
Key Points
-
An investigation of morbidity experienced by patients following iliac crest graft procedures for augmentation of the maxilla or mandible.
-
When treatment options are being discussed with a patient, it is important for the GDP and specialist to fully inform the patient of the possible morbidities that can be experienced at the donor site.
-
This paper provides important information for GDPs and other specialists who may be considering referral of patients for such treatment.
Abstract
Objective A study which examined the morbidity experienced by patients who underwent iliac crest bone graft procedures.
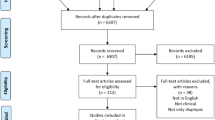
Design A post-operative questionnaire was forwarded to patients who underwent iliac crest bone graft procedures at a single centre.
Subjects One hundred and fourteen patients underwent iliac crest bone grafts for intra-oral augmentation.
Results Ninety-eight patients (80%) returned post-operative questionnaires. Eighty of the 98 (81.6%) patients suffered post-operative pain with 70% of patients being pain-free after four weeks. However, 10% of patients experienced pain for more than 16 weeks. Eighty-five (86.7%) patients were able to walk without any difficulties six weeks post-operatively. Gait disturbance was not related with age, however there was a significant association between pain and disturbance of gait (P< 0.001). Twenty two patients required the use of a walking stick and the use of such aids varied from 0.5 to 26 weeks. Women used walking aids for longer periods than men (P< 0.05). Twenty five patients had altered sensation with about half of them experiencing altered sensation in the distribution of the lateral femoral cutaneous nerve. Other morbidities included deformity at the hip site (2.4%), haematoma (2.4%), infection (3.2%), stress fracture (4.1%) and meralgia paraesthetica in one patient. Despite the above morbidities, 82 patients were willing to undergo the same procedure again and 89 patients would recommend the procedure to their relatives and friends.
Conclusion This study demonstrates considerable morbidity following anterior iliac crest bone harvest for intra-oral augmentation. Clinicians referring patients for such bone graft procedures must be aware of the above morbidities so that any patients referred for such procedures are fully informed.
Similar content being viewed by others

Main
Teeth are usually lost as a result of disease or trauma but some patients may have congenitally missing teeth. One of the key elements involved in successful prosthetic rehabilitation is the remaining volume and contour of alveolar bone and covering mucosa.1 Following a dental extraction, the residual alveolar bone undergoes a period of accelerated resorption for about 10 weeks followed by slower resorption. Atwood in 1971 proposed that residual ridge resorption is a multifactorial disease, which includes anatomic, biologic and mechanical factors which all co-operate in resorption. Anatomical reasons include the size and shape of the ridge, the type of bone and mucoperiosteum, and metabolic reasons including age, sex, hormonal balance and osteoporosis. Mechanical factors include the forces applied to the ridge, the type of denture base and the interocclusal distance. Decreased physical activity, diet, race and hereditary causes may also play a role in age related bone loss.3 Therefore, following tooth loss, patients may require prosthetic rehabilitation or dental implants. Patients increasingly demand implant therapy. Successful treatment of such patients depends on sufficient alveolar bone volume. The use of autogenous corticocancellous block grafts for augmentation of compromised alveolar volume has become a well established and accepted technique with studies reporting high graft success and subsequent osseointegration for implants placed into these grafted sites. The three main indications for bone grafting are inadequate ridge width, inadequate ridge height and improper ridge trajectory.4 However, augmentation of narrow ridges with autogenous grafts carries considerable morbidity.
Compromised alveolar volume may be augmented by use of several methods:
-
Alloplastic materials such as hydroxyapatite, tricalcium phosphate
-
Allografts such as frozen, freeze-dried or demineralised freeze-dried bone, such as deproteinised bovine bone (BioOss — Geistlich)
-
Homografts such as demineralised freeze-dried bone from a bone bank
-
Autogenous bone grafts such as from the iliac crest, tibia, rib, mandible or calvarium
-
Distraction osteogenesis.
A graft harvested from the ilium provides a large number of pluripotent or osteogenic precursor cells in particulate cancellous bone and in the marrow portion of the graft. It is considered the gold standard for graft material.5 The ilium has two great reservoirs of cancellous bone at the anterior and posterior ilium. Consequently, two different approaches have been suggested to harvest bone. At the posterior ilium there is more bone available and the morbidity is minimal.6 However, the main disadvantage is that it adds two hours to surgery time because simultaneous ilium and facial surgery cannot be accomplished and it also risks the position of the endotracheal tube during repositioning of the patient on the operating table. In 1993 Marx suggested that this technique should only be used if 50 cc or more of cancellous bone graft material is required and the preferred donor site for intra-oral augmentation is the anterior ilium.7
Iliac crest graft harvesting is performed under general anaesthesia. The iliac crest is palpated as the site of harvest is between the anterior superior iliac spine (ASIS) and the tubercle of the crest some 5 cm posterior to the ASIS. Here the ilium is at its greatest medio-lateral width and facilitates cancellous bone harvest.
