
Abstract
Study design:
Case report describing the management of repeated perioperative bleeding probably due to Protein-Z-deficiency in a post-traumatic paraplegic patient.
Objectives:
To describe the difficulty in diagnosing this rare form of hypocoagulability and the monitoring and substitution concept during three elective surgical interventions.
Setting:
Spinal Cord Injury Center, Bergmannstrost, Halle, Germany.
Case report:
A 19-year-old male suffering from a post-traumatic paraplegia sub Th8 (ASIA-A) since childhood had experienced two life-threatening intraoperative bleeding incidents before finally Protein-Z-deficiency as the underlying coagulation disorder was diagnosed. After substitution of 2000 IE PPSB (Beriplex P/N) a repeatedly postponed implantation of a sphincter-externus (Brindley-) stimulator could be performed without bleeding complications, and this was also true for two additional urological interventions 1 year later. Protein-Z levels were monitored before, during and after the operations. The preoperative application of between 1000 and 2000 IE PPSB was safe and sufficient to raise the patients' plasma Protein-Z level to almost normal and so prevent excessive intraoperative blood loss.
Conclusion:
In case of repeated bleeding tendency of unknown origin it is mandatory to look for rare causes of hypocoagulability such as Protein-Z-deficiency. We developed a substitution concept using a plasma concentrate with guaranteed Protein-Z amount (PPSB) allowing the safe performance of elective surgical interventions.
Similar content being viewed by others
Introduction
Protein-Z-deficiency is one of the rare causes of unexpected perioperative bleeding. This hypocoagulability is not covered by usual preoperative coagulation tests, and this diagnosis is often missed or finally made after a surgical intervention, when an inadequately heavy loss of blood has occurred. The exact analysis of Protein-Z-deficiency can only be made by a micro-ELISA method using monoclonal antibodies, which is only available in specialized laboratories. A preoperative screening of patients with a history of enhanced bleeding for Protein-Z-deficiency does not seem to be adaequate due to the low incidence of this disorder. Therefore, the measurement of Protein-Z level is usually restricted to a small number of patients with special problems. Nevertheless an investigation of cases with repeated bleeding incidents of unknown origin during and after surgery has demonstrated decreased concentrations of Protein-Z in about 50% of the patients.1
If there is evidence of Protein-Z-deficiency in a patient with repeated bleeding, the whole range of preventive measures must be initiated.
Case report
A 19-year-old male was hit by a car on his way to school in 1993. Besides other severe injuries he suffered from a fracture of the 11th and 12th thoracic vertebral body resulting in paraplegia below Th 8 (ASIA-A). He developed a neurogenic scoliosis accompanied by a restrictive ventilatory capacity.
In 1998, a correction operation in order to reduce skoliosis and improve lung function was carried out. It had to be stopped before successful spondylodesis because of massive bleeding requiring the transfusion of 10 erythrocyte concentrates, 3.5 l autologous blood transfusions, 12 U fresh frozen plasma (FFP) and two thrombocyte concentrates. As extended analysis did not reveal a plasmatic or thrombocytic disorder a second intervention to complete the corrective osteotomy was performed in the same year. The intraoperative problems recurred with profuse blood loss, again consuming several FFPs, five erythrocyte concentrates and autologous blood.
Coagulation tests were redone and completed by the measurement of single coagulation factors, reptilase time, bleeding time, thrombocyte function tests (ie PFA 100, Rotec), v. Willebrand factor, v. Willebrand antigen, plasminogen, alpha2-antiplasmine, cardiolipin antibodies and tPA, all of them being within the normal range. Only the measurement of Protein-Z level, which was carried out in this patient for the first time, showed a reduced concentration of 716 μg/l (normal range above 1500 μg/l).
In 1999, another spinal cord operation to implant an anterior nerve root stimulator of the urinary bladder (ie Brindley stimulator) was considered necessary because of repeated infections of the urinary tract, but it was postponed because of the increased bleeding tendency of the patient. In March 2001, the intervention was considered to be inevitable.
The renewed extensive preoperative testing again did not demonstrate a coagulation defect but showed a low level of plasma Protein-Z of 520 μg/l.
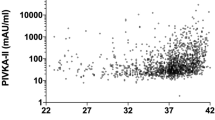
Immediately before the operation the patient received 2000 IE PPSB (Beriplex P/N) intravenously. Protein-Z, which was measured intraoperatively, was raised to a physiological level of 2520 μg/l (Figure 1). During the whole intervention of 5 h no extraordinary bleeding occurred, the concentrates of coagulation factors, blood preparations and antifibrinolytic medicaments, which had been kept ready, were not necessary, neither intra- nor postoperatively.

