
Anterior stromal puncture
McLean et al57proposed the use of anterior stromal puncture in RCE after an interesting observation that recurrent corneal erosion is not seen after corneal injury with deeply embedded foreign bodies or deep stromal laceration. The therapeutic aim of anterior stromal puncture is to enhance the epithelial adhesion to the basement membrane by scar formation and success rates of up to 80% have been reported in recalcitrant RCE.14, 57, 58 It is generally accepted that these procedures may involve reactive fibrosis or production of extra cellular matrix proteins responsible for proper adhesion of the epithelium to its substrate.59 The procedure is performed with topical anaesthesia with a bent 25 gauge (0.1–0.3 mm turned end) needle attached to a 3 ml syringe. Multiple superficial punctures are placed approximately 0.5 mm apart in the affected area. Treatment is extended at least 1 mm into the normal epithelium bordering the lesion. Fluorescein can be instilled topically before the treatment to define the affected area better. Immediately after the treatment, a contact lens is placed and antibiotics are given post-treatment for 1 week.12 Anterior stromal puncture can also be performed with a short pulsed Nd : YAG laser.60, 61 Energy levels between 1.8 and 2.2 mJ can be used to treat erosions. The advantage of laser puncture over needle puncture is that the laser puncture is more reproducible, shallow, and translucent. Anterior stromal puncture may result in subepithelial scars and its use is not advisable if the erosion encroaches upon the visual axis as the resulting scar may result in glare and a reduction in the visual acuity.2
Photo-therapeutic keratectomy
Excimer laser, with its facility to ablate corneal tissue with extreme precision and minimal adjacent tissue damage has been a useful tool in the management of RCE. Studies have shown that partial ablation of Bowman's layer gives a smooth bed for migrating epithelium, and results in new hemidesmosomal adhesional complexes.18, 62, 63 Histological studies of excimer laser ablated monkey corneas have shown increased amounts of type 7 collagen, a major component of anchoring fibrils and hemidesmosomes along the basement membrane of the basal epithelial cells.63, 64 Human studies have shown that the basal epithelial layer forms hemidesmosomes and new basement membrane within 2 weeks of photoablation.65 In addition, undulations are most noticeable on the edge of the ablated zone, which would greatly increase the surface area of attachment. Thus, new hemidesmosomes, anchoring fibrils, and epithelial basement membrane are synthesized rapidly and in increasing amounts after PRK, and problems with epithelial instability would therefore not be expected. In the treatment of recalcitrant erosions, it is possible that both the removal of the abnormal epithelium and the basement membrane are important for a successful outcome. The former results in regeneration of the basal epithelial cells and the latter will allow the epithelium to come into direct contact with stromal elements, stimulating the synthesis of new anchoring fibrils and hemidesmosomes.66
Excimer laser PTK is now a well-established treatment modality for RCE and is being used both safely and effectively.66, 67, 68, 69 Ablation of the cornea with the excimer laser allows removal of corneal tissue with extreme precision and without damage to the nonirradiated area. The second advantage is that large beam cross-sections, typically several millimeters in diameter, allow simultaneous treatment of wider areas. Although there are slight variations in techniques between centres, the aim of this approach is to remove a 6.0 μm thick anterior stromal layer from Bowman's layer. Briefly, the defective epithelium is removed with a cellulose sponge and a 7.0–8.0 mm diameter flat beam is programmed to ablate a 6.0 μm layer of the anterior stroma. The eye is usually padded after cycloplegic and antibiotic drops. A minority of patients may require bandage contact lenses during the postoperative follow-up.70 PTK is an effective treatment for RCE, with a success rate between 60 and 100%.67, 71 This variability in success rate may be due to the initial indication for PTK in the various studies carried out. PTK carries a higher rate of success for RCE following trauma than corneal dystrophies.67, 71
Post-operative pain is a disadvantage of PTK as the central corneal epithelium is removed exposing the underlying nerve plexus. Ardjomand et al have introduced a modification to overcome this problem. Instead of removing the epithelium completely they peel the epithelium with an epipeeler, the epithelium is left at a 12 O’clock hinge, and then PTK is carried out. At the end of this procedure, the epithelium is placed back. This technical modification has the advantage of fast post-operative visual rehabilitation and reduced postoperative pain. The main undesirable effect of PTK is that central flattening of the cornea induces a hyperopic shift, which is related to the ablation depth. However with modern PTK, profiles inducing refractive changes appear less likely, compared to those with older broader beam lasers.72 PTK can also be combined with PRK in appropriate cases.70 Although very effective, PTK requires an expensive excimer laser and only a few NHS centres have this facility in the UK.
