
Abstract
Data sources
Studies were searched for in the Cochrane Oral Health Group Trials Register (up to 15 September 2005), the Cochrane Central Register of Controlled Trials (Cochrane Library 2005, issue 3), Medline (from 1966 up to September 2005, and Embase (1974 to September 2005.
Study selection
Only randomised controlled trials (RCT) were included that compared different methods of tongue cleaning to reduce mouth odour in adults who had halitosis. Selected studies were graded independently for quality of randomisation, allocation concealment, blinding of outcomes assessment, and handling of losses and withdrawals.
Data extraction and synthesis
Data were extracted independently by two review authors; clinical heterogeneity precluded pooling of data.
Results
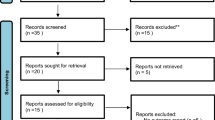
Two trials involving a total of 40 participants were included. Neither trial included data for the primary outcomes specified in this review, ie, self expressed (perceived) and organoleptic (human nose) assessments of halitosis using any validated malodour intensity scale. Secondary outcomes, volatile sulphur compound (VSC) levels, were assessed using a portable sulphide monitor in both trials. Based on the independent data from these two trials, there was a statistically significant difference between the effectiveness of either the tongue cleaner or the tongue scraper in reducing VSC levels when compared with the toothbrush. Adverse effects in one trial were nausea (60%) and trauma (10%) with the toothbrush and all participants were receptive to using the tongue scraper.
Conclusions
There is weak and unreliable evidence suggesting a small but statistically significant difference in reduction of VSC levels when tongue scrapers or cleaners rather than toothbrushes are used to reduce halitosis in adults. We found no high-level evidence comparing mechanical with other forms of tongue cleaning.
Similar content being viewed by others

Commentary
In the majority of cases, halitosis is caused by bacterial putrefaction in the oral cavity which leads to the production of odoriferous metabolites such as VSC. Data from interdisciplinary bad breath consultations indicate that the main source of odour production is most frequently located on the dorsum of the tongue.1, 2–3 Regular mechanical tongue cleaning and other measures attempting to reduce the bacterial load on the tongue are thus considered to be the basic treatment regimes.4
The objective of the present review was to provide reliable evidence regarding the effects of mechanical tongue cleaning versus other interventions such as mouthwashes, an aim that therefore seems appropriate and highly eligible. The results of this investigation are somewhat disappointing, however, and are simply not sufficient to achieve the objective. Only two studies were included in the analysis, neither of which compared tongue cleaning with other interventions. This finding clearly shows that well-designed research is still needed in this field.
Future studies, namely RCT, should not only focus on larger samples and longer interventions and follow-up periods, but also on complex treatment protocols. The management of oral halitosis is not as simple as merely handing out a mouthwash and a tongue cleaner: interventions such as training in oral (interdental) hygiene and professional toothcleaning can also lead to a significant decrease of oral VSC levels without any mechanical tongue cleaning.5 Other potential effects and side-effects of tongue cleaning, such as any reduction in specific microbes (eg, Streptococcus mutans), might also usefully be addressed.6
A major problem for clinical investigations is comparing the severity of subjects' oral malodour between different trials. Results from studies that include individuals who have only slight forms or experimental oral malodour, triggered by refraining from oral hygiene, might be used to combat morning breath, but these may be of little help to patients who have chronic, severe forms of halitosis.
Finally, the main question to be addressed in future research should be how to prevent the development of odour-producing biofilms, instead of mechanically or chemically combating existing biofilms.7 In other words, what is the specific ecological force within the oral microbial community that tips the balance towards odour production? Is it simply a lack of oral hygiene or do, for example, variations in saliva play a major role?8
Practice point
The outcome of the present review is limited in terms of recommending a rationale for the treatment of oral halitosis, besides the fact that a toothbrush might be less suitable for cleaning the tongue than a device specially designed to do so.
References
Delanghe G, Ghyselen J, Feenstra L, Van Streenberg D . Experience of a Belgian multidisciplinary breath odour clinic. In Bad Breath. A Multidisciplinary Approach. Edited by D van Steenberghe, M Rosenberg. Leuven: Leuven University Press; 1996, pp199–209.
Rosenberg M . Experiences of an Israeli malodour clinic. In Bad Breath. Research Perspectives. Edited by M Rosenberg. Tel Aviv: Ramot Publishers; 1997, pp 137–149.
Seemann R, Bizhang M, Djamchidi C, Kage A, Nachnani S . The proportion of pseudo-halitosis patients in a multidisciplinary breath malodour consultation. Int Dent J 2006; 56:77–81.
Yaegaki K, Coil JM, Kamemizu T, Miyazaki H . Tongue brushing and mouth rinsing as basic treatment measures for halitosis. Int Dent J 2002; 52 (suppl. 3):S192–S196.
Seemann R, Passek G, Zimmer S, Roulet JF . The effect of an oral hygiene program on oral levels of volatile sulfur compounds (VSC). J Clin Dent 2001; 12:104–107.
Quirynen M, Avontroodt P, Soers C, Zhao H, Pauwels M, van Steenberghe D . Impact of tongue cleansers on microbial load and taste. J Clin Periodontol 2004; 31:506–510.
Roldan S, Herrera D, Sanz M . Biofilms and the tongue: therapeutical approaches for the control of halitosis. Clin Oral Invest 2003; 7:189–197.
Hinode D, Fukui M, Yokoyama N, Yokoyama M, Yoshioka M, Nakamura R . Relationship between tongue coating and secretory-immunoglobulin A level in saliva obtained from patients complaining of oral malodor. J Clin Periodontol 2003; 30:1017–1023.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Luisa M Fernandez Mauleffinch, Cochrane Oral Health Group, MANDEC, School of Dentistry, University of Manchester, Higher Cambridge Street, Manchester M15 6FH, UK.
Outhouse TL, Al-Alawi R, Fedorowicz Z, Keenan JV. Tongue scraping for treating halitosis. Cochrane Database of Systematic Reviews 2006, issue 2
Rights and permissions
About this article
Cite this article
Seemann, R. Tongue scrapers may reduce halitosis in adults. Evid Based Dent 7, 78 (2006). https://doi.org/10.1038/sj.ebd.6400433
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400433
