
Abstract
Reconstruction of the dentition extensively damaged through tooth surface loss may require the use of removable prostheses. This can be the most appropriate type of treatment when either the teeth are very severely worn or the patient wishes a simpler and more economical approach than a fixed reconstruction.
Similar content being viewed by others


Main
The previous article discussed changes in the occlusion that take place when teeth wear. Severe wear, particularly when coupled with tooth loss, can produce marked changes in the occlusal relationships and significant aesthetic deficit. A removable prosthesis may be the appropriate restorative approach particularly when wear is advanced. Determination of the correct vertical dimension for the occlusion and an appropriate jaw relationship form the basis of treatment whether this employs fixed or removable prostheses. Later articles will examine both adhesive and more traditional fixed approaches to restoration. However, this paper describes the use of removable appliances for restoring dentitions affected by tooth surface loss and how the aesthetic and technical difficulties created by the lack of space may be overcome.
The maintenance of anterior facial height by compensatory growth
The craniofacial complex is not a static entity in the adult;1 there is evidence that growth, though slower than takes place during adolescence, continues into late middle age.2 An aspect of such growth ie the increase in anterior facial height has been reported.2,3,4 One of the mechanisms for this increase (in the absence of excessive tooth wear) is thought to be from the eruption of teeth because of an increase in alveolar height.5,6
Tallgren noted that with the complete dentition, anterior facial height tends to increase with age and that this increase is paralleled by the rest of the face height;3 in other words, the free-way space (FWS) remains constant. This relationship appears to hold as long as there is no appreciable destructive change in the dentition.
Where uniform wear of the occlusal surfaces and incisal edges does take place, Sicher suggests that this is compensated by continuous vertical eruption and thus attrition does not affect the proportions of the face.7 Niswonger (cited by Tallgren3) among others6,8 supported this view. He found that 80% of severe wear cases had a normal FWS ie 3 mm.
However, there is a contrary view (Thompson,4 Mershon,9 and Kazis,10) which affirms that the FWS is affected by wear and its magnitude is proportionate to the degree of attrition. Stern and Brayer11 state that: 'Pathological changes of the occlusion may occur when posterior tooth support is reduced or lost. In these cases, the mandible requires a new support which is usually found in the anterior region of the mouth. Consequently, an excessive occlusal load affects the anterior teeth. Such an event is known as 'occlusal collapse'. Russell,12 supports this concept. He considers that an FWS in excess of 5–6 mm is abnormal and that the occlusal wear which has produced it, has occurred at a rate faster than the physiological mechanisms designed to compensate for it'. This presumption is disputed in a recent paper by Smith and Robb.13
These apparently contrasting opinions are reflected in the following clinical observations. Dawson is adamant that as wear does not decrease the occlusal vertical dimension (OVD), there is no case for its increase during treatment.14 Nonetheless, he subsequently states that: 'If the contacting surface enamel is worn severely on both the upper and lower anterior teeth, there is sometimes no room to restore the surfaces... without either invading the pulp or increasing the vertical dimension. This type of problem is usually treated by opening the vertical'. Watson and Tulloch too, find a seeming paradox in relation to OVD. They comment, that: 'Clinically one frequently finds that despite considerable TSL there is very little interocclusal clearance...on the other hand...the extent of the freeway space is sometimes commensurate with a natural FWS together with the TSL'.
This apparent conflict can be resolved by modifying Pindborg's original classification of TSL.16 The latter makes a distinction between generalised and localised tooth wear.12,16
-
Compensated TSL: Tooth surface loss without loss of OVD. It generally involves a complete or nearly complete dentition and the free-way space remains within the normal range.
-
Non-compensated TSL: Tooth surface loss leading to the loss of OVD. This is often confined to the anterior segments and associated with a lack of posterior occlusion. The rate of wear, confined to a smaller number of teeth, results in an apparent lack of compensatory eruption and the free-way space is greater than normal.
With compensated TSL, the occlusal plane is generally not in doubt. During treatment, the increase in vertical dimension is usually dependent on the space required to restore the teeth. Repositioning of the mandible will re-establish a normal FWS but the anterior lower facial height (ALFH) will be increased.
With non-compensated TSL, the collapse of ALFH necessitates an increase in the vertical dimension to restore the subjects to their presumed, original OVD before TSL took place.
As patients with compensated TSL rarely present for removable partial denture (RPD) treatment, the following discussion will, in the main, be directed to non-compensated TSL.
Assessment of non-compensated TSL
The patient affected by non-compensated TSL with loss of facial height poses the same problem as in complete denture prosthodontics; how to establish a functional OVD. The absence of an acceptable occlusal plane also complicates the determination of an appropriate intercuspal position (ICP).
Two characteristics may be of value in guiding the operator toward the optimal retruded axis position (RAP) and hence a convenient occlusal vertical dimension (OVD).17
Firstly, when teeth are found distal to the worn anterior surfaces, a facet may be present which often appears to be coincident with the retruded contact position (RCP). (It will be obvious if this first contact is a result of over-eruption.) Secondly, this contact will frequently produce an acceptable OVD. This can be confirmed by reference to the patient's appearance and in particular to an unstrained relationship of the lips in apposition.
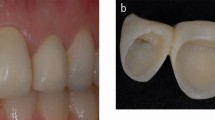
Figures 1,2a,2b,3a,3b,4,5 illustrate this suggestion. The unstable contacts seen in figures 3a and 3b may be responsible for deflecting the mandible forward into ICP, a position to which the functional movements of mastication and swallowing are normally directed.18 The posterior contacts no longer being used, the anterior teeth suffer progressive wear which is probably a combination of attrition and erosion.19 When the mandible is held at the retruded contact position, the original occlusal plane, common to both arches, can be envisaged and there is no longer any evidence of significant over-eruption. The outline of anterior tooth form can be extrapolated from the proportions of the remaining tooth structure and the available interarch space (fig. 4); a diagnostic wax-up will show this more accurately.

