
Abstract
Objective To ascertain the emergency drugs and equipment possessed by general dental practitioners (GDPs), the treatment provided and drugs used in management of the medical emergency events they reported.
Design Postal questionnaire survey of a random sample of GDPs in Great Britain.
Subjects 1500 GDPs, 1000 in England & Wales and 500 in Scotland.
Results There was a 74% response. An aspirator, an airway, oxygen, adrenaline and an injectable steroid were possessed by about 90% of respondents; glucose, glyceryl trinitrate and a salbutamol inhaler by about 80%. Glucose was used in management of nearly one in ten of the events reported, an inhaler, glyceryl trinitrate and oxygen were the next most commonly used. Cardiopulmonary resuscitation (CPR) was carried out in management of 1.1–1.4% of events not associated with general anaesthesia (GA) and in 4.7–16% of events associated with GA, an average of once in 250 years of practice.
Conclusions Most respondents possessed drugs and equipment necessary to manage a medical emergency. Half the drugs recommended by the 'Poswillo report' to be available in every dental practice were not used in more than 8000 years of practice.
Similar content being viewed by others

Main
A number of studies have been carried out which sought to ascertain the emergency drugs and equipment possessed by dentists. In 1986, Shirlaw et a1.1 reported the results of a questionnaire survey of 1200 GDPs in the south west of England which found that, based on a 40% response, 38% of respondents possessed an airway, 31% adrenaline, 30% hydrocortisone, 14% glucose, 12% an antihistamine and 12% an AMBU bag, but 20% were found to have no specific means of giving oxygen in an emergency. More recently, a similar survey was conducted among a random sample of 1250 GDPs in Australia. It was found that 63% possessed oxygen, 27% a manual resuscitator, 22% adrenaline, 13% a bronchodilator spray, 11% oral glucose, and 9% glyceryl trinitrate and hydrocortisone injection.2
Emergency drugs and equipment which should be available in a dental surgery for the management of a medical emergency have been recommended by a number of authorities,3,4,5,6 including the 'Poswillo report',7 whose recommendations are listed in Table 1. The recently revised General Dental Council (GDC) guidelines recommend that all dental practices have available portable suction apparatus for clearing the oropharynx, oral airways, equipment to provide intermittent positive pressure ventilation and a supply of oxygen.8 Commercial emergency drug kits are also available, eg the 'Zitapak' (Blackwell Medical).
The recommendations of the 'Poswillo report', published in 1990, have been questioned.9,10 James has suggested that they are beyond the scope of what most dentists are capable: there are 16 drugs and 12 items of 'equipment for resuscitation' which should be available in every practice, but few dentists are competent or experienced in their use. He quoted the narrative: 'they are for use by dentists and doctors fully trained in advanced life support techniques' and wondered where such help could be obtained by the dental practitioner.
McCarthy has argued that preparation for medical emergencies in dentistry has become overcomplicated and guidelines offered by various authorities give scant consideration to the dentist's experience of diagnosis or treatment of such conditions. He suggested that a dentist should have a working knowledge of basic life support, including airway management, a knowledge of diagnosis and treatment of common risk diseases and anaphylaxis and advocated a minimum of emergency drugs and equipment to include: a means of giving positive-pressure ventilation; oxygen; glyceryl trinitrate; adrenaline and sugar or glucose for hypoglycaemia.11
The purpose of this study was to investigate:
-
The emergency drugs and equipment maintained by GDPs
-
The treatment carried out in the management of emergency events they had experienced.
This is the second of three papers on the findings of a questionnaire survey of GDPs in Great Britain. Details of the method, including a copy of the questionnaire, have been reported previously.12
Results
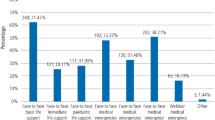
Figure 1 shows the percentage of respondents who possessed each of the 20 items of equipment and emergency drugs specifically asked of in the questionnaire. The majority of respondents had oxygen available (95.4%), yet fewer (91.4%) reported having the means to give it, adrenaline was possessed by 93.3%, an injectable steroid by 86.9% in England & Wales and 91.6% in Scotland. Fewer had a salbutamol inhaler (70.0%), glucose (77.7%), or glyceryl trinitrate (80.1%). There were some statistically significant differences (P < 0.05) between GDPs in England & Wales and Scotland in proportions possessing some items. More respondents in England & Wales possessed nitrous oxide, but more in Scotland possessed an injectable steroid, an intravenous glucose preparation, an aspirator, a tourniquet and flumazenil. Some listed emergency drugs and equipment not specifically asked about in the questionnaire such as a pulse oximeter, lignocaine, atropine and others stated that they possessed the 'Poswillo' recommended drugs.

