
Key Points
-
Anterior crown fractures are commonplace in children and adolescents and may affect up to 25% of this patient population.
-
If an intact tooth fragment is present after trauma, the incisal edge reattachment procedure presents a conservative, simple and aesthetic treatment.
-
Clinical trials and long-term follow-up have reported that reattachment using modern dentine bonding agents or adhesive luting systems may achieve functional and aesthetic success for up to 7 years.
-
Reattachment failures may occur with new trauma, parafunction, or horizontal traction. Athletic soft mouthguards and patient education may enhance clinical success.
Abstract
This article presents an overview of the evolution of the incisal edge reattachment procedure. Case reports are described of patients presenting with traumatised teeth in which the reattachment procedure was performed. A review is provided of present in vivo studies detailing long-term success rates in the clinical application of this procedure. Finally, a recommended technique for diagnosis and treatment is offered to improve success in this procedure which may benefit a significant segment of the paediatric and adolescent populations.
Similar content being viewed by others

Main
Recent investigations into the incidence of dental trauma, especially in the paediatric and adolescent populations, have made it clear that this particular injury is of a significant nature and effects up to one-third of patients in this age group.1 Prior studies have reported estimates that about one out of every four persons under the age of 18 will sustain a traumatic dental injury in the form of an anterior crown fracture.2,3 More recent investigations through clinical examinations of large adolescent populations and surveys of lay knowledge on the management of avulsed teeth provide dentoalveolar trauma incident estimates ranging from 6–34%.1,3,4,5,6 These reports confirm that dentists are confronted with managing dental trauma and restoring fractured teeth on a regular basis. Techniques that speed and simplify treatment, restore aesthetics, and improve long-term success rates are therefore of potential value and should be considered. The recent investigation by Hamilton et al. however, revealed high failure rates for treatments extended to adolescents experiencing dentoalveolar trauma, as well as a low knowledge level concerning management of specific traumatic injuries.5
A review of 25 published case reports indicates that 85% of traumatised incisors fracture in an oblique fashion from the labial to lingual aspects with the fracture line proceeding in an apical direction. This tendency has been confirmed in an in vitro investigation by Stokes.7 This study demonstrated that the presence of this unfavourable fracture pattern, once restored, exhibits a low resistance to labially applied forces which mimic trauma force vectors, but may exhibit higher resistance to horizontal traction forces which occur with incising or tearing food. Other laboratory investigations have been published using models addressing a variety of materials and preparation designs in an attempt to optimise the strength and consistency of the reattachment procedure.8,9,10,11,12,13
The dental profession has attempted to educate the lay public to the prompt and appropriate management of avulsed teeth.2,14 Numerous international campaigns to improve the emergent response necessary to optimise the prognosis in replantation cases have been carried out in Australia, Denmark, Brazil, Argentina, and the United States.14 These educational attempts may result in patients (or parents) presenting with intact avulsed teeth, as well as fractured coronal tooth fragments. This article will address the treatment regimen for incisal edge reattachment, a treatment option that offers advantages of simplicity, immediate aesthetics, and conservatism in cases of dental trauma.
Historical perspective
The first published case reattaching a fractured incisor fragment was reported in 1964 by paediatric dentists at Hebrew University, Hadassah School of Dentistry.15 In an era of dentistry prior to commonplace acid-etching and bonding, the authors termed this treatment a temporary restoration. Other reports espousing a variety of preparation design features and materials for reattachment have appeared in the literature restoring teeth presenting with and without pulpal or periodontal complications.16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43 Though some in vitro investigations attempted to define optimised materials and reattachment regimens, the majority of design features had been chosen empirically.