Pre-, intra- and postoperative plasma levels of Protein-Z under substitution of 2000 IE PPSB (2001) and 1000 IE PPSB each (2002) during surgical interventions of the paraplegic patient
In 2002, another urological intervention was necessary (ureterotomia interna and a WINKELMANN hydrocele resection) because of a hydrocele of the size of a fist of the right testicle due to an ascending epididymorchitis. According to a preoperative Protein-Z level of 440 μg/l the patient was supplied with only 1000 IE PPSB, because the bleeding risk was significantly lower this time. This achieved an increase of Protein-Z throughout the operation of 2 h ranging between 1200 and 1380 μg/l (Figure 1) and was also sufficient for the postoperative period. Again, no bleeding complications were reported.
In August 2002, the patient safely underwent a resection of the right epididymis under the same substitution regimen, which resulted in an intraoperative Protein-Z level >1000 μg/l.
Discussion
Protein-Z is a vitamin-K-dependent plasma glycoprotein with a molecular weight of 62 000 Da.1 The sequence of amino acids of human Protein-Z was resolved in 1990,2 the corresponding gene lying on chromosome 13.3
Protein-Z is synthesized in the liver like most of the coagulation factors – and shows great structural similarities with other vitamin-K dependent coagulation factors such as factor II, IX, X and Protein C and S. The mean plasma concentration of Protein-Z of adults was found to be between 1500 and 3000 μg/l, the levels of babies and younger children range below 1500 μg/l.4, 5, 6 The half-life time in plasma is about 2.5 days.4
Protein-Z seems to assist haemostasis by binding thrombin and promoting its association with phospholipid surfaces, and it downregulates coagulation by forming a complex with the plasma Protein-Z-dependent protease inhibitor, which inhibits activated factor Xa.7, 8 From this it can easily be deduced, that in cases with – hereditarily caused – Protein-Z-deficiencies an increased bleeding tendency may occur, especially when the coagulation system experiences extreme challenges, such as during surgical interventions.
There are also some indications that in plasma only a fraction of the Protein-Z pool existing in the organism is measurable; higher concentrations seem to be found in proliferating vascular endothelium.9 Therefore, it has been suggested, that high Protein-Z levels might be a risk factor for ischaemic strokes.10 The highest Protein-Z concentrations so far have been measured in patients dependent on haemodialysis.11 Patients with homozygotic factor-V-disease mutation, however, combine low Protein-Z levels with an increased procoagulation potential.12 These examples may shed some light on the ambivalent function of some factors in many coagulation defects caused by the inherent complexity of the regulation systems.
The low amount and small number of cases of scientific investigations concerning the impact of Protein-Z on bleeding incidents of unknown origin lead to different results and interpretations. Some authors assume, on the basis of serial investigations in patients with unexplained haemorrhagia, that Protein-Z does not play an important role in the explanation of bleeding tendencies.13, 14 In contrast to this Gross and co-workers concluded from the examination of two families with increased bleeding tendency that low Protein-Z levels could exacerbate originally mild bleeding disorders.15 According to Kemkes-Matthes and Matthes1 over 50% of patients with recurrent bleeding incidents showed diminished levels of Protein-Z when other coagulation defects had been excluded. Moreover, they found a correlation between the severity of bleeding complications and the exact level of Protein-Z (they investigated oral and cardiosurgical interventions and patients undergoing adenotomies and tonsillectomies).16, 17, 18 A plasma level below 1000 μg/l was combined with a significant increase of intraoperative blood loss.
In 1995, Greten and co-workers described a female patient with previous severe intraoperative bleeding which occurred at a Protein-Z level of 600 μg/l.9 Under substitution of a prothrombin complex concentrate containing Protein-Z an acute cholecystectomy could be performed without bleeding complications later. The same observation was reported recently from Kemkes-Matthes and Matthes concerning a further patient with a preoperative Protein-Z level of about 500 μg/l, where a sufficient perioperative haemostasis could be achieved with the same regimen.5
Our case confirms these observations and shows that elective surgical interventions can be performed safely under an adequate compensation of the coagulation defency.
Protein-Z is not available as a single factor for substitution therapy, but it is represented in PPSB-concentrates in a concentration between 70 and 200 μg/ml. Comparative analyses have shown different levels of Protein-Z in different preparations of coagulation factor concentrates.19 An adequate substitution for patients with documented Protein-Z deficiency using fresh-frozen-plasma is not practicable and tolerable because of the enormous volumetric load.
