
Abstract
Objective To assess the educational effectiveness of delivering continuing professional education (CPE) from dental schools to small groups of dentists at distant sites via videoconferenced links using relatively inexpensive equipment and ISDN2 links.
Design 41 videoconferences between the four campuses of London Dental Schools and postgraduate centres in South East England were assessed using a pre-piloted questionnaire which contained open and specific questions. The questionnaire was given to all participants at the end of each videoconference. Answers to the specific questions were graded using the Likert scale.
Results 40 of the 41 videoconferences were completed satisfactorily and were attended by 257 participants, all of whom completed questionnaires. However, no individual question was answered by all the participants. Of the responses 90% were positive on the topics of appropriateness of the teaching material for delivery by videoconference and of its educational level. 90% of responses also indicated a wish to attend further videoconferences and satisfaction at avoiding the need to travel to London for similar educational activity. 87% rated the lecturers as good or excellent in their use of the medium. 85% of responses indicated that the question and answer sessions within the videoconferences were useful and 82% that the visual aids enhanced the sessions. The technical aspects of the videoconferences were rated positively but to a lesser extent than the educational aspects with 69% of positive responses for visibility of visual aids, 54% for sound quality and 76% for the lecturers use of the technology. The technical aspects of the videoconferences improved during the pilot study. In response to the open questions, participants stated that they found the most useful aspects of the videoconferences were not having to travel, access to first rate lecturers, the discussions and the opportunity to interact with experts.
Conclusions The participants in this pilot study were positive about the use of videoconferencing to deliver educational material from dental schools to small groups. Once the technology has improved, this medium has the potential to provide CPE for dentists at work or at home in response to their specific needs.
Similar content being viewed by others

Main
In 1989 a large national survey1 indicated that 30% of UK dentists had attended either no courses or lectures to update their professional knowledge or only one such course/lecture. The same survey investigated reasons why these dentists had not undertaken continuing professional development (CPD) during the previous 12 months.
Four of the most commonly cited reasons for non-attendance, such as distance from postgraduate centres and domestic commitments, suggested that these problems could be overcome by the provision of distance learning materials and programmes. To address the problems a range of videos,2 manuals3,4 and computer-aided learning programmes5 have been developed at public expense6 and distributed free of charge to dentists working in Primary Dental Care within the NHS. A more recent study7 indicates that in one English region during the 1990s there has been an improvement in the numbers of dentists attending CPD courses. A further stimulus to CPD has arisen from the General Dental Council's (GDC's) recently launched voluntary scheme8 which requires a UK registered dentist to take part in CPD throughout his or her practising career. This has further encouraged the development and evaluation of additional techniques for the provision of CPD for dentists, one of which is videoconferencing, a technique which allows two way audio and video communication between remote sites.
Videoconferencing has been used to provide 'expert' opinions and advice to remote sites in a range of medical specialties9 and other areas of healthcare.10 In dentistry the technique has been used in the UK in the provision of orthodontic diagnosis and education,11,12 to improve dentist-laboratory communication and to provide consultant restorative dentistry support to remote dental practices13.
The primary benefit of videoconferencing is that it overcomes the problems caused by distance and geographical inaccessibility whilst permitting a 'realtime' interaction between those taking part. These problems may not be synonymous as travelling time can be affected by traffic congestion and poor roads as much as by geographical distance. To an extent the problem of unnecessarily long travelling times for relatively short journeys appertains in and around London and other large cities. The problem exists for both speakers and audience, as with 'conventional' attendance courses, either one or sometimes both parties have to travel to take part. Videoconferencing and other distance learning may well provide an alternative means of delivery for courses which do not require the audience to take part in practical exercises (hands-on courses).
Against this background, the Thames Postgraduate Medical and Dental Education (TPMDE) Dental Deanery, funded a pilot videoconferencing project – the Postgraduate Regional On-line Videoconferencing in Dentistry (PROVIDENT) project. The aims of PROVIDENT were to assess the educational efficacy of videoconferencing in dental CPD, and to evaluate its practicability (in terms of audience and teacher satisfaction and reliability of equipment). This paper reports the views of the dentists who formed the audiences for the project.