Reattachment techniques have been described in demanding clinical situations,34,38 including one case reported by Simonsen in which an incisor fragment was reattached and the tooth subsequently subjected to orthodontic treatment without difficulties.23 The reattachment regimens cited above can aid in treatment when concomitantly addressing endodontic therapy, periodontal management of biologic width violations, or electrosurgical gingivectomy.15,16,19,24,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43
Other innovative approaches to conservation of natural tooth structure include recovery of a retained, fractured crown segment in the lip of a patient presenting 3 years after history of sports trauma or bonding multiple fragments together for subsequent reattachment.17,40 Though unsupported by laboratory studies or clinical trials, many successful case reports were published in the mid-to-late 1980s by a variety of authors.23,24,25,26,27,28,29,30,31,32 An assortment of beveled designs, endodontic adjunctive care, dentinal channels, and composite resin materials and technique choices were employed. These case reports range in follow-up from 3 months to 36 months, and are overwhelmingly positive regarding retentive and esthetic success.
Andreasen et al. described the clinical procedure for reattachment of fractured incisal edges based on their unpublished clinical collection of 76 permanent incisors restored with what they termed the 'GLUMA technique'.21 This article described clinical steps for restoring both uncomplicated and complicated fractures for incisors. The technique involved placing a temporary restoration for a waiting period: 4 weeks for uncomplicated and 3 months for complicated fractures. After verification of the vitality of the tooth, the fragments were reattached using an acid etch/dentine bonding regimen and no preparation of the tooth or fragment. Recent multicentre trials and long-term studies have established this treatment option as successful in many instances.22,46 Though initiated early in the evolution of dentine bonding agents, the Andreasen group reported 25% retention of fragments at 7 years and noted that this technique is especially useful for young patients presenting with the need for apexigenesis or in the mixed dentition stage where delaying prosthetic restoration of the tooth until eruption and tooth positioning have stabilised is a distinct advantage.22 As an additional study finding when reviewing cases of fragment reattachment, these authors reported that 50% of the reattached fragments were lost within the first year when only enamel bonding was used, while 3 years elapsed before 50% of fragments were lost when dentine bonding was carried out.22 It would therefore appear desirable to obtain bonding between the opposed dentine surfaces as well as from enamel. Cavelleri and Zerman published higher success rates (though on a more limited study size) and suggest that reattachment regimens may be used for longer term restoration when clinical conditions are favourable.46 An additional long-term study of 50 incisal fragment reattachments reported an 80% success rate at 5 years when incisal fragments of approximately one-half the length of maxillary central incisors were replaced using acid-etching, internal V-shaped notches, bonding agents, and a visible-light cured composite.47
While Kanca and Baratieri et al. have also described the use of dentine bonding systems such as All-Bond 2 (Bisco Dental, Itaska, IL, USA)44 and Scotchbond Multi-purpose (3M Dental, St Paul, MN, USA),39 respectively, in the repair of fractured incisor teeth, other clinicians have used alternative approaches. Baratieri and co-workers described the use of the glass ionomer/resin 'sandwich' technique.37 The use of an 'adhesive' luting material based on the resin 4-methacryloxyethyl trimellitate anhydride with the setting reaction initiated by tri-n-butyl borane (4-META) is another alternative and this material has been reported to provide high bond strengths to enamel and to dentine. Cooley and co-workers in 1991 reported that the material demonstrated better bond strengths to dentine than any material previously tested in their laboratory.48 Clinicians have thus considered this 4-META luting material suitable for luting fractured tooth fragments to remaining tooth structure, and cases of reattachment of fractured fragments have been described using this technique.49,50,50 Two recent technique articles voice agreement in promoting the reattachment procedure based on improvements in materials and properties of modern adhesive bonding.51,52
Published advantages and disadvantages gleaned from these multiple case reports for incisal edge reattachment are listed in Table 1.
