
Abstract
Study design:
Randomized controlled trial.
Objectives:
To establish whether the use of mechanical insufflation/exsufflation leads to a significant improve in tracheostomy subjects with upper spinal cord injuries (C1–C7), ASIA classification grade A and bronchial hyper secretion the following parameters: forced vital capacity (FVC), forced exspiratory volume on the first second (FEV1), FEV1/FVC, peak exspiratory flow (PEF), arterious pressure of O2 (Pa O2), arterious pressure of CO2 (Pa CO2), pH, saturation of O2 (Sa O2).
Setting:
Spinal Cord Unit, Montecatone Rehabilitation Institute, Imola, Italy.
Methods:
The patients were split into two groups: the experimental group (EG) and the control group (CG). Each patient was given 10 treatments: the EG was given manual respiratory kinesitherapy associated with mechanical insufflation/exsufflation with inhale and exhale pressure between 15 cm H2O and 45 cm H2O, while the CG was only given manual kinesitherapy. The treatment sessions covered the necessary amount of time in order to achieve sufficient clearance. The study has been approved by the local ethic committee. The patients were informed before being enrolled in that study and gave their written consent.
Results:
At the end of the treatment associated with the mechanical insufflation/exsufflation, the EG showed a significant increase in FVC, FEV1 and PEF, although it was not possible to compare the latter with the CG. The other parameters were also subject to variations, although not statistically significant. The CG did not show signs of any significant change.
Conclusion:
The use of mechanical insufflation/exsufflation in subjects with the aforementioned characteristics is shown to be an effective adjunct to manual respiratory kinesitherapy, since it makes it possible to achieve adequate bronco-pulmonary clearance, even removing thick, deep secretions and making it possible to insufflate any areas affected by atelectasis.
Similar content being viewed by others


Introduction
Respiratory problems are one of the main complications found in patients with upper spinal cord injury. Respiratory kinesitherapy is an effective weapon to combat pulmonary complications that arise following the sputum retention, forced immobility, mechanical ventilation and tracheostomy. Those who have a cervical spinal cord injury are particularly susceptible to Restrictive Syndrome, marked by the decrease of all respiratory volumes and flows.1 The peak cough expiratory flow (PCEF) in particular falls below 3 l/s, which is necessary to produce an effective cough.2 The inefficiency of the cough in upper spinal cord lesions is one of the main factors that causes sputum retention; therefore one of the main aims of respiratory kinesitherapy is to generate a PCEF that can enable the removal of secretions. In order to achieve this goal, the therapists can use manually assisted coughing, other manual clearance methods and mechanical insufflation and exsufflation.
Our study aims to establish whether the use of mechanical insufflation and exsufflation has a greater effect on respiratory volumes and flows than manual bronchial clearance.
Materials and methods
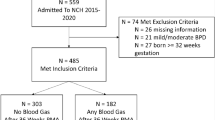
The inclusion criteria was cervical spinal cord injury (C1–C7) with ASIA classification grade A, tracheostomy and bronchial hyper secretion.
Each patient was given 10 treatments, except two patients from the control group (CG), who were given six and nine treatment sessions respectively, using bronchial clearance methods consisting of postural drainage, uPEP, assisted coughing, Ambu bag, endoscopic bronchoaspiration. The experimental group (EG), who used the Cough Assist Mechanical In-Exsufflator by Emerson, was also given a maximum of five additional cycles of a maximum of five insufflations/exsufflations per cycle, alternating with short breaks (max 3 min) after each cycle, in a semiseated position (35–40°); we set the mechanical insufflation/exsufflation device in automatic mode using the following parameters:
-
Inhale: 2 s;
-
Exhale: 3 s;
-
Pause: 0.5 s;
-
Inhale flow: maximum;
-
Pressure: minimum 15 cm H2O, maximum 45 cm H2O, always starting from the minimum pressure in order to give the patient time to adjust to the instrument.
The average age of the CG was 52.2±17.6 years old; that of the EG was 31.5±16.1 years old, but this difference was not significant (P=0.273).
The study has been approved by the local ethic committee. The patients were informed before being enrolled in that study and gave their written consent.
Results
Sex was similarly distributed in the two groups: 80% of the EG was male and 20% female, while the CG was 75% male and 25% female, with P=0.317.
The ventilation method (Mechanical Ventilation or Spontaneous Breathing) was thus distributed in the two groups:
-
80% SB and 20% MV in the EG
-
50% SB and 50% MV in the CG.
The P was equal to 1 and therefore insignificant.
The difference in the extent of injury between the two groups was represented by P=0.102 and therefore there was no significant difference.
As our final consideration, we looked at the tobacco addiction factor: we found that 60% of the EG were exsmokers and 40% nonsmokers, while 25% of the CG were exsmokers and 75% nonsmokers. Once again, the P is insignificant (P=0.157). Before the first treatment and at the end of the last treatment session, we performed the analysis of artery blood on every patient in order to record the Pa O2, Pa CO2 and pH values; we monitored the Sa O2 value before and after each treatment session using the pulse oxymeter; we also performed three spirometry tests before and after each session, as indicated by the American Thoracic Society (ATS), in order to check the values of FVC, FEV1, FEV1/FVC and PEF.