Materials and methods
Forty one postgraduate videoconference teaching sessions were provided by 27 experienced academic staff from the four campuses of London Dental Schools: The Eastman Dental Institute for Oral Health Care Sciences, King's College Hospital, Guy's Hospital and The Royal London Hospital. All sessions were advertised in tandem with the existing CPD courses for dentists working in primary care in the TPMDE deanery area. The sessions linked a London dental school with audiences at one of eight postgraduate centers, the locations of which are shown in the map (Figure 1), or, on two occasions, at a general dental practice.

Location of Centres involved in the project.
All sessions were organised in the same way as other Dental MADEL CPD (Section 63) courses for dentists, with the dental tutors and administrators at the postgraduate centres involved in making the necessary arrangements.6
All locations, both the dental schools and the postgraduate centres, were provided with a PC based videoconferencing H320 international standard system which incorporated a Zydacron On WAN 350 (Z350 Codec) videoconferencing card release 1.1 (Zydacron, Manchester, New Hampshire, USA)) connected by commercial ISDN2 (128 kbs) lines. Each system comprised a Toshiba Equium 7000D multimedia PC,with an Intel Pentium II microprocessor, a 64MB RAM and a 6GB hard disk, running Windows 95, Sony EV1-D31 colour videocamera and a Toshiba TLP 411E data projector with integral rostrum (document) camera (Figure 2). Sound was captured using either AKG C680 BL static autogain semidirectional microphones or lapel radiomicrophones and output via the standard PC speakers or in some centres via lecture theatre sound systems. The videoconferencing systems were mobile allowing transfer between centres. Sessions were transmitted and received using unadapted lecture theatres. One transmitting centre used an Elmo TRV-35G digitising projector (Elmo C. Ltd., 6, Kamiho-dori 1-chrome, Mizuho-ku, Nagoya, Japan) which enabled teachers to transmit a carousel of conventional 35mm slides.

The videoconferencing equipment used in the project.
A core group of lecturers, postgraduate tutors and co-ordinators, who were earmarked as the providers of technical support during the PROVIDENT project at transmitting and receiving centers, attended a one day training course at the Open University prior to the start of the project. The transmitting centres commenced live videoconferences after links to test technical issues but without practice educational transmissions. Each session was preceded by a test link to either a second postgraduate centre or the equipment supplier.
A range of topics was selected to cover as wide a range of dental specialties as possible. Amongst the subjects covered were Prosthodontics, Periodontics, Endodontics, Oral Surgery, Orthodontics, Children's Dentistry, Oral Imaging etc. Lecturers were provided with information on the types of material and presentation format suited to videoconferencing but the content of the session was entirely within their control. The following presentation styles and elements were used (more than one being possible in each session): lecture (38 times), tutorial (5 times), interactive question and answer session (30 times), case studies (8 times). Teachers used a variety of visual aids most frequently 35mm transparencies which were either transmitted digitally, (12 times) inserted with text into Powerpoint presentations transmitted live, (8 times) transmitted as live video of slides projected at a transmitting centre (13 times) or forwarded in advance either digitally or as slides for projection (6 times). A small minority of sessions used the interactive whiteboard in Microsoft NetMeeting (3 times). Radiographs were transmitted as live video camera images from a radiograph viewer (7 times) or digitally in Powerpoint presentations. Images of flat artwork, line drawings, anatomical models, dental casts and instruments were transmitted using the integral document camera in the dataprojector (12 times). All digitised images were compressed for transmission by the Zydacron videoconferencing card.
Each session was evaluated by questionnaires, which both the participants (members of the audience) and the teachers completed at the end of every session. The questionnaire completed by the participants contained both specific and open questions. The specific questions were answered using the Likert scale in which grades 1 and 2 are positive replies, grade 3 neutral and grades 4 and 5 negative. The results from the teachers' questionnaires are reported elsewhere.14
Results
Of the 41 teaching sessions only one was considered to have failed and this was for technical reasons. A total of 257 dentists attended the other 40 sessions. All completed participant questionnaires but some did not answer all questions. The reponses to the specific questions are presented in Tables 1 2 3 together with the questions asked.