Case reports
Three case reports will be described, giving details for a variety of situations and treatments: for full details, the reader should consult the original texts.35,49 Report 1 describes the use of dentine and enamel bonding to effect a repair, and Reports 2 and 3 describe the use of an adhesive luting system. In the first two cases, gross exposures of the pulp during the traumatic incident made root canal therapy necessary, but in the last case report a small exposure was treated using the bonding/luting system.35,49
Case report 1
Following trauma to her upper left central incisor tooth (fig. 1), a 10-year-old girl attended a dental surgery for emergency treatment. Her mother had retrieved the fractured fragment. Radiographic examination showed that root formation was complete and that there was no root fracture. The patient was in pain as a result of a large pulpal exposure, and accordingly, the pulp was extirpated, the canal dressed following instrumentation and the canal obturated one week later. The retained root and the fractured fragment were treated with the components of a dentine bonding system, a hybrid composite material placed between the fragments and the fractured portion placed against the retained root. Excess composite was removed and the composite light cured from labial and palatal directions. After light curing, the margins were polished using discs and impregnated rubber points. At recall 1 year later, the repair was performing satisfactorily (fig. 2). Following further trauma after 3 years, the fragment debonded. It was not possible to satisfactorily appose the fragment to the remaining tooth, and the tooth was restored initially by a post-retained composite build-up and later by a post crown.

Upper left central incisor exhibiting typical facial-lingual sloping fracture pattern and large pulpal exposure (Ellis Class III fracture) (from ref. 35)

Reattachment of the fragment remained successful at the one year recall visit. The reattachment ultimately failed due to recurrent trauma (from ref. 35)
Case report 2
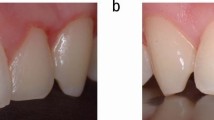
During an assault, a male patient aged 23 years suffered a fracture of the crown of the upper left central incisor tooth, with the fracture line extending below the gingival margin by 1 mm palatally (fig. 3). The pulp was exposed, so root canal treatment was initiated and the root canal obturated 1 week later. A friend of the patient had recovered the fractured tooth fragment; this was cleaned using a pumice and water slurry, and was found to fit satisfactorily.

A physical assault yielded this fractured central incisor (Ellis Class III), again with pulpal involvement, necessitating endodontic therapy consisting of pulpal extirpation and subsequent obturation
The disadvantages and advantages of the reattachment procedure were discussed with the patient and a decision to proceed was made. Following isolation, the enamel margins of the retained root and the fractured fragment were etched with 35% orthophosphoric acid for 1 minute, washed and dried. The dentine of the root and fractured fragment was conditioned with the aqueous solution of 10% citric acid and 3% ferric chloride provided with the proprietary 4-META luting system (Metabond, Sun Medical Co., Kyoto, Japan) selected for the reattachment. The luting material was mixed and applied to the tooth fragment, which was placed in position. Excess luting material was removed and the fragment held in position for 10 minutes. The margins of the repair were finished and polished as described for Case 1. A thin layer of composite restorative material, retained by acid etching an area 1 mm adjacent to the fracture line labially, was placed to improve the aesthetics of the repair. The occlusion was checked and adjusted, and the patient discharged, having been given post-operative instructions. At review at 6 months (fig. 4) and 2 years, the repaired tooth was found to be symptom-free. However, further reevaluation was not possible as contact was lost with the patient after the 2-year recall visit.

Reattached incisor fragment is successfully retained at the 6-month recall visit
Case report 3
A male exchange student from France suffered trauma from a squash racquet in the first week following his arrival in England, resulting in incisal fractures of the upper left and right central incisor teeth. (fig. 5). The pulp was visible on the palatal aspect of the fracture in the upper right central incisor, but there was no haemorrhage.

Fractured central incisor exhibiting Ellis Type III fracture on upper right central and Ellis Class II on the upper left central incisor. No pulpal therapy was instituted for the exposed pulp, but dentine bonding was accomplished and the fragments reattached with an adhesive luting system (C&B Metabond)
The patient had recovered the fractured fragment of the upper right central incisor tooth. No root fracture was visible on radiographical examination. After isolation of the central incisor teeth using rubber dam, the fractured tooth fragment of the upper right central incisor tooth was cleaned and was tried against the remaining tooth and was found to fit satisfactorily. After discussion with the patient of the advantages and disadvantages of the techniques involved, it was decided that an attempt should be made to bond the lost fragment to the remaining tooth.