The study data was processed using the nonparametric Wilcoxon test. In the EG, treated with mechanical insufflation and exsufflation, two parameters increased significantly: the FVC and the FEV1, with respective percentage increases of 24% (from 0.37±0.23 l to 0.46±0.21 l) and 33% (from 0.21±0.15 l to 0.28±0.14 l) (P=0.0001). The other parameter that shows a significantly increase, (P=0.0093), is the PEF (from 0.24±0.19 l/s to 0.31±0.19 l/s); however, the PEF of the two groups cannot be compared because the PEF average final value of the EG is lower than the PEF average starting value of the CG.
In the CG, there was no significant change in any of the parameters taken into consideration; when compared to the significantly different EG parameters, the FVC increases by 0%, while the FEV1 actually decreases by 3.7%. The objection could be raised that the small number of patients treated could discredit the validity of the significant variation in the FVC and the FEV1; however, the fact that P=0.0001 is so much lower than 0.01 means that this variation could not be due to chance.
The FEV1/FVC also tends to increase in the EG (+14%), but this is not statistically significant.
In the CG, we observed that the FEV1/FVC decreased slightly (−4/65%), but the P is not significant (0.92).
We find an increase in blood gas values and the O2 value after treatment in both groups, with the exception of the decreasing Pa CO2; however, these signs of improvement are not significant results: for PaO2, SaO2 and pH in the EG.
Discussion
The FVC and FEV1 of the EG increased significantly with respect to the CG. This means better ventilation for the patient and compliance maintenance thanks to the mechanical action of the mechanical insufflation/exsufflation. However, the improved ventilation did not mean a significant improvement in perfusion, as shown by the blood gas parameters (Table 1).
The increase in FEV1 meant an improvement in the capacity to expel air by force; the increase of this flow may be due to better clearance and compliance maintenance, and not to the increased strength of the muscles used during exhalation and inhalation: with the same strength the patient is able to inhale and exhale a greater volume of air, as the airways are free from secretion; the same stands for the FVC. The only research that looked at the effect of mechanical insufflation/exsufflation in patients with upper spinal cord injuries was carried out by Dr Bach.3 In a study carried out on 46 ventilator assisted patients suffering from neuromuscular diseases, he found a significant increase in the FVC and the PEF, especially in the five patients with spinal cord injuries, which underwent respective increases from 478±289 ml to 616±292 ml (+29%) and from 2.63±0.75 l/s to 2.87±0.72 l/s (+9%); he also recorded a significant increase in the FEF 25–75% and the PCEF. The results of this study confirm our results.
Conclusion
On the basis of our results and observations made during the study, we believe that it is important to continue with this work through further exploration in order to establish whether weaning in ventilator assisted patients may be significantly reduced by using mechanical insufflation and exsufflation, with respect to the simple administration of manual techniques. During this future research, I propose to monitor the vital capacity following the same methods used in the experiment described herein: I believe that it is effectively very useful to randomize two groups of nonventilator assisted patients and, then, monitor their vital capacity during the weaning trials.
It could also be very interesting to carry out a further study aimed at establishing whether secretion control through mechanical insufflation and exsufflation could reduce tracheostomy tube weaning times in patients who are able to breath spontaneously.
In conclusion, we can affirm that the use of a mechanical insufflation and exsufflation device, during intensive and postintensive care, is without doubt effective since, while maintaining optimal ventilation in these patients, it could reduce the number of fibrobronchoscopy and bronchoaspiration operations, with a probable reduction in respiratory complications and improved general conditions. It could reduce tracheostomy tube weaning times and, consequently, also hospital stay times, thereby increasing the number of early discharges from hospital, leading to an indisputable improvement in patient quality of life and cost reductions for the hospital.
References
De Troyer A, Borenstein S, Cordier R . Analysis of lung volume restriction in patients with respiratory muscle weakness. Thorax 1980; 35: 603–610.
Bach JR et al. Airway secretion clearance by mechanical exsufflation for post poliomyelitis ventilator assisted individuals. Arch Phys Med Rehabil 1993; 74: 170–177.
Bach JR . Mechanical insufflation-exsufflation. Comparison of peak expiratory flow with manually assisted and unassisted coughing techniques. Chest 1993; 104: 1553–1621.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Pillastrini, P., Bordini, S., Bazzocchi, G. et al. Study of the effectiveness of bronchial clearance in subjects with upper spinal cord injuries: examination of a rehabilitation programme involving mechanical insufflation and exsufflation. Spinal Cord 44, 614–616 (2006). https://doi.org/10.1038/sj.sc.3101870
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101870
Keywords
This article is cited by
-
The immediate effects of breathing with oscillated inspiratory and expiratory airflows on secretion clearance in intubated patients with cervical spinal cord injury
Spinal Cord (2019)
-
Preliminary experience on the safety and tolerability of mechanical “insufflation-exsufflation” in subjects with artificial airway
Intensive Care Medicine Experimental (2018)
-
Benefits of interventions for respiratory secretion management in adult palliative care patients—a systematic review
BMC Palliative Care (2016)
-
The acute respiratory management of cervical spinal cord injury in the first 6 weeks after injury: a systematic review
Spinal Cord (2011)