Percentage of respondents possessing specified items of emergency equipment and drugs in England & Wales and Scotland
Figure 2 shows how they ensured that the drugs they possessed were kept up-to-date (ie within their 'use by' date). Three-quarters of respondents relied on making regular checks on the expiry date of drugs in their emergency kits, while 9% were informed by the supplier of a preparatory emergency drug kit, suggesting that at least this proportion possessed such a kit and 10% were assisted in this by a health authority or some other locally arranged scheme.

How respondents maintained drugs within 'use by' date
Figure 3 shows the percentages of each emergency event not associated with GA where treatment and drugs were used in its management and figure 4 for those associated with GA. Active intervention in the management of non-GA events was most frequent in those associated with diabetes (in 79%), followed by angina pectoris in 69%, cardiac arrest — a much rarer event — in 66% and in 56% of asthma events. The GA events in which active intervention was reported included most cases of anaphylaxis to intravenous agents, in circulatory failure and in respiratory failure. The proportions of respondents carrying out treatment under IS, IVS and GA has been reported previously.12

Percentage of medical emergencies not associated with GA for which treatment or emergency drugs were used in the management of the event

Percentage of medical emergencies associated with GA for which treatment or drugs were administered
Figure 5 shows the proportion of occasions when various procedures and drugs were used in management of the events not associated with GA, where details were given, and figure 6 for those associated with GA. The most commonly used drugs were glucose, in 9.8% of events, mainly in management of diabetic problems, followed by glyceryl trinitrate in 8.6%, predominantly in treatment of angina pectoris: some stated that the patient's own supply was used rather than that held at the practice. An inhaler of some sort was used, in most cases in treatment of asthma, in 8.3% of events. Management of the most frequently reported event, 'fits and seizures', included 'diazepam', 'intravenous diazepam', 'midazolam', 'glucose', 'oxygen', an 'inhaler', 'carbon dioxide' and an 'intramuscular antihistamine'. The latter three were each reported in the management of single episodes.

Percentage of emergency events not associated with GA for which specified procedures and drugs were used