Note the shiny surface of the apparently non-functional amalgam surface on the |5

The posterior segments are 'collapsed' and there appears to be gross over-eruption. Note the relationship of the apparently over-erupted upper second premolar teeth to the lower first premolar. The arrows indicate the presence of wear facets

The posterior segments are 'collapsed' and there appears to be gross over-eruption. Note the relationship of the apparently over-erupted upper second premolar teeth to the lower first premolar. The arrows indicate the presence of wear facets

Note that the facets are now in contact and the apparent overeruption of the 753|578 has resolved into an acceptable occlusal plane

Note that the facets are now in contact and the apparent overeruption of the 753|578 has resolved into an acceptable occlusal plane


In ICP the patient's lower anterior facial height is very much reduced. However, at RCP the face takes on a more normal appearance. In particular note that the lips appear to be in unstrained contact
Thus, an examination of the casts mounted in RCP, will often allow the operator to visualise the degree of tooth loss and the extent of restoration required. This can be the starting point for the proposed restoration.
Treatment of non-compensated TSL
The following is a schematic outline for the treatment of TSL with a removable prostheses. Management can be divided into three stages:
-
1
Preliminary investigations
-
2
Restorative phase
-
3
Maintenance.
Preliminary investigations:
-
1
Routine examination
-
2
Note the presence and position of facets and their relationship on opposing teeth (this is most easily seen on the casts)
-
3
Assess the amount of free-way space (FWS)
-
4
Manipulate the mandible into RCP and observe the effect on the facial appearance
-
5
Make impressions of the complete arches and verify the accuracy the resultant casts20
-
6
Make duplicates of these casts after blocking out undercuts
-
7
Using a measuring device (eg Willis Bite Gauge) record the rest vertical dimension (RVD)
-
8
Take an interocclusal record at a jaw separation approximating the RVD recorded
-
9
Note the occlusal vertical height (OVD) when the teeth are in ICP
-
10
Deduct the OVD from the RVD to obtain the FWS
-
11
With the casts mounted and the interocclusal record in situ, note the reading on the scale of the incisal pin (ie this is equivalent to the RVD, see 8 above)
-
12
Close the articulator until first tooth contact and again take note of the reading on the incisal pin. (If there is no posterior contact close the articulator until the upper and lower occlusal planes appear to coincide)
-
13
Close the articulator into ICP and note the reading at the incisal pin
-
14
Compare these results with those found in vivo. If the first contact (or coincidence of the occlusal plane) produces an acceptable FWS and facial appearance, use this as a guide for restoration
-
15
An occlusal splint is constructed, as described in Part 3 of this series. It is usually most convenient to construct a maxillary appliance. Little, if any, alterations should be made to the teeth at this stage. This is to allow abandonment of treatment with a minimum of recrimination. Teeth can be added to the splint, making it, in effect, an overlay denture. When adjustments and habituation have produced a satisfactory functional and aesthetic result, the next stage can be embarked upon.
2. Restorative phase
The OVD and ICP having been established by the upper occlusal splint, it is possible to envisage two situations:
-
1
Where the lower dentition produces a satisfactory occlusal plane, there is no need for a lower denture to complement the upper splint/denture unless there are specific reasons eg aesthetics
-
2
Where the loss of teeth and tooth substance in the lower arch have created a need for a lower denture to establish a harmonious occlusal plane. The occlusal splint having followed the irregular lower occlusal plane, it itself is unaesthetic as it overlays the teeth. Two methods can be used:
-
The casts are articulated as described above and the lower denture is waxed up to meet the upper contacts, care being taken to present an harmonious occlusal plane to which the definitive upper denture can eventually be made to occlude
-
The lower cast is articulated against a cast of the occlusal splint. An idealised occlusal plane is set up, stone from the opposing cast being removed to allow this. The definitive lower denture is fitted and appropriate adjustments are made to the splint.
Choice of the denture base material
This will depend on various factors including the opposing materials and whether coverage is mainly on hard or soft tissue:
-
Because a well-supported denture is of primary importance; the best design for the definitive lower denture is based on a metal framework
-
The definitive upper denture will benefit from a metal construction if the splint has shown signs of excessive wear resulting in breakage
-
The final prosthesis can be veneered over its entire occlusal surface with cobalt chromium which will strengthen the appliance and avoid the need to attempt the reproduction of the appearance and functional occlusion de novo. When using cobalt chromium attention must be paid to the likelihood that the opposing arch may suffer accelerated wear.