Diamond burr superficial keratectomy
Epithelial debridement and diamond burr polishing of Bowman's membrane has rarely been reported in the treatment of RCE. Animal experiments show that diamond burr superficial keratectomy (DB) leads to faster re-epithelialisation and a smoother corneal surface compared to surgical blade keratectomy. In DB treatment, loose sheets of epithelium are debrided from the cornea using a combination of peeling with forceps and gentle wiping with an iris spatula and a cellulose sponge. In cases where the erosion is close to or within the visual axis, the entire corneal surface is polished with a fine diamond burr, using multiple, even, circular movements to prevent irregular topography. In order to ensure uncomplicated re-epithelialisation, a narrow 1–2 mm rim of the corneal epithelium is left intact in the circumferential periphery. Treatment is limited to no deeper than the anterior part of Bowman's layer. A bandage contact lens is inserted and antibiotics can be given following the treatment. DB treatment offers an alternative method of treating RCE and the results are comparable to PTK.73 In a series of 13 cases reported by Buxton and Fox,74only one patient failed to achieve notable improvement. Although a subtle granular epithelial/subepithelial deposit was noticed in all cases, the haze cleared in 6–12 weeks. In a small series involving 42 eyes with RCE and anterior basement membrane dystrophy, the tendency to develop haze was found to be less compared to PTK.56 DB treatment is a simple, less expensive outpatient procedure with a smaller incidence of haze and fewer recurrences compared to PTK. Futhermore, DB can be used to treat RCE involving the visual axis. Retreatments are simple and DB is more widely available than PTK. Long-term studies are, however, required to confirm the efficacy of DB treatment in the management of RCE.
Conclusion
RCE are common and may lead to visual disability. The majority of cases will respond to simple, conservative medical treatment. However, a minority of patients will require surgical intervention. As has been discussed, various therapeutic approaches have been advocated to manage this condition. The ultimate method of intervention should be based on the nature and degree of the pathology, the expertise of the attending physician, and the facilities that are available.
References
Jackson H . Effect of eye-pads on healing of simple corneal abrasions. BMJ 5200; 713: 1960.
Hykin PG, Foss AE, Pavesio C, Dart JK . The natural history and management of recurrent corneal erosion: a prospective randomised trial. Eye 1994; 8 (Part 1): 35–40.
Brown N, Bron A . Recurrent erosion of the cornea. Br J Ophthalmol 1976; 60: 84–96.
Chandler P . Recurrent corneal erosion of the cornea. Am J Ophthalmol 1945; 28: 355–363.
Bron AJ, Burgess SE . Inherited recurrent corneal erosion. Trans Ophthalmol Soc UK 1981; 101 (Part 2): 239–243.
Hope-Ross MW, Chell PB, Kervick GN, McDonnell PJ . Recurrent corneal erosion: clinical features. Eye 1994; 8 (Part 4): 373–377.
Friend J, Thoft RA . The diabetic cornea. Int Ophthalmol Clin 1984; 24: 111–123.
Jenkins MS, Brown SI, Lempert SL, Weinberg RJ . Ocular rosacea. Metab Pediatr Syst Ophthalmol 1982; 6: 189–195.
Jenkins MS, Brown SI, Lempert SL, Weinberg RJ . Ocular rosacea. Am J Ophthalmol 1979; 88: 618–622.
Heyworth P, Morlet N, Rayner S, Hykin P, Dart J . Natural history of recurrent erosion syndrome—a 4 year review of 117 patients. Br J Ophthalmol 1998; 82: 26–28.
Eke T, Morrison DA, Austin DJ . Recurrent symptoms following traumatic corneal abrasion: prevalence, severity, and the effect of a simple regimen of prophylaxis. Eye 1999; 13 (Part 3a): 345–347.
Reidy JJ, Paulus MP, Gona S . Recurrent erosions of the cornea: epidemiology and treatment. Cornea 2000; 19: 767–771.
Tabery HM . Corneal stromal infiltrates in patients with recurrent erosions. Acta Ophthalmol Scand 1998; 76: 589–592.
Rubinfeld RS, Laibson PR, Cohen EJ, Arentsen JJ, Eagle Jr RC . Anterior stromal puncture for recurrent erosion: further experience and new instrumentation. Ophthalmic Surg 1990; 21: 318–326.
Ionides AC, Tuft SJ, Ferguson VM, Matheson MM, Hykin PG . Corneal infiltration after recurrent corneal epithelial erosion. Br J Ophthalmol 1997; 81: 537–540.