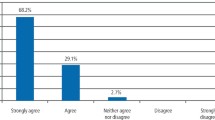
As far as the four questions on presentational style were concerned, 255 participants responded to the question on the appropriateness of the teaching material for delivery by videoconference of whom 230 (90%) gave positive responses to the question, 247 responded to the question on the ability of the lecturer as a presenter in the medium of whom 215 (87%) answered excellent or good, 246 to the question on feelings about attending further videoconferenced CPD sessions of whom 222 (90%) were positive and 245 to the question 'How did you compare the event with the alternative of travelling to London?' of whom 221 (90%) were positive (Table 1).
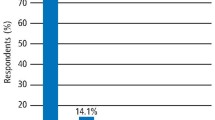
As far as the technical aspects of the sessions were concerned, there were 233 responses to the question on the visibility of the visual aids of which 161 (69%) were positive, 239 responses to the question on ability to hear the presentation, of which 128 (54%) were positive, 239 to the question on the appropriate use of the technology by the presenter of which 182 (76%) were positive. 228 responded to the question on the use of computers at home, of whom 188 (82%) claimed to have a home computer and 182 to the question 'do you have a computer at work?' of whom 129 (71%) answered yes (Table 2).
The final three specific questions related to the perceived educational value of the videoconferences. In answer to the question on the appropriateness of the educational level, there were 239 responses of which 215 (90%) were positive. 228 responded to the question on the value of visual aids to the event (session) of which 188 (82%) were positive and 224 to the question 'did you find the question and answer session useful?' of which 190 (85%) were positive.
Non-responses to questions ranged from 2 (less than 1%) to 75 (29%) with a mean of 23 (9%) – Tables 1,2 and 3.
With the exception of the question on quality of sound during the transmissions (Table 2), respondents gave very positive responses with between 69% and 90% grades 1 and 2 on the Likert scale. However, in answer to the question on sound quality, only 128 (54%) of respondents gave positive gradings (the two columns nearest the left-hand margin), a further 47 (20%) a neutral grading and the remaining 64 (26%) a negative grading.
When sound quality was reported as unsatisfactory, there were breaks, more frequently, feedback and sometimes both of these faults. This was ascribed largely to poor acoustics in the rooms used, partly to use of small computer loudspeakers and, in one or two instances, to ISDN2 transmission quality. Overall, technical problems tended to affect the earlier transmissions and were rectified without difficulty.
A further range of problems beyond the control of the project affected four transmissions temporarily. These were primarily ISDN2 line faults leading to severe pixelation or freezing of the picture (with normal sound) and overheating of a data projector.
The most frequent answers to the open question on the most useful aspects of the videoconferences were:
-
Not having to travel
-
The discussions
-
Access to first rate lecturers
-
Ability to interact with experts
Comments in response to the open question on how participants thought that presenters could improve their presentations included:
-
Move about less
-
Look into the camera and not the monitor
-
Send handouts to the audience
Participants made very favourable comments in answer to the final open question which invited any other comments. A number included the comments 'Brilliant' and 'the way forward'. Others highlighted the problems with sound quality e.g. 'needs better sound quality' or suggested future developments e.g. 'would like to have sessions to my practice'.
Discussion
Videoconferencing has been used for a variety of purposes in medicine and dentistry. Postgraduate education has been an element in many studies of videoconferencing 12,15,16,17 and continuing education has proved a common theme in those pilot studies which have remained active beyond the pilot phase.9 Possible benefits for the UK have been reviewed with the experiences of the UK Teledent project.12 Many of these studies have adopted videoconferencing to overcome great distances or dispersed communities and have provided education in tandem with other telemedicine functions. The current study appears to be the first in which videoconferencing has been used to overcome the time rather than the geographical constraints of travel. To date, few studies have directly assessed educational benefit.18,19,20
Successful videoconferencing requires training in both technical and in educational methods.21 In the present study, a core group of staff from the transmitting and receiving stations were provided with a one day training course covering simple technical issues and educational best practice for video-presentation. A short summary of key issues was produced and sent to all centres and a part-time project co-ordinator was available to travel to centres and provide help and training. As almost all staff were novices, the importance of keeping teaching simple and preparing well were stressed.22