Percentage of emergency events associated with GA for which specified procedures and drugs were used
Table 2 lists the occasions on which cardiopulmonary resuscitation (CPR) and artificial ventilation were performed as part of the management of an emergency event. In England & Wales, CPR was reportedly carried out in management of cardiac arrest, stroke, anaphylaxis and respiratory arrest on 20 occasions and artificial ventilation on four occasions in the management of stroke, anaphylaxis and respiratory arrest. In five of the events where CPR was carried out, the patient was reported to have subsequently died. There were 1383 emergency events reported not associated with GA, thus CPR was carried out in management of 1.4% and artificial ventilation in 0.3% of them. Of the 86 events associated with GA, CPR was carried out in management of four (4.7%) and artificial ventilation of three (3.5%) of them.
In Scotland, CPR was carried out on nine occasions in 793 events reported (1.1%) — only in the management of cardiac arrest and stroke — and six deaths ensued, all following cardiac arrest. However, on three of these occasions, the patients were passers-by to whom assistance was offered by the dental staff and resulted in two deaths, both after cardiac arrest. It was carried out four times (16.0%) and artificial ventilation once (4.0%) in management of 25 GA events. There were no deaths reported in association with GA.
CPR was reported to have been carried out 24 times and artificial ventilation six times over the 6062 years of general practice experience represented in the survey in England & Wales. Thus some form of resuscitation was performed, on average, once in 202 years of practice, representing approximately a 1:5 chance of having to carry this out in a 40-year career. In Scotland, CPR was carried out 11 times in 2789 years (including three times involving the assistance of passers-by), representing one instance for every 253 years of practice, less than a 1:6 chance of having to carry it out in a 40-year career.
Those who provided treatment under GA, IVS or IS were investigated to determine whether they differed, in terms of drugs and equipment they possessed, from those who did not. Those providing treatment under IVS were statistically significantly more likely to possess 17 of the 20 items of emergency drugs and equipment specifically asked of in the questionnaire, including flumazenil, the specific benzodiazepine inhibitor, yet only 50% of this group actually reported possessing this drug. Those providing IS were statistically significantly more likely to possess twelve of the twenty items and those providing GA nine (all P < 0.05). There were no differences in possession of oxygen, the apparatus for delivering air and an oral airway between those who provided any of these treatment modalities and those who did not. Those providing GA and IVS were more likely to have received training as undergraduates and postgraduates in gaining intravenous access and in the use of emergency drugs (P < 0.05).
Discussion
According to the findings of this study, the percentage of GDPs in Great Britain possessing a number of emergency drugs and items of equipment compares favourably with that reported in the recent national survey in Australia.2 In the present study, in excess of 90% of respondents possessed oxygen, compared with 63% in Australia. More than 50% had the means of delivering air (eg by an AMBU bag) and more than 90% had the means of delivering oxygen, compared with 27% in Australia who possessed a 'manual resuscitator' and more than 90% possessed adrenaline in this survey compared with 22% in Australia. That so many more GDPs here possess these items than their counterparts in Australia may well be one of the positive results of the 'Poswillo report'.
Those providing treatment under IVS, might be considered the best prepared group: it is not surprising that this group was more likely to possess a tourniquet and flumazenil, the specific benzodiazepine antagonist, but it is of concern that only 50% of those providing IVS did. The possession of oxygen (by 95.4%), an airway (by 92.5%) and apparatus for delivering air (by 52.7%) is not related to the types of treatment provided indicating that, certainly in the cases of oxygen and an airway, which are possessed by the majority of respondents, there is perhaps a universal realisation of the importance of these items. Possession of these three items and some form of portable aspirator is now considered to be mandatory in a dental practice by the recently revised GDC guidelines.8
Active intervention by the dental team in the management of emergency events was reported most frequently in association with diabetic events, with the administration of glucose orally in most cases but also intravenously (2.0%) and glucagon was also used (0.8%). Active intervention was also prominent in reported cases of angina pectoris, asthma and in the few reported cases of cardiac arrest. However, there appears to have been some confusion as to the diagnosis of a fit or its management as suggested by the treatment reported of this event.
In the Australian study,2 CPR was carried out, on average, once in around seven practising lifetimes (ie in a 40-year career). The results of the present survey indicate a higher frequency, but of a similar order of magnitude, of between once in five and once in six practising life times.
The drugs most commonly used in management of the medical emergencies reported were oral glucose, in 9.8% of reported events, glyceryl trinitrate in 8.6%, an inhaler in 6.3% and oxygen in 4.2%. A ready supply of a glucose substitute is, of course, available as sugar. Glyceryl trinitrate and a salbutamol inhaler may well be possessed by those patients who use them but it seems a reasonable precaution for practitioners to stock them as well, especially as these items were commonly used in the management of the events reported. Oxygen is the one drug which the GDC considers must be available in the dental surgery.