Williams R, Buckley RJ . Pathogenesis and treatment of recurrent erosion. Br J Ophthalmol 1985; 69: 435–437.
Dua HS, Forrester JV . The corneoscleral limbus in human corneal epithelial wound healing. Am J Ophthalmol 1990; 110: 646–656.
Gipson IK . Adhesive mechanisms of the corneal epithelium. Acta Ophthalmol Suppl 1992; 202: 13–17.
Khodadoust AA, Silverstein AM, Kenyon DR, Dowling JE . Adhesion of regenerating corneal epithelium. The role of basement membrane. Am J Ophthalmol 1968; 65: 339–348.
Rodrigues MM, Fine BS, Laibson PR, Zimmerman LE . Disorders of the corneal epithelium. A clinicopathologic study of dot, geographic, and fingerprint patterns. Arch Ophthalmol 1974; 92: 475–482.
Brodrick JD, Dark AJ, Peace GW . Fingerprint dystrophy of the cornea. A histologic study. Arch Ophthalmol 1974; 92: 483–489.
Tripathi RC, Bron AJ . Ultrastructural study of non-traumatic recurrent corneal erosion. Br J Ophthalmol 1972; 56: 73–85.
Dahl MV, Ross AJ, Schlievert PM . Temperature regulates bacterial protein production: possible role in rosacea. J Am Acad Dermatol 2004; 50: 266–272.
Dougherty JM, McCulley JP . Bacterial lipases and chronic blepharitis. Invest Ophthalmol Vis Sci 1986; 27: 486–491.
Dougherty JM, McCulley JP . Analysis of the free fatty acid component of meibomian secretions in chronic blepharitis. Invest Ophthalmol Vis Sci 1986; 27: 52–56.
McCulley JP, Dougherty JM . Bacterial aspects of chronic blepharitis. Trans Ophthalmol Soc UK 1986; 105 (Part 3): 314–318.
Afonso AA, Sobrin L, Monroy DC, Selzer M, Lokeshwar B, Pflugfelder SC . Tear fluid gelatinase B activity correlates with IL-1alpha concentration and fluorescein clearance in ocular rosacea. Invest Ophthalmol Vis Sci 1999; 40: 2506–2512.
Jester JV, Petroll WM, Barry PA, Cavanagh HD . Expression of alpha-smooth muscle (alpha-SM) actin during corneal stromal wound healing. Invest Ophthalmol Vis Sci 1995; 36: 809–819.
Jester JV, Rodrigues MM, Herman IM . Characterization of avascular corneal wound healing fibroblasts. New insights into the myofibroblast. Am J Pathol 1987; 127: 140–148.
Fini ME, Girard MT, Matsubara M . Collagenolytic/gelatinolytic enzymes in corneal wound healing. Acta Ophthalmol Suppl 1992; 202: 26–33.
Fini ME, Cook JR, Mohan R . Proteolytic mechanisms in corneal ulceration and repair. Arch Dermatol Res 1998; 290 (Suppl): S12–S23.
Fini ME . Keratocyte and fibroblast phenotypes in the repairing cornea. Prog Retin Eye Res 1999; 18: 529–551.
Sivak JM, Fini ME . MMPs in the eye: emerging roles for matrix metalloproteinases in ocular physiology. Prog Retin Eye Res 2002; 21: 1–14.
Wong TT, Sethi C, Daniels JT, Limb GA, Murphy G, Khaw PT . Matrix metalloproteinases in disease and repair processes in the anterior segment. Surv Ophthalmol 2002; 47: 239–256.
Boudreau N, Bissell MJ . Extracellular matrix signaling: integration of form and function in normal and malignant cells. Curr Opin Cell Biol 1998; 10: 640–646.
Sivak J, Fini M . Pax-6 deficient mice show altered phenotype and gene expression during corneal re-epithelialization. ARVO Poster, Presentation Number: 41972002.
Mohan R, Chintala SK, Jung JC, Villar WV, McCabe F, Russo LA . Matrix metalloproteinase gelatinase B (MMP-9) coordinates and effects epithelial regeneration. J Biol Chem 2002; 277: 2065–2072.
Garrana RM, Zieske JD, Assouline M, Gipson IK . Matrix metalloproteinases in epithelia from human recurrent corneal erosion. Invest Ophthalmol Vis Sci 1999; 40: 1266–1270.
Goldman JN, Dohlman CH, Kravitt BA . The basement membrane of the human cornea in recurrent epithelial erosion syndrome. Trans Am Acad Ophthalmol Otolaryngol 1969; 73: 471–481.