The upper left central incisor was restored using Scotchbond MP and Z100 (3M, St. Paul, MN, USA). For the upper right central incisor tooth, the retained tooth and the fractured fragment were cleaned using a pumice and water slurry, the enamel of the retained root and the fractured fragments etched with 35% orthophosphoric acid; the dentine surface, including the exposure site, was treated with the 10% citric acid, 3% ferric chloride conditioner provided by the manufacturer of the 4-META luting system chosen for use in the reattachment (Metabond, Sun Medical Co, Kyoto, Japan). The tooth and fragment were washed with water and dried and the fractured fragment recemented to the remaining tooth using the 4-META cement. Excess cement was removed, and when the 4-META cement had cured, a layer of composite was placed across the fracture line labially; the occlusal relationship of the central also allowed the placement of a palatal layer of composite across the fracture line. At recall, 1 year later, the replaced tooth fragment was still in position (fig. 6) and vitality testing of both teeth gave similar, vital readings. The patient returned to France with a request that the clinician should be advised if the repair had failed, and, to date, 4 years following the repair, no contact has been received from the patient.

Reattached fragment remains successful at 1 year, teeth are vital, asymptomatic, and aesthetically acceptable
Discussion and clinical technique
Functional, aesthetic, and biologic restoration of the fractured incisor often presents a daunting clinical challenge. Conventional composite resin restoration may result in less than ideal contours, colour match, and incisal translucency. Prosthodontic restoration in cases involving younger patients is questionable as confounding variables such as a large pulpal sizes, progressive eruption, and gingival margin instability take this predictable treatment modality for adults and turn the treatment outcome into one of uncertain longevity. When an intact fragment is available, incisal edge reattachment may offer a most functional and aesthetic treatment option. As with conventional restoration, restorative success hinges on proper case selection and strict adherence to sound principles of periodontal and endodontic therapies, and the techniques and materials for modern adhesive dentistry.22,46
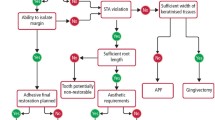
With regard to clinical success, the incisal fragment should ideally exhibit no caries, negligible loss of tooth structure, and adapt well to the remaining tooth structure when 'tried-in'. The absence of traumatic occlusion should be confirmed.47 Root integrity and maturation status are assessed with pre-operative periapical radiographs. Periodontal diagnostic testing detects biologic width concerns, the treatment of which ensures adequate isolation and future periodontal health. Initial post-trauma endodontic diagnostic testing, although unreliable, is integrated with radiographic findings to provide a basis for future endodontic treatment decisions.
Rubber dam isolation facilitates successful management of endodontic complications and provides an environment conducive to quality adhesive dentistry. An important consideration for clinicians may be the effects of different fracture patterns on the long-term success of the reattachment treatment. Bond strength measurements to dentine which are similar to those found with enamel ('the gold standard') are now achieved with many systems and high retention rates of restorations in non-retentive, non-stress-bearing cavities are also possible. However, it may be considered that the achievement of an intimate reapproximation of the segments giving a semblance of resistance form within the fracture line to prevent rotation of the reattached fragment on the remaining tooth structure may serve to protect the bond from rotational and twisting forces which may reduce the potential for success. A pumice-water slurry removes any pellicle and the use of a phosphoric acid etch and/or material specific '10-3 conditioning' may be employed to facilitate enamel bonding, promote interdiffusion and the formation of a hybrid layer, and act as an antimicrobial agent against oral bacteria.54 In all cases, bonding to dentin should be employed given that the results of multicentre clinical studies of fractured incisors have indicated a more favourable prognosis when a dentin bonding system is used during the repair.22 Furthermore, results of treatment using a dentine bonding agent and replacement of the fragment in which around half of the reported cases had suffered a pulpal exposure have indicated a low proportion (4%) with pulpal necrosis.22 Contemporary dentine bonding agents with high, demonstrable bond strength values with a total-etch, moist bonding technique reunites the fragment and remnant, and a highly filled composite resin added as necessary to replace lost tooth structure and optimise aesthetics.
