
Abstract
Data sources
Medline, Embase, Cancerlit, Toxline were searched, followed by the reference lists of identified reviews and articles.
Study selection
Human cohort or case–control studies in peer-reviewed journals or that were publicly available were selected if they specified study location; examined any form of oral cancer as the outcome; and described use of chewing tobacco, orally used moist snuff or unspecified smokeless tobacco as the exposure. Studies in Asian populations and those with insufficient power where risk estimates and confidence intervals were not reported or could not be calculated were excluded.
Data extraction and synthesis
Standard information was abstracted from each study. Whole-population data were used to estimate numbers of never-smokers. Separate figures for males and females were obtained where possible. Estimates were made of effect size and precision since these were not presented in original studies. Separate meta-analyses were conducted for chewing tobacco, for snuff and for overall smokeless tobacco. Sensitivity analyses for smokers/ nonsmokers were carried out. Heterogeneity was investigated and publication bias assessed using a funnel plot.
Results
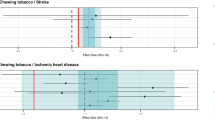
The 32 studies meeting the inclusion criteria provided 38 heterogeneous study-specific estimates of odds or relative risk ratios (see Tables 1, 2). An increase in risk was mainly evident in studies conducted before 1980. No increase was seen in studies in Scandinavia. The pattern of estimates suggests some publication bias.
Conclusions
Smokeless tobacco, as used in America or Europe, carries at most a minor increased risk of oral cancer, but elevated risks in specific populations or from specific products cannot definitely be excluded.
Similar content being viewed by others

Commentary
One has to wonder at the origin, purpose and motives of this research, purely on the basis that it was funded by Philip Morris international, the largest multinational tobacco company in the world. It had a global income of US$8.8 billion in 2007 with an increasing share of the international market.1 their website (www.philipmorrisinternational.com) also shows that they are involved in the production of both cigarette and smokeless tobacco products, and the primary mission of the company is the corporate interests of its shareholders.
Without doubting the scientific ethics of the individual authors, it is disappointing that such thoughts and doubts must arise while reading this paper. There is a well-documented, significant debate on whether tobacco industry-funded research or, as in this case, internal tobacco company research is ethical and whether it should be published in the scientific literature at all.2, 3 Philip Morris' companies and experts have a long history of involvement in this controversy.4, 5 On the plus side for this present study, the authors' conflicts of interest are up front, declared and not hidden.
The main conclusions of the paper are that smokeless tobacco products have “at most a minor increased risk of oral cancer”, and that there is no “direct effect of smokeless tobacco itself”. Despite claims in the paper of a more robust and inclusive approach, a number of methodological issues may not have been fully considered. There are no guidelines for undertaking meta-analyses of observational studies as there are for interventional studies (eg, Cochrane guidelines).6 nevertheless the meta-analysis of observational studies in epidemiology group7 provide a robust reporting framework for such studies. A number of key areas could have been given more attention to reduce the potential risks of bias in this meta-analysis, including:
-
A fully documented systematic search strategy (including wider database search and attempts to include published and unpublished data);
-
Documentation of data abstraction (including multiple assessors and blinding);
-
Quality assessment of the included studies and sensitivity analysis based on study quality.
-
Although reasonable attempts were made to adjust for the influence of confounding factors such as smoking and alcohol, this can only really be done with a pooled analysis of individual patient data (IPD). However this may not be possible as the original data may no longer available in the case of older studies.
-
Furthermore, the findings of this meta-analysis contradict a similar earlier analysis,8 which had excluded studies from India and other Eastern countries where processed tobacco is not comparable with that used in the west, and the review and conclusions of the world health organization international agency on research on cancer's (IARC),9 who maintain that:
-
“there is sufficient evidence in humans for the carcinogenicity of smokeless tobacco”;
-
“smokeless tobacco causes cancers of the oral cavity and pancreas”;
“there is sufficient evidence in experimental animals for the carcinogenicity of moist snuff”;
And conclude that smokeless tobacco is carcinogenic to humans.
As this new meta-analysis goes against IARC'S view, only contains two studies published since the Rodu review,8 (although it did include other earlier studies not considered by Rodu) and has a number of methodological issues in addition to my concerns about the origins and motives of the paper, I feel that it merely clouds rather than clarifies the question.
References
Mackay J, Eriksen M . The Tobacco Atlas. Geneva: World Health Organization; 2002.
King J, Yamey G, Smith R . For and Against: Why journals should not publish articles funded by the tobacco industry: for and against. Br Med j 2000; 321:1074.
Chapman S . Research from tobacco industry affiliated authors: need for particular vigilance. Tobacco Control 2005; 14:217–219.
Davey Smith G, Phillips A . Passive smoking and health: should we believe Philip Morris's “experts”? Br Med J 1996; 313:929–933.
Ong EK, Glantz SA . Constructing “sound science” and “good epidemiology”: tobacco, lawyers, and public relations firms. Am J Public Health 2001; 91:1749–1757.
Higgins JPT, Green S (eds). Cochrane handbook for systematic reviews of interventions version 4.2.6. The Cochrane Collaboration 2006.
Stroup D, Berlin J, Morton S, et al. Meta-analysis of observational studies in epidemiology: proposal for reporting. J Am Med Assoc 2000; 283:2008–2012.
Rodu B, Cole p . Smokeless tobacco use and cancer of the upper respiratory tract. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002; 93:511–515.
International Agency on Research on Cancer. IARC monographs on the evaluation of carcinogenic risks to humans. Volume 89. Smokeless tobacco and some tobacco-specific n-nitrosamines Lyon: IARC; 2007.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Rolf Weitkunat, Philip Morris International, research and development, Philip Morris products SA, Neuchâtel, Switzerland. E-mail: rolf.weitkunat@pmintl.com
Weitkunat R, Sanders E, Lee PN. Analysis of the relation between European and American smokeless tobacco and oral cancer. BMC Publ Health 2007; 7:334
Rights and permissions
About this article
Cite this article
Conway, D. Oral cancer risk and smokeless tobacco products – clouded by smoke?. Evid Based Dent 9, 114–115 (2008). https://doi.org/10.1038/sj.ebd.6400615
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400615