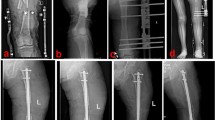
Donor site morbidity still remains a major problem (Fig. 1). The most frequent complication is pain,8 other complications include sensory disturbance,7 gait disturbance,1,10 infection,11 meralgia paraesthetica,12 adynamic ileus,13 contour deformity,11 fracture of the iliac crest11,14 and unsightly scaring.9

Donor site morbidity/complications
The aims of the study were:
-
To examine the post-operative morbidity experienced by patients who had harvest of bone from the iliac crest for intra-oral augmentation.
-
To establish types of complications at the donor site.
-
To establish if these patients would have the same operation again.
Method
Approval of the Trust Ethical Committee was obtained together with written informed consent from patients. One hundred and fourteen patients who had undergone anterior iliac crest graft harvesting completed a questionnaire 12 months after surgery to establish post-operative morbidity (Fig. 2). Autogenous bone was harvested by consultants and experienced specialist registrars from the medial aspect of the anterior ilium. Patient data was collected during a seven-year period (1994 to 2001).

Patient questionnaire
Results
One hundred and fourteen patients underwent iliac crest bone graft procedures. One hundred and twenty three iliac crest bone harvests were performed of which nine patients had graft harvest on two separate occasions. Ninety-eight (80%) questionnaires were returned. The patients were aged from 16–75 (median 44 years), with a female/male ratio of 1.6:1. There were two peaks in age distribution with one peak at age 25 which contained patients with congenitally missing teeth or teeth loss due to trauma and the second peak was at 45–50 age group and related to patients who were edentulous. Each question posed is presented in an abbreviated form with the results as follows:
Question 1 — Did you experience pain at the hip donor site?
Eighty patients suffered post-operative pain with 18 patients reporting no pain (Fig. 3). When assessing the experience of pain according to gender, there was no difference between males (81%) and females (82%).

Presence/absence of pain following iliac crest graft harvest
Question 2 — For how long did you experience pain at the hip donor site?
Figure 4 shows the duration of post-operative pain at the ilium may last up to 16 weeks. However, 70% of patients were pain-free after 4 weeks, with 10% of patients experiencing pain for more than 16 weeks.

Duration of post-operative pain at the ilium
Question 3 — On this scale of 0-100 place a mark to indicate the worst pain that you experienced at the hip donor site.
A visual analogue scale was used to assess the worst pain patients experienced at the donor site. Figure 5 shows the quantity of pain experienced by patients. The median value for worst pain was 39.6. A Mann-Whitney U test confirmed that women (mean rank 51) did not report more pain than men (mean rank 47).

Measurement of worst post-operative pain
Question 4 — For how long after surgery did you have problems with walking ?
Eighty-five (86.7%) of patients were able to walk without any difficulties 6 weeks post-operatively (Fig. 6). However, of the five patients who suffered with disturbance of gait for more than 14 weeks, four had a single iliac graft harvest and one patient had bilateral iliac crest graft harvest on two separate occasions. Although, age did not correlate with problems with gait, there was a significant association between pain and disturbance of gait (P<0.001) indicating that patients who experienced more pain had greater problems with walking.

Duration of problems with gait
Question 5 — Did you need to use a walking stick, crutch or wheelchair after your hip operation. If yes, for how long?
Twenty-two (22.4%) patients required the use of a walking stick. One patient with a fracture at the iliac crest required a wheelchair. The duration of use of such aids was from 0.5 to 26 weeks. There was a significant difference (P<0.05) between the sexes as women used walking aids for longer periods than men.
Question 6 and 7 — Was there any numbness in the hip or leg. If so, where?
Twenty-five patients reported numbness with 11 patients experiencing numbness of the outside of the thigh, nine on top of the thigh, eight inside of the thigh and three patients had larger areas of sensory loss.
Question 8 — Please could you specify if you experienced any other complications as listed?
