
Abstract
Data sources
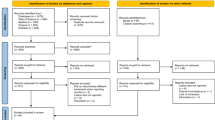
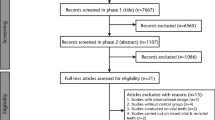
The authors searched the following electronic databases: the Cochrane Oral Health Trials Register, the Cochrane Central Register of Controlled Trials (CENTRAL), Medline Ovid and Embase Ovid. The US National Registry of Clinical Trials (ClinicalTrials.gov) and the World Health Organisation (WHO) International Clinical Trials Registry Platform were searched for ongoing trials. There were no restrictions regarding language and publication date. The authors hand-searched the reference lists of the studies retrieved and key journals in the field of endodontics.
Study selection
Randomised controlled trials (RCTs) involving people with periapical pathosis including comparison of surgical versus non-surgical treatment or different types of surgery. Outcome measures were healing of the periapical lesion assessed after one-year follow-up or longer, postoperative pain and discomfort and adverse effects such as tooth loss, mobility, soft tissue recession, abscess, infection, neurological damage or loss of root sealing material evaluated through radiographs.
Data extraction and synthesis
Two review authors independently extracted data from the included studies and assessed their risk of bias. Study authors were contacted to obtain missing information. The authors combined results of trials assessing comparable outcomes using the fixed-effect model, with risk ratios (RRs) for dichotomous outcomes and mean differences (MDs) for continuous outcomes, and 95% confidence intervals (CIs) and they used generic inverse variance for split-mouth studies.
Results
The review included 20 RCTs. Two trials at high risk of bias assessed surgery versus a non-surgical approach: root-end resection with root-end filling versus root canal retreatment. The other 18 trials evaluated different surgical protocols.
There was no clear evidence of superiority in the surgical or non-surgical approach for healing at one-year follow-up (RR 1.15, 95% CI 0.97 to 1.35; two RCTs, 126 participants) or at four- or ten-year follow-up (one RCT, 82 to 95 participants), although the evidence is very low quality. More participants in the surgically treated group reported pain in the first week after treatment (RR 3.34, 95% CI 2.05 to 5.43; one RCT, 87 participants; low quality evidence).
In terms of surgical protocols, there was some inconclusive evidence that ultrasonic devices for root-end preparation may improve healing one year after retreatment, when compared with the traditional bur (RR 1.14, 95%CI 1.00 to 1.30; one RCT, 290 participants; low quality evidence). There was evidence of better healing when root-ends were filled with MTA than when they were treated by smoothing of orthograde GP root filling, after one-year follow-up (RR 1.60, 95% CI 1.14 to 2.24; one RCT, 46 participants; low quality evidence).
There was no evidence that using CBCT rather than radiography for preoperative evaluation was advantageous for healing (RR 1.02, 95% CI 0.70 to 1.47; one RCT, 39 participants; very low quality evidence), nor that any magnification device affected healing more than any other (loupes versus endoscope at one year: RR 1.05, 95% CI 0.92 to 1.20; microscope versus endoscope at two years: RR 1.01, 95% CI 0.89 to 1.15; one RCT, 70 participants, low quality evidence). There was no evidence that antibiotic prophylaxis reduced incidence of postoperative infection (RR 0.49, 95% CI 0.09 to 2.64; one RCT, 250 participants; low quality evidence).
There was some evidence that using a papilla base incision (PBI) may be beneficial for preservation of the interdental papilla compared with complete papilla mobilisation (one RCT (split-mouth), 12 participants/24 sites; very low quality evidence). There was no evidence of less pain in the PBI group at day one post surgery (one RCT, 38 participants; very low quality evidence).
There was evidence that adjunctive use of a gel of plasma rich in growth factors reduced postoperative pain compared with no grafting (measured on visual analogue scale: one day postoperative MD -51.60 mm, 95% CI -63.43 to -39.77; one RCT, 36 participants; low quality evidence). There was no evidence that use of low energy level laser therapy (LLLT) prevented postoperative pain (very low quality evidence).
Conclusions
Available evidence does not provide clinicians with reliable guidelines for treating periapical lesions. Further research is necessary to understand the effects of surgical versus non-surgical approaches, as well as to determine which surgical procedures provide the best results for periapical lesion healing and postoperative quality of life. Future studies should use standardised techniques and success criteria, with precisely-defined outcomes and the participant as the unit of analysis.