The restoration should be finished, polished, and a composite surface sealant placed. If aesthetics are compromised, premature separation anticipated, or a degrading bond noted, subsequent restoration with porcelain or cast ceramic veneers to reinforce the weakened edge is in order.42,55 Strong consideration must be given to the fabrication of a soft polyvinyl or acrylic mouthguard to be worn in athletic competition or at night (if the patient exhibits a nocturnal parafunctional habit) as these conditions may predispose the reattached fragment to an early failure. Recall examination permits observation and direct provider feedback.
The current view
An advantage of the incisal edge reattachment procedure is that it does not preclude any future treatment and therefore, in cases where the fragment is available, represents a viable first treatment option. Andreasen and Andreasen state that the reattachment procedure may importantly serve as a transitional treatment alternative for pre-teens or teenage patients to postpone definitive treatment until an age where gingival margin contours are relatively stable.56 Patients should be appraised of the advantages and disadvantages and should make an informed decision based on the dentist's recommended treatment regimen founded on trends gleaned from the results of clinical trials and published case reports. A quote by Liew is very appropriate in describing the prognosis for this procedure. He believes this restoration to act as 'a short to medium term temporary restoration which has the potential for indefinite service'.31 The outcomes of the cases described in this article are in keeping with the results of the multicentre study by Andreasen in that long-term success was elusive in a number of the cases. However, it appears that improvements in the luting and/or bonding systems employed and a greater knowledge of the factors influencing restoration longevity should serve to enhance the potential for success of reattachment techniques in the future.
Conclusions
The incisal fragment reattachment procedure may offer a conservative, cost-effective, and aesthetic restorative option when patients present with intact incisal edge segments. The use of a moist bonding procedure using fourth or fifth generation dentine bonding agents without additional retention features (such as internal or external preparation) has been shown to provide clinical restorative success. Research through laboratory findings and clinical observations show debonding failures when rapid loading is applied (simulating trauma to the reattached fragment), yet current adhesive agents provide sufficient bonding strengths to withstand the slow loading from masticatory stresses. This bonded interface is undeniably susceptible to the effects of cyclic fatigue and hydrolytic degradation over time. Despite these factors, case reports and multicentre studies have described functional and aesthetic successes exceeding 7 years.
This article was prepared in part by officers of the United States Government as part of those persons' official duties and is deemed a work of the United States Government. Accordingly, this material may not be copyrighted and may be reprinted without permission. Figures 3 – 6 are reproduced courtesy of Dental Update.
References
Hamilton F A, Hill F J, Holloway P J . An investigation of dento-alveolar trauma and its treatment in an adolescent population. Part 1: The prevalence and incidence of injuries and the extent and adequacy of treatment received. Br Dent J 1997; 182: 91–95.
Andreasen J O, Ravn J J . Epidemiology of traumatic dental injuries to primary and permanent teeth in a Danish population sample. Int J Oral Surg 1972; 1: 235–239.
Petti S, Tarsitani G . Traumatic injuries to anterior teeth in Italian schoolchildren: prevalence and risk factors. Endod Dent Traumatol 1996; 12: 294–297.
Hamilton F A, Hill F J, Mackie I C . Investigation of lay knowledge of the management of avulsed permanent incisors. Endod Dent Traumatol 1997; 13: 19–23.
Hamilton F A, Hill F J, F J, Holloway P J . An investigation of dento-alveolar trauma and its treatment in an adolescent population. Part 2: dentists' knowledge of management methods and their perceptions of barriers to providing care. Br Dent J 1997; 182: 129–133.
Burton J, Pryke L, Rob M, Lawson J S . Traumatised anterior teeth amongst high school students in northern Sydney. Aust Dent J 1985; 30: 346–348.
Stokes A, Hood J . Impact fracture characteristics of intact and crowned human central incisors. J Oral Rehabil 1993; 20: 89–95.
Dean J, Avery D, Swartz M . Attachment of anterior tooth fragments. Ped Dent 1986; 8: 139–143.
Munksgaard E, Højtved L, Jørgensen E, Andreasen J, Andreasen F . Enamel-dentin crown fractures bonded with various bonding agents. Endod Dent Traumatol 1991; 7: 73–77.