Three (2.4%) patients developed a haematoma at the operation site. Haematomas usually develop when a drain is not placed intra-operatively. A drain was placed for 110 out of 117 procedures. In seven procedures, drains were not inserted and two out of the three haematomas occurred in this patient group (P<0.01). For six patients, this information was not available. Four (3.2%) patients suffered with infection at the donor site, of which three cases had a superficial infection whilst a fourth patient developed a deep infection. These were treated conservatively with a course of antibiotics. Five (4.1%) patients had post-operative stress fractures in the area of graft harvest. All five patients were female and a significant number of patients were in the older rather than younger age group (P<0.01). All of the patients were treated conservatively with bed rest and physiotherapy. Three of the patients walked with the aid of a walking stick, one used crutches and the other patient was wheelchair bound for five months. This patient also suffered with a tingling and burning sensation in the distribution of the lateral femoral cutaneous nerve known as meralgia paraesthetica. A 60-year-old male recorded the following: 'when the weather is cold, the scar feels tender', and a 32-year-old female reported: 'in cold weather and when flying for over five hours the hip area on the right hand side aches and on a scale of 0-100, the ache is 70'. In both cases, a clinical diagnosis of meteorotropism was made. Three (2.4%) patients reported deformity at the hip site, which was confirmed clinically on post-operative review.
Question 9 — Were you satisfied with your scar ?
Patients rated their satisfaction with the residual scar using a visual analogue scale (Fig. 7). Fifty-nine (60%) patients were very satisfied with their scar and there was no statistical difference between male and females. However, a significant number of younger patients were dissatisfied with the appearance of their scar compared with older patients (P<0.001).

Scar satisfaction
Question 10 — Would patients be willing to undergo the same operation again at the hip donor site ?
Eighty-two (85.6%) patients were willing to undergo an iliac crest bone graft procedure again. However, 14 patients were not willing to have the procedure repeated and two patients did not respond to the question.
Question 11 — Would you recommend this surgery to friends and colleagues ?
Eighty-nine (91.8%) patients would recommend iliac crest grafting to their relatives and friends whereas 8 (8.2%) patients would not. One patient did not respond to this question.
Discussion
In the current study, harvesting from the inner table of the anterior iliac crest provided sufficient quantities of bone for alveolar augmentation for all patients. The advantages of this donor site include easy accessibility, a high ratio of cancellous to cortical bone and a high concentration of osteoblasts, which induce additional bone growth at the recipient site.7,15 Bone harvest from this site, however, has the disadvantage of the need for a separate donor site with its inherent morbidity. The complications of the anterior iliac approach include prolonged post-operative pain,16,17,18 altered gait,10,19 sensory nerve damage,17,18 poor scar placement and altered bone contour,18 delayed healing,18 herniation of abdominal contents,11 clicking during walking,18 ilium fracture,20 peritonitis,6 excessive blood loss18 and rarely retroperitoneal haematoma.21
The precise cause of donor site pain remains obscure. Some patients experience no pain whilst 10% experienced considerable pain for up to 16 weeks. The findings here concur with previous observations of patients suffering pain at 6 months after surgery.8 It is postulated that this is either muscular or periosteal, secondary to the stripping of abductors from the ilium or neurogenic secondary to sensory nerve injury. In order to overcome the problem of pain at the wound site, several technical modifications have been suggested8,11,25,26,27 and furthermore, the use of Bupivicaine for post-operative pain relief.30 Other modifications include, placement of a vertical or oblique skin incision to avoid cutting cutaneous nerves, incisions greater than or equal to 3 cm dorsal to the anterior superior iliac spine and sub-periosteal dissection with careful haemostasis.11,15,31,32 It has been suggested that incisions directly over the crest are avoided as this increases the incidence of delayed healing.18 However, the use of medially and crestally placed incisions also increases the risk of damage to the lateral cutaneous nerve of the thigh. Paraesthesia of the anterior thigh also occurs when the lateral femoral cutaneous nerve is injured. The incidence of altered sensation in the distribution of the latter nerve is 11.2% in our series compared with the reported range of 1.3–37%.8,11,22,23,24,25,26,27,28 Variations in the position of the lateral femoral cutaneous nerve may be a contributing factor associated with injury of that nerve.29
Gait disturbance after bone harvesting from the inner table is a minimal and temporary inconvenience.6,7,10,17,18,27 This may also be related to pain and was present for greater than 14 weeks in the five patients who developed post-operative stress fractures. Three patients reported deformity at the donor site and this has been reported on previously.18 Donor site deformity can be minimised by repositioning of the osteoplastic flap and suturing with a strong resorbable suture.22 Three patients (2.4%) developed a haematoma at the operation site. Haematoma formation results from inadequate intra-operative haemostasis, improper sub-periosteal dissection or cancellous bone bleeding.11 Haematoma formation can be reduced by use of sheets of absorbable haemostatic sponge at the end of surgery as well as expeditious removal of surrounding cancellous bone marrow.15 Placement of a drain into the site of surgery may also prevent haematoma formation.24 None of the patients in this study developed a seroma. Post-operative deep infections requiring surgical intervention have been reported to have occurred in less than 1% of cases.11 Infection usually results from improper technique particularly in immuno-compromised or nutritionally depleted hosts. Treatment of deep post-operative infections requires incision and drainage, irrigation, debridement and a course of culture-directed intravenous and oral antibiotics.11 The one patient in this study who developed such an infection was treated with antibiotic therapy.
