
Abstract
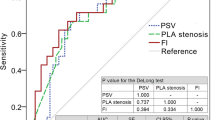
Erection is a hemodynamic event and accordingly, erectile dysfunction (ED) is closely related with ischemic heart disease. We should confirm that the cardiac condition of the ED patient is safe enough to perform sexual intercourse prior to beginning treatment for ED. Asymptomatic ischemic heart disease cannot be diagnosed only in an interview, but it's difficult to perform cardiac exercise tests on all patients complaining of ED. Therefore, screening methods to evaluate patients who should undergo exercise tests are needed. Sixty patients with erectile dysfunction participated in this study. Physical examinations, interviews, and color Doppler examinations were conducted. Chest X-rays and electrocardiograms of all patients in the resting position were obtained, as were electrocardiograms following exercise. Echocardiograms, treadmill test results, thallium exercise scintigrams, and coronary angiograms were obtained as required for diagnosis. Two patients were excluded because they had obvious arteriogenic ED due to perineal injury. Fifty-eight patients underwent Doppler evaluations of their cavernous arteries and heart exercise tests. Fourteen patients (24.1%) were diagnosed with ischemic heart disease. Although six of them had already been diagnosed with ischemic heart disease, eight were newly diagnosed by the exercise tests. Cardiovascular risk factors such as advanced age, hyperlipidemia, diabetes mellitus, hypertension, smoking, and obesity were not sufficient predictive factors. The mean peak systolic velocity of the patients without ischemic heart disease was 34.6 cm/s vs 22.0 cm/s in those with ischemic heart disease. Only 3.7% of patients whose peak systolic velocity in the cavernous artery was equal to or exceeded 35 cm/s had ischemic heart disease. On the other hand, 41.9% of patients with peak systolic velocity of less than 35 cm/s had ischemic heart disease. The sensitivity of peak systolic velocity against ischemic heart disease was 92.9%, and specificity was 59.1%. In ED patients, incidences of complications involving symptomatic or asymptomatic ischemic heart disease were found to be high. The peak systolic velocity in the cavernous artery is thought to be a useful predictive factor of ischemic heart disease in ED patients. When a patient reveals a peak systolic velocity of less than 35 cm/s, he should undergo heart exercise tests prior to treatment of ED.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 8 print issues and online access
$259.00 per year
only $32.38 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Muller JE et al.Triggering myocardial infarction by sexual activity. Low absolute risk and prevention by regular physical exertion. JAMA 1996 275, 1405–1409.
Muller JE. . Sexual activity as a trigger for cardiovascular events: what is the risk? Am J Cardiol 1999 84, 2N–5N.
Mittleman MA et al.Triggering of acute myocardial infarction by heavy physical exertion. Protection against triggering by regular exertion. Determinants of Myocardial Infarction Onset Study Investigators. New Engl J Med 1993 329, 1677–1683.
Master AM, Rosenfeld I. . Criteria for the clinical application of the ‘Two-step’ exercise test. JAMA 1961 178, 283–298.
Fletcher GF et al.Exercise standards. A statement for healthcare professionals from the American Heart Association. Circulation 1995 91, 580–615.
Conti CR, Pepine CJ, Sweeney M. . Efficacy and safety of sildenafil citrate in the treatment of erectile dysfunction in patients with ischemic heart disease. Am J Cardiol 1999 83, 29C–34C.
Kloner RA, Jarow JP. . Erectile dysfunction and sildenafil citrate and cardiologists. Am J Cardiol 1999 83, 576–582.
Kloner RA, Zusman RM. . Cardiovascular effects of sildenafil citrate and recommendations for its use. Am J Cardiol 1999 84, 11N–17N.
Wespes E et al.Corporeal veno-occlusive dysfunction: a dorsal arterial pathology? J Urol 1998 160, 2054–2057.
Azadzoi KM, Siroky MB, Goldstein I. . Study of etiologic relationship of arterial atherosclerosis to corporal veno-occlusive dysfunction in the rabbit. J Urol 1996 155, 1795–1800.
Greenstein A et al.Does severity of ischemic disease correlate with erectile function? Int J Impot Res 1997 9, 123–126.
Porter A et al.Acute myocardial infarction following sildenafil citrate (Viagra) intake in a nitrate-free patient. Clin Cardiol 1999 22, 762–763.
Drory Y, Kravetz S, Florian V, Weingarten M. . Sexual activity after first acute myocardial infarction in middle-aged men: demographic, psychological and medical predictors. Cardiology 1998 90, 207–211.
Drory Y, Shapira I, Fisman EZ, Pines A. . Myocardial ischemia during sexual activity in patients with coronary artery disease. Am J Cardiol 1995 75, 835–837.
Bohlen JG, Held JP, Sanderson MO, Patterson RP. . Heart rate, rate–pressure product, and oxygen uptake during four sexual activities. Arch Intern Med 1984 144, 1745–1748.
Feenstra J, van Drie-Pierik RJ, Lacle CF, Stricker BH. . Acute myocardial infarction associated with sildenafil. Lancet 1998 352, 957–958.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kawanishi, Y., Lee, K., Kimura, K. et al. Screening of ischemic heart disease with cavernous artery blood flow in erectile dysfunctional patients. Int J Impot Res 13, 100–103 (2001). https://doi.org/10.1038/sj.ijir.3900642
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ijir.3900642
Keywords
This article is cited by
-
Evaluation of arterial stiffness and cardiac function in patients with vascular erectile dysfunction: acute effects of phosphodiesterase-5 inhibitor tadalafil
International Journal of Impotence Research (2017)
-
Erectile Dysfunction in the Elderly
Current Geriatrics Reports (2015)
-
Pharmaco-écho-doppler pénien: méthodologie, critères diagnostiques et indications actuelles dans l’exploration d’une dysfonction érectile
Basic and Clinical Andrology (2012)
-
Comparison of the differences in circadian autonomic function in hyperlipidemic men with and without erectile dysfunction
International Urology and Nephrology (2010)
-
Metabolisches Syndrom und erektile Dysfunktion
Der Urologe (2007)