Hersh PS, Rice BA, Baer JC, Wells PA, Lynch SE, McGuigan LJ et al. Topical nonsteroidal agents and corneal wound healing. Arch Ophthalmol 1990; 108: 577–583.
Mackie IA . Successful management of three consecutive cases of recurrent corneal erosion with botulinum toxin injections. Eye 2004; 18 (7): 734–737.
Hope-Ross MW, Chell PB, Kervick GN, McDonnell PJ, Jones HS . Oral tetracycline in the treatment of recurrent corneal erosions. Eye 1994; 8 (Part 4): 384–388.
Dursun D, Kim MC, Solomon A, Pflugfelder SC . Treatment of recalcitrant recurrent corneal erosions with inhibitors of matrix metalloproteinase-9, doxycycline and corticosteroids. Am J Ophthalmol 2001; 132: 8–13.
Matsubara M, Zieske JD, Fini ME . Mechanism of basement membrane dissolution preceding corneal ulceration. Invest Ophthalmol Vis Sci 1991; 32: 3221–3237.
Sobrin L, Ye HQ, Azar DT . Regulation of MMP-9 activity in human tear fluid and corneal epithelial culture supernatant. Invest Ophthalmol Vis Sci 2000; 41: 1703–1709.
Ye HQ, Azar DT . Expression of gelatinases A and B, and TIMPs 1 and 2 during corneal wound healing. Invest Ophthalmol Vis Sci 1998; 39: 913–921.
Solomon A, Rosenblatt M, Li DQ, Liu Z, Monroy D, Ji Z . Doxycycline inhibition of interleukin-1 in the corneal epithelium. Invest Ophthalmol Vis Sci 2000; 41: 2544–2557.
Fujikawa LS, Foster CS, Harrist TJ, Lanigan JM, Colvin RB . Fibronectin in healing rabbit corneal wounds. Lab Invest 1981; 45: 120–129.
Goto E, Shimmura S, Shimazaki J, Tsubota K . Treatment of superior limbic keratoconjunctivitis by application of autologous serum. Cornea 2001; 20: 807–810.
del Castillo JM, de la Casa JM, Sardina RC, Fernandez RM, Feijoo JG, Gomez AC . Treatment of recurrent corneal erosions using autologous serum. Cornea 2002; 21: 781–783.
Donnenfeld ED, Selkin BA, Perry HD, Moadel K, Selkin GT, Cohen AJ . Controlled evaluation of a bandage contact lens and a topical nonsteroidal anti-inflammatory drug in treating traumatic corneal abrasions. Ophthalmology 1995; 102: 979–984.
Poland DE, Kaufman HE . Clinical uses of collagen shields. J Cataract Refract Surg 1988; 14: 489–491.
Willoughby CE, Batterbury M, Kaye SB . Collagen corneal shields. Surv Ophthalmol 2002; 47: 174–182.
Mackie IA . Role of the corneal nerves in destructive disease of the cornea. Trans Ophthalmol Soc UK 1978; 98: 343–347.
Kent HD, Cohen EJ, Laibson PR, Arentsen JJ . Microbial keratitis and corneal ulceration associated with therapeutic soft contact lenses. Clao J 1990; 16: 49–52.
Sridhar MS, Rapuano CJ, Cosar CB, Cohen EJ, Laibson PR . Phototherapeutic keratectomy versus diamond burr polishing of Bowman's membrane in the treatment of recurrent corneal erosions associated with anterior basement membrane dystrophy. Ophthalmology 2002; 109: 674–679.
McLean EN, MacRae SM, Rich LF . Recurrent erosion. Treatment by anterior stromal puncture. Ophthalmology 1986; 93: 784–788.
Malecha MA . Anterior stromal puncture for recurrent corneal erosion after laser in situ keratomileusis. J Cataract Refract Surg 2004; 30: 496–498.
Katsev DA, Kincaid MC, Fouraker BD, Dresner MS, Schanzlin DJ . Recurrent corneal erosion: pathology of corneal puncture. Cornea 1991; 10: 418–423.
Geggel HS . Successful treatment of recurrent corneal erosion with Nd:YAG anterior stromal puncture. Am J Ophthalmol 1990; 110: 404–407.
Rubinfeld RS, MacRae SM, Laibson PR . Successful treatment of recurrent corneal erosion with Nd:YAG anterior stromal puncture. Am J Ophthalmol 1991; 111: 252–255.