Stress fractures at the iliac crest have been reported previously14,33 and this possibly may be caused by the anterior iliac crest bone graft being harvested too close to the anterior superior iliac spine thereby pre-disposing the patient to a fracture of the anterior superior iliac spine from the iliac wing. Five patients experienced stress fractures several weeks after harvest of the iliac crest graft. Three of these patients had falls post-operatively which may have contributed to their stress fracture. Radiographic examination confirmed that the fractures in all patients were undisplaced and therefore treated conservatively. We also examined scar satisfaction with 60% of patients reporting satisfaction. A significant number of younger patients were dissatisfied with the appearance of their scar. Tension-free skin closure along with meticulous multiple layer closure so that the skin edges sit in approximation or near approximation before sub-cuticular closure of the skin is important. Despite the above morbidities, 85.6% were willing to undergo the procedure again with 91.8% of patients reporting that they would recommend the procedure to relatives and friends. The rates of satisfaction after harvest of anterior iliac crest bone grafts have been reported between 82% and 86.1%.9,34
Conclusion
This study demonstrates considerable morbidity following anterior iliac bone harvest for intra-oral augmentation. In order to reduce morbidity, it is not only important to have a thorough understanding of the osseous anatomy of the anterior ilium and its muscular attachments, but also good surgical procedure. Although bone graft substitutes are available, their use for large areas of resorbed alveolar bone has not been proven and clinicians referring patients for bone graft technique must be aware of the above morbidities.
References
Wyatt CL . The effect of prosthodontic treatment on alveolar bone loss: a review of the literature. J Prosth Dent 1998; 80: 362–366.
Atwood DA . Reduction of residual ridges: a major oral disease entity. J Prosth Dent 1971; 26: 266–277.
Krolner P, Toft P . Vertebral bone loss: an unheeded site effect, therapeutic bed rest. Clin Sci 1983; 64: 537–540.
Rissolo AR, Bennet J . Bone grafting and its essential role in implant dentistry. Dent Clin North Am 1998; 42: 91–116.
Buchardt H . Biology of bone transplantation. Ortho Clin N Am 1987; 18: 187–196.
Marx RE, Morales MJ . Morbidity from bone harvest in major jaw reconstruction: a randomised controlled trial comparing the lateral anterior and posterior approaches to the ilium. J Oral Maxillofac Surg 1988; 48: 196–203.
Marx RE . Philosophy and particulars of autogenous bone grafting. J Oral Maxillofac Clin North Am 1993; 5: 599–612.
Goulet JA, Senunas LE, DeSilva GL, Greenfield ML . Autogenous iliac crest bone graft. Complications and functional assessment. Clin Orthop Rel Res 1997; 339: 76–81.
Schnee CL, Freese A, Weil RJ, Marcotte PJ . Analysis of harvest morbidity and radiographic outcome using autograft for anterior cervical fusion. Spine 1997; 22: 2222–2227.
Crockford DA, Converse JN . The ilium as a source of bone grafts in children. Plast Reconstr Surg 1972; 50: 270–274.
Kurz LT, Garfin SR, Booth RE . Iliac bone grafting. Techniques and complications of harvesting. In Garfin. S R (ed). Complications of spine surgery. Baltimore, Williams and Wilkins, 1989; pp323–341.
Weikel AM, Habal NB . Meralgia paraesthetica: a complication of iliac bone graft. Plast Reconstr Surg 1977; 60: 572–574.
James JD, Gross BD, Jeist ET . Adynamic ilius as a complication of iliac bone graft. J Oral Surg 1981; 39: 289–291.
Guha SC, Poole MD . Stress fracture of the iliac bone with sub-fascial femoral neuropathy; an unusual complication at a bone graft donor site: case report. Br J Plast Surg 1983; 36: 305–306.
Tayapongsak P, Wimsatt JA, LaBlanc JP, Dolwick MF . Morbidity from anterior ilium bone harvest. A comparative study of lateral versus medial surgical approach. Oral Surg Oral Med Oral Pathol 1994; 78: 296–300.