It is of note that half the drugs recommended by the 'Poswillo report' to be available in every dental practice were not actually used in nearly 9000 years of dental practice covered by this survey. This must bring its recommendations into question again. As James pointed out, it is highly unlikely that an emergency event will occur in dental practice in the presence of someone capable of using most of the drugs listed.9 It is also of note that lignocaine and atropine should certainly not be administered without an ECG monitor, which is not recommended to be available in every dental practice. The guidelines in the section of the Dental practitioners' formulary3 entitled 'Medical emergencies in dental practice' omit atropine, lignocaine, aminophylline, calcium chloride, sodium bicarbonate, naloxone and suxamethonium. Indeed, the first line emergency services do not carry as extensive a list as recommended by the 'Poswillo report': Table 3 lists the items carried by the West Yorkshire Metropolitan Ambulance Service.13
A number of respondents articulated the feeling that they were 'damned if they did not possess the Poswillo drugs' and would be 'damned if they used them' without experience in their use or management of complications arising from their use. Others remarked that they had been advised at CPR training courses not to use some of the Poswillo recommended drugs, as to do so without adequate training could lead to prosecution if further complications arose.
Apparently, the recommendations of the 'Poswillo report' for emergency drugs are now considered 'unnecessarily complex'14 and the advice given by the Dental practitioners' formulary is considered more appropriate. It is disappointing that this change of view has not been 'fanfared' to the profession at large as much as were the Poswillo recommendations, for certainly a number of GDPs in 1996, when this survey was carried out, were still labouring under the impression that the Poswillo recommendations were still current.
There appears to be a need for new guidelines on precisely what drugs and equipment for management of medical emergencies GDPs should possess, not least as this may save GDPs the expense of stocking and updating drugs which will never be used. In addition, there have been changes in the Resuscitation Council's guidelines for Advanced Life Support since 1990, when the 'Poswillo report' was published, which have only been tacitly acknowledged in the guidelines to dentists. If GDPs are expected to possess emergency drugs, then clear guidance on indications for their use should be set out, together with routes of administration which are realistically within the capability of a dentist. Any such guidelines should reflect the fact that the dental staff, in an emergency, are trying only to prevent further deterioration in the condition of the patient before transfer to a hospital. It is also important to ensure that training in the use of the drugs and equipment dentists are required to possess should be available.
Conclusions
The majority of respondents possess equipment and drugs which are recommended for use in the management of medical emergencies. Most respondents relied on regular checks on the expiry date of their emergency drugs, but nearly one in ten were reminded by a scheme arranged by the local health authority, and a further one in ten by the supplier of a preparatory kit. The drugs most commonly used in management of the medical emergency events reported were glucose, a salbutamol inhaler, glyceryl trinitrate and oxygen. Yet, the first three items were possessed by only about four out of five respondents. One resuscitation event was reported for approximately every 250 years of practice. Only eight of the 16 drugs recommended by the 'Poswillo report' to be available in every dental practice, namely oxygen, adrenaline, glyceryl trinitrate, salbutamol, chlorpheniramine, dextrose, hydrocortisone and midazolam were used in more than 8000 years of practice. In view of this, the guidelines for drugs which are to be available in a dental surgery for the management of a medical emergency should be revised to reflect what dentists feel capable of using and for which formal training is available in an organised manner.
References
Shirlaw P J, Scully C, Griffiths M J, Levers B G H, Woodwards R T M . General anaesthesia, parenteral sedation and emergency drugs and equipment in general dental practice. J Dent 1986; 14: 247–250.
Chapman P J . Medical emergencies in dental practice and choice of emergency drugs and equipment: a survey of Australian dentists. Aust Dent J 1997; 42: 103–108.
British Dental Association, British Medical Association, Pharmaceutical Society. Dental practitioners' formulary 1996–1998, together with the British national formulary No 32 (September 1996). BMA & Pharmaceutical Press, 1996.
Craig D, Debuse D, Skelly M . The dental team — management of medical emergencies. Focus (Journal of the Dental Defence Union) 1995; 1: 6–12.
Crosby A C . In Figures K H and Lamb D J (Eds) Primary and emergency dental care. A practitioner's guide. Oxford: Wright, 1995.
Scully C, Cawson R A . In Medical problems in dentistry. p550. 3rd ed. Bristol: Wright, 1993.
Poswillo D E (Chair). Standing Dental Advisory Committee. General anaesthesia, sedation and resuscitation in dentistry: report of an expert working party. London: HMSO, 1990.
General Dental Council. Maintaining standards — guidance to dentists on professional and personal conduct. London: General Dental Council, November 1997.
James D W . General anaesthesia, sedation and resuscitation in dentistry. Br Dent J 1991; 171: 345–347.
Macpherson L M D, Binnie V I . A survey of general anaesthesia, sedation and resuscitation in general dental practice. Br Dent J 1996; 181: 199–203.
McCarthy F M . Emergency drugs and devices — less is more. CDA J 1993; 21: 19–25.
Atherton G J, McCaul J A, Williams SA . Medical emergencies in general dental practice in Great Britain. Part I: their prevalence over a 10-year period. Br Dent J 1999; 186: 72–79.
Personal communication: E J Whitely, Station Officer, West Yorkshire Metropolitan Ambulance Service, 5.3.97.
Personal communication: General Practice Department, British Dental Association, London, 27.8.98.
Author information
Authors and Affiliations
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
Atherton, G., McCaul, J. & Williams, S. Medical emergencies in general dental practice in Great Britain Part 2: drugs and equipment possessed by GDPs and used in the management of emergencies. Br Dent J 186, 125–130 (1999). https://doi.org/10.1038/sj.bdj.4800040
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4800040
This article is cited by
-
Letters
British Dental Journal (2000)
-
Most dentists have the drugs and equipment required for managing medical emergencies
British Dental Journal (1999)