Andreasen F, Steinhardt U, Bille M, Munksgaard E . Bonding of enamel-dentin crown fragments after crown fracture. An experimental study using bonding agents. Endod Dent Traumatol 1993; 9: 111–114.
Andreasen F, Flügge E, Daugaard-Jensen J, Munksgaard E . Treatment of crown fractured incisors with laminate veneer restorations. An experimental study. Endod Dent Traumatol 1992; 8: 30–35.
Badami A, Dunne S, Scheer B . An in-vitro investigation into the shear bond strengths of two dentine-bonding agents used in the reattachment of incisal edge fragments. Endod Dent Traumatol 1995; 11: 129–135.
Worthington R B, Murchison D F, Vandewalle K S . Incisal edge reattachment: the effect of preparation design. J Dent Res 1998; 77 (Special Issue A, Abstract #1238): 260.
Andreasen J O, Andreasen F M . Textbook and color atlas of traumatic injuries to the teeth. 3rd ed. p.213. Copenhagen: Munksgaard, 1994.
Chosack A, Eidelman E . Rehabilitation of a fractured incisor using the patient's natural crown — case report. J Dent Child 1964; 71: 19–21.
Spasser H . Repair and restoration of a fractured, pulpally involved anterior tooth: report of case. J Am Dent Assoc 1977; 94: 519–520.
Mader C . Restoration of a fractured anterior tooth. J Am Dent Assoc 1978; 96: 113–115.
Tennery T . The fractured tooth reunited using the acid-etch bonding technique. Texas Dent J 1978; 96: 16–17.
Simonsen R . Traumatic fracture restoration: An alternative use of the acid etch technique. Quintessence Int 1979; 2: 15–22.
Starkey P . Reattachment of a fractured fragment to a tooth. J Indiana Dent Assoc 1979; 58: 37–38.
Andreasen F M, Rindum J L, Munksgaard E C, Andreasen J O . Bonding of enamel-dentin crown fractures with GLUMA® and resin. Endod Dent Traumatol 1986; 2: 277–280.
Andreasen F M, Noren J G, Andreasen J O, Engelhardtsen I, Lindh-Stromberg U . Long term survival of fragment bonding in the treatment of fractured crowns. Quintessence Int 1995; 26: 669–681.
Simonsen R . Restoration of a fractured central incisor using original tooth fragment. J Am Dent Assoc 1982; 105: 646–648.
Croll T . Dentin adhesive bonding: new applications (I). Quintessence Int 1984; 10: 1021–1027.
Croll T . Dentin adhesive bonding: new applications (II). Quintessence Int 1984; 11: 1123–1129.
Osborne J, Lambert R . Reattachment of incisal tooth fragment. Gen Dent 1985; 33: 516–517.
Ludlow J, La Turno S . Traumatic fracture: 1-visit endodontic treatment and dentinal bonding reattachment of coronal fragment: report of case. J Am Dent Assoc 1985; 110: 341–343.
Amir E, Bar-Gil B, Sarnat H . Restoration of fractured immature maxillary central incisors using the crown fragments. Ped Dent 1986; 8: 285–288.
DiAngelis A J, Jungbluth M A . Restoration of an amputated crown by the acid-etch technique. Quintessence Int 1987; 18: 829–833.
Martens L, Beyls H, Craene L, D'Hauwers R . Reattachment of the original fragment after vertical crown fracture of a permanent central incisor. J Pedod 1988; 13: 53–62.
Liew P . Reattachment of original tooth fragment to a fractured crown. Case report. Aus Dent J 1988; 33: 47–50.
Ehrmann E . Restoration of a fractured incisor with exposed pulp using original tooth fragment: report of case. J Am Dent Assoc 1989; 118: 183–185.
Dorignac G, Nancy J, Griffiths D . Bonding of natural fragments to fractured anterior teeth. J Pedod 1990; 14: 132–135.
Baratieri L, Monteiro S, Caldeira de Andrada M . Tooth fracture reattachment: case reports. Quintessence Int 1990; 21: 261–270.