Similar content being viewed by others

Commentary
Root canal treatment is still a treatment option to preserve teeth that have lost vitality for different reasons. Patients still prefer that option to retain their natural dentition when possible, instead of extraction and replacement of the problematic tooth.1,2
Failure rate for root canal treatment may have different and varied aetiology.
Anatomical complexity of the root canals, resilient microbes, operative procedural errors,3 type of chemo-mechanical instrumentation and obturation, methods and leakage of permanent restoration can all influence the success of the endodontic treatment.
There is great variability among practitioners in treatment planning teeth with questionable prognosis. The presence and the size of apical periodontitis is an important factor affecting the outcome of the root canal treatment and retreatment.4
At present, based on the results of the updated review, the evidence from non-surgical retreatment compared to surgical treatment is not robust enough to recommend one technique over the other. Postoperative pain needs to be considered in the surgical intervention. For the devices suggested, ultrasonic scalers or low energy laser therapy does not improve the outcome of postoperative pain or healing. The same outcome resulted for magnification devices. In regard to surgical technique, preserving the papilla seems to be beneficial. In assessing materials used for the technique, it seems that MTA is better and in some cases, using plasma rich in growth factors shows an improvement. Antibiotic prophylaxis did not seem to have an effect.
A review from Torabinejad and colleagues5 compared the clinical and radiographic outcomes of non-surgical retreatment with traditional surgical endodontic treatment. The results at two to four years for surgical endodontic treatment were a 78% success rate compared to 71% for non-surgical retreatment. The relationship reversed at four to six years, showing a higher success for non-surgical (83%) compared to surgical (72%). There are claims that newer techniques such as the use of microscopes, new root-end materials and microsurgery also improve the surgical technique but because of the limitations of the evidence the results should be considered with caution.
Endodontic therapy is a complex technique and multiple variables are associated with its success. It gets more complex when the survival of the tooth is affected by apical periodontitis. The decision of the retreatment, the surgical approach or the final extraction and replacement needs to be carefully considered by the practitioner and all risks and benefits of the proposed treatment discussed with the patient.
References
Iqbal M K, Kim S . A review of factors influencing treatment planning decisions of single-tooth implants versus preserving natural teeth with nonsurgical endodontic therapy. J Endod 2008; 34:519–529.
Lee C B, Chang Y H, Wen P C, Li C Y . Association of Failed Root Canal Treatment with Dentist and Institutional Volumes: A Population-based Cohort Study in Taiwan. J Endod 2017; pii: S0099-2399(17)30769-0. DOI: 10.1016/j.joen.2017.06.016.
Chércoles-Ruiz A, Sánchez-Torres A, Gay-Escoda C . Endodontics, Endodontic Retreatment, and Apical Surgery Versus Tooth Extraction and Implant Placement: A Systematic Review. J Endod 2017; 43: 679–686. DOI: 10.1016/j.joen.2017.01.004.
Torabinejad M, White SN . Endodontic treatment options after unsuccessful initial root canal treatment: Alternatives to single-tooth implants. J Am Dent Assoc 2016; 147:214–220.
Torabinejad M, Corr R, Handysides R, Shabahang S . Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod 2009; 35:930–937.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Luisa Fernandez Mauleffinch, Managing Editor, Cochrane Oral Health Group, School of Dentistry, The University of Manchester, JR Moore Building, Oxford Road, Manchester, M13 9PL, UK. E-mail: luisa.fernandez@manchester.ac.uk
Del Fabbro M, Corbella S, Sequeira-Byron P, Tsesis I, Rosen E, Lolato A, Taschieri S. Endodontic procedures for retreatment of periapical lesions. Cochrane Database Syst Rev 2016; 10: Art. No.: CD005511. DOI: 10.1002/14651858.CD005511.pub3
This paper is based on a Cochrane Review published in the Cochrane Library 2016, issue 10 (see www.thecochranelibrary.com for information). Cochrane Reviews are regularly updated as new evidence emerges and in response to feedback, and the Cochrane Library should be consulted for the most recent version of the review.
Rights and permissions
About this article

Cite this article
Ferrailo, D., Veitz-Keenan, A. No clinical quantifiable benefits between non-surgical and surgical endodontic treatment. Evid Based Dent 18, 75–76 (2017). https://doi.org/10.1038/sj.ebd.6401254
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6401254
This article is cited by
-
20 years - 20 highlights
Evidence-Based Dentistry (2019)