This pre-project training appears to have been effective as, with the exception of their answer to the question on sound quality, the participants predominantly gave positive or very positive answers to all the other questions. Unsurprisingly, in view of the small numbers attending each session and the relatively few questions, all 257 participants completed questionnaires. However, not every question was answered by all participants. There appears to be no obvious reason for this and with the exception of the question on ownership of a computer at work, which was answered by 182 and unanswered by 75 of the 257 participants, all other questions were answered by the vast majority of the participants (between 224 and 255). The majority considered that the teaching material for the sessions was appropriate for delivery by videoconferencing and that the presenters made good use of the technology. In general, participants rated the presenters highly in their use of the medium, were able to see the visual aids adequately and felt that they added to the value of sessions. Although on occasion, some presenters were seen to 'move about too much' and 'not look into the camera'. The participants also found the question and answer sessions to be useful and that they could interact with the presenters in spite of being 'at a distance'. The finding that the majority of participants used computers both at work and at home was not surprising and mirrored the results of the national survey carried out in 1997 by the Dental Practice Board.23
As with all educational activities, it is important that the knowledge level is right for the audience. In this respect, it was encouraging that over 80% of the participants felt that this had been achieved in the videoconferences. However, perhaps the most encouraging answers from the participants were in response to the question about attending further videoconferencing sessions for CPD and the benefits in saving travelling time. It is pertinent to stress that travelling time is not necessarily related to distance. The shortest distance between one of the postgraduate centres and the nearest London teaching hospital was only 12 miles and the furthest 70 miles. However, during the last 12 months, even out of rush hours, it has been impossible to make even the 12 mile journey door to door into Central London in less than one hour, whether by public or private transport. Return journeys to attend similar courses at the teaching hospitals, if they had not been delivered by videoconference, would have been between a minimum of two and a maximum of six hours, with significant costs to the participants in lost clinical time. If delivered face to face at the postgraduate centres, it is likely that there would have been less loss of time to the participants and significantly more to the teachers. Cost savings resulting from the use of videoconferencing in dental vocational training and postgraduate education have been reported recently.24 However, they were not calculated in this study.
A wide range of videoconferencing systems are available. The present study opted for a low cost system based on desktop computers and ISDN2 connection which was judged sufficient to assess the feasibility of providing general postgraduate teaching. An inexpensive solution does not preclude educational benefit, provided technical reliability is good.18 In the present pilot study the quality of videoconferencing was generally deemed good with technical problems limited mainly to sound quality. Other, usually more significant, technical failures were the result of poor training or ISDN2 line transmission quality and in only a few instances was the picture quality deemed inadequate. It is clear that sound quality needs to be improved in order to maintain the audience-presenter contact and to ensure that question and answer sessions are effective. Ultimately, improved sound quality will require the additional bandwidth offered by ADSL, ISDN6 or other connections. However, satisfactory sound can be achieved using ISDN2 by ensuring that the acoustic properties of the rooms are optimal.
In this study all but two of the transmissions were to postgraduate centres. In the future it is planned to transmit direct to dental practices on topics requested by the practitioners themselves. It is hoped that the topics will be requested after the practitioners concerned have found that they need advice or updating on these topics, ideally after carrying out clinical audit. In this way the medium can be used to address the specific educational needs of small groups of dentists.
In conclusion, this pilot study has been undertaken using relatively inexpensive computer/ISDN2 equipment. The participants were overwhelmingly positive about the medium, the quality of the sessions and their educational value. The low bandwidth technology has been rated relatively successful despite problems with sound quality. However, technical unreliability and shortcomings in the sound and visual clarity need to be improved. Nevertheless, the future possibility of videoconferencing with dentists at work or at home in response to their individual educational needs offers exciting possibilities for the future.
References
Mouatt RB, Veale B, Rothwell PS. Continuing education in the GDS. An England study. Br Dent J 1991; 170: 76–79.
Holt RD, Rule DC, Basker RM., Davenport JC, Ralph JP, Murray JJ, Eaton KA. The influence on partial denture design of a teaching video for general dental practitioners. Br Dent J 1994; 176: 379–383.
Morris S. An evaluation of the Teamwork programme. Br Dent J 1992; 172: 212–214.
Eaton KA, Pendlebury M, Brown GA. Two groups of dentists evaluation of a self-assessment manual. J Dent Res 1996; 75: 359.
Eaton KA. CAL for general dental practitioners: an evaluation of the current scene. In: Richards B. editor. British Computer Society Health Informatics Specialist Groups. Conference Proceedings; 1994; March 21–23; Harrogate. Weybridge : Current Perspectives in Healthcare Computing, 1994; 97–102.