Cohen M, Figueroa AA, Haviv Y, Schafer ME, Aduss H . Iliac versus cranial bone for secondary grafting of residual alveolar clefts. Plast Reconstr Surg 1991; 87: 423–429.
Grillon GL, Gunther SF, Connole PW . A new technique for obtaining iliac bone grafts. J Oral Maxillofac Surg 1984; 42: 172–176.
Laurie SWS, Karan LB, Mulliken JB, Murray JB . Donor site morbidity after harvesting rib and iliac bone. Plast Reconstr Surg 1984; 73: 933–938.
Mrazik J, Amato C, Leban S, Mashberg A . The ilum as a source of autogenous bone for grafting: clinical considerations. J Oral Surg 1980; 38: 29–32.
Rosenstein S, Vado DV, Kernahan D, Griffith BH, Grasseschi M . The case for early bone grafting in cleft lip and palate. Plast Reconstr Surg 1991; 87: 644–654.
Sindet-Peterson S, Enemark H . Mandibular bone grafts for reconstruction of alveolar clefts. J Oral Maxillofac Surg 1988; 46: 533–537.
Beirne JC, Barry HJ, Brady FA, Morris VB . Donor site morbidity of the anterior iliac crest following cancellous bone harvest. Int J Oral Maxillofac Surg 1996; 25: 268–271.
Canady JW, Zeitler DP, Thompson SA, Nicholas CK . Suitability of the iliac crest as a site for harvest of autogenous bone graft. Cleft Palate J 1993; 30: 579–581.
Younger EM, Chapman MW . Morbidity at bone graft donor sites. J Orthop Trauma 1989; 3: 192–195.
Fowler BL, Dall BE, Rowe DE . Complications associated with harvesting autogenous iliac bone graft. Am J Orthop 1995; 24: 895–903.
Arrington ED, Smith WJ, chambers HG, Bucknel AL, Davino NA . Complications of iliac crest bone graft harvesting. Clin Orthop 1996; 329: 300–309.
Keller EE, Triplett WW . Iliac bone graft: review of 160 consecutive cases. J Oral Maxillofac Surg 1987; 45: 11–14.
Colterjohn NR, Bednar DA . Procurement of bone graft from the iliac crest. An operative approach with decreased morbidity. J Bone Joint Surg Am 1997; 79: 756–759.
Murata Y, Takahashi K, Yamagata M, Shimada Y, Morya H . The anatomy of the lateral femoral cutaneous nerve with special reference to the harvesting of iliac bone graft. J Bone Joint Surg Am 2000; 82: 746–747.
Puri R, Moskovich R, Gusmorino P, Shott S . Bupivicaine for post-operative pain relief at the iliac crest bone graft harvest site. Am J Orthop 2000; 29: 443–446.
Burstein FD, Simms C, Cohen SR, Work F, Paschal M . Iliac crest bone graft harvesting techniques: a comparison. Plast Reconstr Surg 2000; 105: 34–39.
Tanishima T, Yoshimasu N, Ogai M . A technique for prevention of donor site pain associated with harvesting iliac bone grafts. Surg Neurol 1995; 44: 131–132.
Reynolds Jnr A F, Turner P T, Loeser J D . Fracture of the anterior superior iliac spine following anterior cervical fusion using iliac crest. J Neuro Surg 1978; 48: 809–810.
Kalk WW, Raghoebar GM, Jansma J, Boering G . Morbidity from iliac crest bone harvesting. J Oral Maxillofac Surg 1996; 54: 1424–1429; discussion 1430.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Joshi, A., Kostakis, G. An investigation of post-operative morbidity following iliac crest graft harvesting. Br Dent J 196, 167–171 (2004). https://doi.org/10.1038/sj.bdj.4810945
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4810945
This article is cited by
-
Radiographic Assessment of Different Autogenous Bone Grafts in the Alveolar Cleft: A Retrospective Longitudinal Study
Journal of Maxillofacial and Oral Surgery (2023)
-
The performance of two-implant overdentures in the atrophic maxilla: a case series with 1-year follow-up
International Journal of Implant Dentistry (2022)
-
Surgical and prosthetic rehabilitation of siblings with Witkop tooth and nail syndrome using zygomatic implants: a familial case series of 3 patients with up to 15-year follow-up
Oral and Maxillofacial Surgery (2022)
-
Patient experience following iliac crest-derived alveolar bone grafting and implant placement
International Journal of Implant Dentistry (2020)
-
Cancellous allogenic and autologous bone grafting ensure comparable tunnel filling results in two-staged revision ACL surgery
Archives of Orthopaedic and Trauma Surgery (2020)