Burke F J T . Reattachment of a fractured central incisor tooth fragment. Br Dent J 1991; 170: 223–225.
DiAngelis A J, Jungbluth M A . Reattaching fractured tooth segments: an esthetic alternative. J Am Dent Assoc 1992; 123: 58–63.
Baratieri L, Monteiro S, Caldeira de Andrada M . The 'sandwich' technique as a base for reattachment of dental fragments. Quintessence Int 1991; 22: 81–85.
Baratieri L, Monteiro S, Cardoso A, de Filho J C M . Coronal fracture with invasion of biologic width: a case report. Quintessence Int 1993; 24: 85–91.
Baratieri L, Monteiro S, Mendes de Albuquerque F, Vieira L, Caldeira de Andrada M, Filho JC de M . Reattachment of a tooth fragment with a 'new' adhesive system. Quintessence Int 1994; 25: 91–96.
Blakytny C, Chadwick B . Treatment of an immature complicated crown fracture: a case report. Dent Update 1994; 21: 36–37.
Dickerson W G . Conservative reattachment of a pulpally exposed, fractured incisor. Dent Econ 1994; 84: 90–91.
Hyde T P . A reattachment technique for fractured incisor tooth fragments: a case history and discussion of alternative techniques. Prim Dent Care 1995; 2: 18, 20–22.
Walker M . Fractured-tooth fragment reattachment. Gen Dent 1996; 44: 434–436.
Kanca, J . Replacement of a fractured incisor fragment over pulpal exposure: a case report. Quintessence Int 1993; 24: 81–84.
Kanca J . Replacement of a fractured incisor over pulpal exposure: a long-term case report. Quintessence Int 1996; 27: 829–832.
Cavalleri G, Zerman N . Traumatic crown fractures in permanent incisors with immature roots: a follow-up study. Endod Dent Traumatol 1995; 11: 294–296.
Vijayakumaran V . Evaluation of crown restoration of fractured anterior teeth using original tooth fragment. J Dent Res 1998; 77(Special Issue B, Abstract #520): 696.
Cooley R L, Tseng E Y, Barkmeier W W . Dentinal bond strength and microleakage of a 4-META adhesive to amalgam and composite resin. Quintessence Int 1991; 22: 979–983.
Burke F J T . Repair of fractured incisors using a 4-META luting material. Dent Update 1997; 24: 358–360.
Burke F J T, Thavraj S J . Alternative uses of a 4-META material: repair of a fractured incisor tooth. Asian J Esthet Dent (in press).
Liebenberg W H . Reattachment of coronal fragments: operative considerations. Pract Periodont Aesthet Dent 1997; 9: 761–772.
Baratieri L N, Ritter A V, Junior S M, de Filho J C M . Tooth fragment reattachment: an alternative for restoration of fractured anterior teeth. Pract Periodont Aesthet Dent 1998; 10: 115–127.
Lowey M N . Reattachment of a fractured central incisor tooth fragment (letter). Br Dent J 1991; 170: 285.
Settembrini L, Boylan R, Strassler, Scherer W . A comparison of antimicrobial activity of etchants used for a total etch technique. Op Dent 1997; 22: 84–88.
Andreasen F, Daugaard-Jensen J, Munksgaard E . Reinforcement of bonded crown fractured incisors with porcelain veneers. Endod Dent Traumatol 1991; 7: 78–83.
Andreasen J O, Andreasen F M . Textbook and color atlas of traumatic injuries to the teeth. 3rd ed. p. 240, Copenhagen: Munksgaard, 1994.
Author information
Authors and Affiliations
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Murchison, D., Burke, F. & Worthington, R. Incisal edge reattachment: indications for use and clinical technique. Br Dent J 186, 614–619 (1999). https://doi.org/10.1038/sj.bdj.4800178
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4800178
This article is cited by
-
Milled versus moulded mock-ups based on the superimposition of 3D meshes from digital oral impressions: a comparative in vitro study in the aesthetic area
BMC Oral Health (2019)
-
A single visit, multidisciplinary approach to the management of traumatic tooth crown fracture
British Dental Journal (2000)