Aitken DA, Beirouty ZA, Lee WR . Ultrastructural study of the corneal epithelium in the recurrent erosion syndrome. Br J Ophthalmol 1995; 79: 282–289.
Marshall J, Trokel SL, Rothery S, Krueger RR . Long-term healing of the central cornea after photorefractive keratectomy using an excimer laser. Ophthalmology 1988; 95: 1411–1421.
SundarRaj N, Geiss MJ, Fantes F, Hanna K, Anderson SC, Thompson KP . Healing of excimer laser ablated monkey corneas. An immunohistochemical evaluation. Arch Ophthalmol 1990; 108: 1604–1610.
Lohmann CP, Gartry DS, Muir MK, Timberlake GT, Fitzke FW, Marshall J . Corneal haze after excimer laser refractive surgery: objective measurements and functional implications. Eur J Ophthalmol 1991; 1: 173–180.
O'Brart DP, Muir MG, Marshall J . Phototherapeutic keratectomy for recurrent corneal erosions. Eye 1994; 8 (Part 4): 378–383.
Dausch D, Landesz M, Klein R, Schroder E . Phototherapeutic keratectomy in recurrent corneal epithelial erosion. Refract Corneal Surg 1993; 9: 419–424.
Ohman L, Fagerholm P, Tengroth B . Treatment of recurrent corneal erosions with the excimer laser. Acta Ophthalmol (Copenhagen) 1994; 72: 461–463.
Cavanaugh TB, Lind DM, Cutarelli PE, Mack RJ, Durrie DS, Hassanein KM . Phototherapeutic keratectomy for recurrent erosion syndrome in anterior basement membrane dystrophy. Ophthalmology 1999; 106: 971–976.
Jain S, Austin DJ . Phototherapeutic keratectomy for treatment of recurrent corneal erosion. J Cataract Refract Surg 1999; 25: 1610–1614.
Fagerholm P, Fitzsimmons TD, Orndahl M, Ohman L, Tengroth B . Phototherapeutic keratectomy: long-term results in 166 eyes. Refract Corneal Surg 1993; 9: S76–S81.
Maini R, Loughnan MS . Phototherapeutic keratectomy re-treatment for recurrent corneal erosion syndrome. Br J Ophthalmol 2002; 86: 270–272.
Soong HK, Farjo Q, Meyer RF, Sugar A . Diamond burr superficial keratectomy for recurrent corneal erosions. Br J Ophthalmol 2002; 86: 296–298.
Buxton JN, Fox ML . Superficial epithelial keratectomy in the treatment of epithelial basement membrane dystrophy. A preliminary report. Arch Ophthalmol 1983; 101: 392–395.
Harrison DA, Periman LM . Diffuse lamellar keratitis associated with recurrent corneal erosions after laser in situ keratomileusis. J Refract Surg 2001; 17: 463–465.
Ti SE, Tan DT . Recurrent corneal erosion after laser in situ keratomileusis. Cornea 2001; 20: 156–158.
Asano-Kato N, Toda I, Tsubota K . Severe late-onset recurrent epithelial erosion with diffuse lamellar keratitis after laser in situ keratomileusis. J Cataract Refract Surg 2003; 29: 2019–2021.
Hovanesian JA, Shah SS, Maloney RK . Symptoms of dry eye and recurrent erosion syndrome after refractive surgery. J Cataract Refract Surg 2001; 27: 577–584.
Jeng BH, Stewart JM, McLeod SD, Hwang DG . Relapsing diffuse lamellar keratitis after laser in situ keratomileusis associated with recurrent erosion syndrome. Arch Ophthalmol 2004; 122: 396–398.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ramamurthi, S., Rahman, M., Dutton, G. et al. Pathogenesis, clinical features and management of recurrent corneal erosions. Eye 20, 635–644 (2006). https://doi.org/10.1038/sj.eye.6702005
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702005
Keywords
This article is cited by
-
Efficacy of topical insulin for recurrent epithelial corneal erosions
Irish Journal of Medical Science (1971 -) (2023)
-
Diffuse lamellar keratitis as a rare complication of diamond burr superficial keratectomy for recurrent corneal erosion: a case report
BMC Ophthalmology (2022)
-
Anti-glaucoma agents-induced pseudodendritic keratitis presumed to be herpetic simplex keratitis: a clinical case series
Scientific Reports (2021)
-
Clinical evaluation of corneal changes after phacoemulsification in diabetic and non-diabetic cataract patients, a systematic review and meta-analysis
Scientific Reports (2017)
-
Putting on the brakes: Bacterial impediment of wound healing
Scientific Reports (2015)