Eaton KA, Veale B, Rothwell PS, What are Section 63 and 'approved' courses and how are they organised. Br Den J 1992; 173: 307–311.
Mercer PE, Long AF, Ralph JP, Bailey H. Audit activity and uptake of postgraduate dental education among General Dental Practitioners in Yorkshire. Br Dent J 1998; 184: 138–142.
Lifelong Learning, Taking Dentistry Forward - Recertification for the Dental Profession. General Dental Council Brochure 2000. General Dental Council, London.
Elford R. Telemedicine activities at Memorial University of Newfoundland: a historical review, 1975-1997. Telemed J 1998; 4: 207–224.
Edelman G, Hall A. Innovation and partnership: the voluntary sector contribution. Int J Lang & Comm Disorders 1998; 33: 10–15.
Cook J. ISDN videoconferencing in postgraduate dental education and orthodontic diagnosis. CTICM Update 1997; 8: 8–10.
Cook J, Austen G, Stephens C. Videoconferencing: what are the benefits for dental practice. Br Dent J 2000; 188: 67–70.
Steed M. Evaluation of a teledental PC videoconference link in the delivery of a restorative dentistry service to remote dental practices in Scotland. Proceedings of the 7th International Conference on Telemedicine and Telecare, London UK, TeleMed99. 1999: 205.
Odell EW, Francis CA, Eaton KA, Reynolds PA, Mason R. A pilot study of videoconferencing for postgraduate continuing education in dentistry in the UK – a teachers view. Eur J Dent Ed 2001; 5: 113–119.
Hovenga EJ. Using multi media to enhance a flexible learning program: lessons learned. Proceedings / AMIA Annual Symposium 1999; 530–534.
Chen HS, Guo FR, Lee RG. Recent advances in telemedicine. Journal of the Formosan Medical Association 1999; 98: 767–772.
Weber JR, Lawlor AC. Professional nursing series by videoconferencing. Journal of Continuing Education in Nursing 1998; 29: 161–164.
Jarrett C, Wainwright P, Lewis L. Education and training of practice nurses. Journal of Telemedicine and Telecare 1997; Suppl 1: 3: 40–42.
Reiss J, Cameon R, Matthews D, Shenkman E. Enhancing the role public health nurses play in serving children with special health needs: an interactive videoconference on Public Law 99-457 Part H. Public Health Nursing 1996; 13: 345–352.
Mason R. The educational value of ISDN. In: Mason R, Bacsich P, eds. ISDN applications in education and training. Exeter: Short Run Press, 1994; 25–38.
Blignault I, Kennedy C. Training for telemedicine. Journal of Telemedicine and Telecare 1999; 5 Suppl 1: S112–4.
Sen Gupta TK, Wallace DA, Clark SL, Bannan G. Videoconferencing: practical advice on implementation. Australian Journal of Rural Health 1998; 6: 2–4.
Dental Practice Board. Dental Computer Survey 1997. Eastbourne: DPB.1998.
Cook J & Stephens CD. The potential and costs of videoconferencing in dental education and dental vocational training and MFDS preparation. Annals of the Royal College of Surgeons and Faculty Bulletin 2000; 82: 161–163.
Acknowledgements
We are grateful to Thames Postgraduate Medical and Dental Education Deanery for funding the project and providing facilities at participating postgraduate centres in the Thames Region. We also wish to thank Toshiba and MVision Videoconferencing Ltd (Reading, UK) for supply of equipment, technical advice and support throughout the project. We are indebted to Claire Westerbeke, PROVIDENT coordinator for central organisation of the project, technical assistance and training and to all the Postgraduate Dental Tutors and their Administrators who ran the pilot sessions at the receiving end of the videoconferences. Finally, we wish to thank Kate McWilliams for her help in preparing the figures.
Author information
Authors and Affiliations
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Eaton, K., Francis, C., Odell, E. et al. Participating dentists' assessment of the pilot regional online videoconferencing in dentistry (PROVIDENT) project. Br Dent J 191, 330–335 (2001). https://doi.org/10.1038/sj.bdj.4801176
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4801176
This article is cited by
-
A description of the new technologies used in transforming dental education
British Dental Journal (2008)
-
Seeing is believing: dental education benefits from developments in videoconferencing
British Dental Journal (2008)