Management of the appearance
Two options are available for restoring the worn teeth:
-
1
Complete facings with or without a flange
-
2
Butt joint.
The materials can be purpose-made acrylic facings, hollowed-out denture teeth or custom made in the mouth with autopolymerising resin, composite, or light curing resin. An opaquer may be necessary to mask the colour of a metal base. In the latter case, special provisions will also need to be made for retention either mechanically or chemically.
The choice of restoration will depend upon:
-
Path of insertion of the denture
-
The ability of the lip to tolerate labial coverage of the teeth
-
The height of the lip during function ie if the butt joint is visible
-
The occlusion
-
The ability to match the colour of the overlaid tooth with the restorative material.
Maintenance
One objective of treatment is to produce an appliance which is resistant to degradation but nonetheless is capable of simple servicing at routine checkups. Overlay dentures will normally be worn at night to prevent parafunctional attrition of the teeth. If it is thought that this will place the denture at too much risk an occlusal splint may be substituted.
Conclusion
The article has discussed the effects of tooth surface loss on anterior facial height and how this can be related to the distribution of wear within the mouth. Identification of the changes that have taken place is important in making a complete assessment of the patient and forming a restorative plan. Removable appliances may be the treatment of choice for some individuals, particularly when the time and cost of fixed restorations are considered. The complexities of treatment of the severely worn dentition serve to re-emphasise the importance of effective prevention as discussed in the first three parts of this series. There may also be a case for early restoration to prevent the extensive damage to the teeth which necessitates extensive reconstruction. Parts 1 and 2 mentioned a possible role for early restorative intervention to minimise further wear: this is sometimes considered controversial as concerns have been expressed over wear continuing around the margins of restorations. However, there is merit in such an approach, particularly if the restorative techniques are relatively non-invasive and it is coupled with an overall preventive approach. Part 5 examines the role of adhesive dentistry in the management of the worn dentition.
References
Crothers A, Sandham A . Vertical height differences in subjects with severe dental wear. Eur J Orthod 1993; 15: 519–525.
Behrent R G . Growth in the aging craniofacial skeleton. Craniofacial Growth series. Monograph No.17 Center for Human Growth and Development. Michigan: University of Michigan, Ann Arbor, 1985.
Tallgren A . Changes in adult face height due to ageing, wear and loss of teeth and prosthetic treatment. Acta Odont Scand 15: Suppl. 24, 1957; 73.
Thompson J L, Kendrick G S . Changes in the vertical dimension of the human male skull during the third and fourth decades of life. Anat Rec 1964; 27: 209.
Manson J D . Passive eruption. Dent Pract 1963; 14: 2–8.
Murphy T . Compensatory mechanisms in facial height adjustment to functional tooth attrition. Aust Dent J 1959; 4: 312–323.
Sicher H Oral biology. St Louis, CV Mosby Co. 1949 (in Tallgren 1957.)
Berry D C, Poole D F G . Attrition: possible mechanisms of compensation. J Oral Rehabil 1976; 3: 201–206.
Mershon J V . Possibilities and limitations in the treatment of closed-bites. Int J Orthodont 1937; 23: 581–589 (in Tallgren A. 1957).
Kazis H . Complete mouth rehabilitation through restoration of lost vertical dimension. J Am Dent Ass 1948; 37: 19–39 (in Tallgren A. 1957).
Stern N, Brayer L . Collapse of the occlusion — aetiology, symptomatology and treatment. J Oral Rehabil 1975; 2: 1–19.
Russell M D . The distinction between physiological and pathological attrition: a review. Ir Dent Assoc 1987; 33: 23.
Smith B G N, Robb N D . The prevalence of toothwear in 1007 dental patients. J Oral Rehabil 1996; 23: 232–239.
Dawson P . Evaluation, diagnosis and treatment of occlusal problems. 2nd ed. Mosby-Toronto, 1989.
Watson I B, Tulloch E N . Clinical assessment of cases of tooth surface loss. Br Dent J 1985; 159: 144–148.
Pindborg J J . Pathology of dental hard tissues. pp300–309. Copenhagen: Munksgaard, 1970.
Hemmings KW, Howlett JA, Woodley N J, et al. Partial dentures for patients with advanced tooth wear. Dent Update 1995; 22: 52–59.
Ramfjord S P . Bruxism, a clinical and electromyographic study. JADA 1961; 62: 21–44.
Lewis K J, Smith B G N . The relationship of erosion and attrition in extensive tooth tissue loss. Br Dent J 1973; 135: 400–404.
Faigenblum M J . Advice on producing an accurate impression and working cast for construction of partial dentures. Br Dent J 1985; 159: 45–46.
Acknowledgements
This article is based on a presentation at The Medical Society of London on 15 December 1994 as part of the Alpha Omega lecture programme.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Faigenblum, M. Removable prostheses. Br Dent J 186, 273–276 (1999). https://doi.org/10.1038/sj.bdj.4800086
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4800086