The PPSB dose regimen so far is based on experience derived from few case reports and implies a dosage, that in extensive operations with high-bleeding risk the Protein-Z level ideally should be raised to the upper physiological range. Based on initial values between 500 and 700 μg/l this can normally been achieved by the preoperative application of 2000 IE PPSB (Beriplex P/N from Aventis-Behring, now ZLB-Behring). PPSB is the only preparation so far where data concerning Protein-Z concentration are available.19
The case described by our group adds further information to these experiences because the pre-, intra- and postoperative measurements of Protein-Z here could give proof of the sufficiency of the substitution of Protein-Z using PPSB throughout the whole ‘sensitive phase’. Furthermore, the applied doses lying between 1000 and 2000 IE PPSB can serve as a practical guide-line for the safe planning of surgical interventions under these preconditions in the future. For interventions with a somewhat lower bleeding risk the application of 1000 IE PPSB is sufficient, because it reaches a preventive plasma level of above 1000 μg/l, as shown in our case. The indication for repeated applications of Protein-Z containing preparations during one session must be made individually depending on the kind and duration of the intervention and regarding the obvious blood loss, as in this case laboratory results of the actual Protein-Z level usually are not at hand.
References
Kemkes-Matthes B, Matthes KJ . Protein Z Deficiency: a new cause of bleeding tendency. Thromb Res 1995; 79: 49–55.
Ichinose A, Takeya H, Espling E, Iwanaga S, Kisiel W, Dawie EW . Amino acid sequence of human protein Z, a vitamin K-dependent plasma glycoproteine. Biochem Biophys Res Commun 1990; 172: 1139–1144.
Fujimaki K, Yamazaki T, Taniwaki M, Ichinose A . The gene for human protein Z is located to chromosome 13 at band q34 and is coded by eight regular exons and one alternative exon. Biochemistry 1998; 37: 6838–6846.
Miletich JP, Broze GJ . Human plasma protein Z antigen: range in normal subjects and effects of warfarin therapy. Blood 1987; 69: 1580–1586.
Kemkes-Matthes B, Matthes KJ . Rolle von Protein Z in der Blutgerinnung. Med Welt 2000; 11321–11325.
Kemkes- Matthes B, Hammermann H, Rettig-Gammler A, Wozniak G, Matthes KJ . Age-dependency of Protein Z concentration. Ann Hematol 2000; 79: A99.
Han X, Fiehler R, Broze GJ . Characterization of the protein Z-dependent protease inhibitor. Blood 2000; 96: 3049–3055.
Hogg PJ, Stenflo J . Interaction of vitamin K-dependent protein Z with thrombin. J Biol Chem 1991; 266: 10953–10958.
Greten J, Kemkes-Matthes B, Nawroth PP . Prothrombin complex concentrate contains protein Z and prevents bleeding in a patient with protein Z deficiency. Thromb Haemost 1995; 74: 992–993.
Kobelt K, Bisiutti D, Mattle HP, Lämmle B, Wuillemin WA . Protein Z in ischemic cerebrovascular disease. (ICVD). Ann Hematol 2000; 79: A41.
Usalan C, Erdem Y, Altum B . Protein Z levels in hemodialysis patients. Int Urol Nephrol 1999; 31: 541–545.
Kemkes-Matthes B, Matzdorf A, Matthes KJ . Protein Z influences prothrombotic phenotype of factor V Leiden in humans. Blood 2000; 96: 534a.
Ravi S, Mauron T, Lämmle B, Wuillmin W . Protein Z in healthy individuals and in patients with a bleeding tendency. Br J Haematol 1998; 102: 1219–1223.
Gamba G, Bertolino G . Bleeding tendency of unknown origin and protein Z levels. Thromb Res 1998; 90: 291–295.
Gross J, Petrescu-Jipa M, Dobonici M, Stephan B, Pindur G, Seyfert UT . Prothrombin complex concentrate in the perioperative management of a 71-year-old woman with protein Z deficiency. German Association of Thrombosis and Haemostaseology, Annual Conference 2004, abstract.
Kemkes-Matthes B, Rettig-Gammler A, Hoerster W, Matthes KJ . Plasma-Protein-Z Verminderung – Perioperatives Blutungsrisiko bei kieferchirurigischen Eingriffen. In: Scharrer I, Schramm W. (Hrsg.) Hämophilie-Symposium 1997. Springer: Hamburg 1999; 468–470.
Kemkes-Matthes B, Hammermann H, Glanz H, Matthes KJ . Correlation between blood loss and protein Z levels in tonsillectomy and adenotomy. Ann Hematol 2000; 79: A63.
Kemkes-Matthes B, Wozniak G, Bauer J, Matthes KJ . Protein Z in cardiac surgery. Ann Hematol 1998; 76: A84.
Römisch J, Bonik K, Diehl KH, Müller HG . In-vitro Vergleich von PPSB-Konzentraten. Krankenhauspharmazie 1997; 18: 124–127.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Röhl, K., Jäger, D. & Barth, J. Protein-Z-deficiency as a rare case of unexpected perioperative bleeding in a patient with spinal cord injury. Spinal Cord 44, 636–639 (2006). https://doi.org/10.1038/sj.sc.3101897
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101897
