
Abstract
Study design:
A retrospective analysis.
Objectives:
To examine the natural history of renal scarring in the spinal cord injured population.
Setting:
United Kingdom.
Methods:
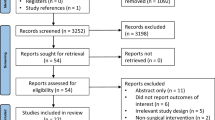
All spinal cord injured patients with renal scars at our establishment were considered eligible. A total of 27 patients with renal scars were identified. No patient had renal scarring at presentation on radiological imaging. All patients had annual renal imaging with a mean follow up period of 19.1 years. The presence of new scars was considered as evidence of progression.
Results:
In all, 59% of kidneys developed renal scars with a mean time interval between spinal injury and renal scar development of 13 years. Of these kidneys with scars, only 15.6% demonstrated progression of the scarring process. There were no deaths due to renal causes.
Conclusion:
The aetiology of renal scarring is multifactorial. The findings of this study suggest that renal scarring in the spinal cord injured population is predominantly a nonprogressive process once a scar has developed. This is in concordance with the belief that renal scarring in the paediatric population with vesicoureteric reflux is also a stable, nonprogressive process.
Similar content being viewed by others


Introduction
The management of the bladder sequelae of spinal cord injury (SCI) continues to be a controversial issue. The main options consist of clean intermittent catheterization (CIC), continuous bladder drainage via an indwelling urethral catheter or suprapubic catheter, sphincterotomy with condom catheter or urinary diversion. The choice of bladder management is determined by the objective urodynamics of the bladder, patient mobility, ability to perform CIC and various other parameters. Over the last 3–4 years, the management of the lower urinary tract has been based on the belief that the maintenance of a low residual urine volume in the bladder leads to a low pressure bladder system, which in turn reduces the risk of renal injury and deterioration in function. However, studies performed as early as the 1950s have found that chronic renal inflammation can be demonstrated in 65–95% of SCI patients with long term indwelling catheters at post-mortem examinations.1 Much more recently, it has been shown that chronic catheterization in SCI patients seems to be associated with a higher incidence of renal scarring and caliectasis.2 Furthermore, contrary to previous belief, the use of an indwelling catheter does not necessarily result in a constantly low intravesical pressure.3 In fact, there is urodynamic evidence that phasic detrusor contractions persist despite chronic catheterization and that such situations have an association with increased renal scarring. In light of this evidence, we have studied our population of patients with SCI with evidence of renal scarring in order to determine whether the development of such scars constitutes a solitary event or is a progressive process in the affected renal unit.
Patients and methods
The study population consisted of all patients with SCI at the Pinderfields Hospital Regional Spinal Injuries Unit. The criterion for inclusion in the study was the demonstration of persistent renal scarring on upper urinary tract imaging in SCI patients in whom provisional renal imaging at the time of injury demonstrated no evidence of scarring. In total, 27 patients were eligible for the study. The mean age of the patients was 61.5 years (range 38–84 years). Patient's demographic details are summarized in Table 1. There were 13 cervical cord injuries, 12 dorsal cord injuries and two lumbar cord injuries, with renal scarring in 32 renal units. Renal imaging was by regular IVU up until the late 1980s, after which annual ultrasonography became the investigation of choice for the detection of renal scarring. The sensitivity of renal ultrasonography when compared to dimercaptosuccinic acid scintigraphy (DMSA) is acceptable4 and in SCI patients ultrasonography is a reliable method of renal scar detection.5 The time interval between the occurrence of the spinal injury and the detection of the first renal scar was recorded. A scar was considered to be persistent if it was unequivocally demonstrated on at least one future subsequent imaging study. The appearance of additional scars or diffuse scarring within a renal unit was recorded as being indicative of progression of the scarring process, provided such progression could be demonstrated on future imaging studies. The main method of bladder drainage for each patient was recorded as either involving the use of an indwelling catheter for a continuous period greater than 50% of the time (urethral or suprapubic) or free of an indwelling catheter (voiding on urge, CIC, condom catheter drainage, urinary diversion).
Various independent variables were analysed to assess their influence on the occurrence and progression of renal scarring. These included patient's age, level of spinal injury, method of bladder drainage and interval between spinal injury and detection of renal scarring. Analysis, where appropriate, was by the Student's t-test or Fischer's Exact test with a level of P<0.05 taken for significance.
Results
A total of 54 renal units in 27 patients were examined, with a mean follow-up period of 19.1 years (range 4–38 years). In these renal units, there was evidence of scarring in 59.3%, which was not evident at or soon after the time of the spinal injury. Of the renal units with scarring, 84.4% were static in nature with only 15.6% demonstrating progression of the scarring process (Figure 1).

Type of renal scarring
There was no difference between the ages of the patients demonstrating static scarring and those with progressive scarring (mean 57.8 versus 57.2 years, respectively). The level of SCI was evenly distributed between cervical and thoracic injuries, with only two lumbar injuries (Table 2). The mean time interval between the SCI and the development of renal scarring was 13.0 years (range 1–33 years; Figure 2). There was no particular correlation between the occurrence of renal scarring and the time interval between the SCI and the development of the scarring (Figure 3). Two deaths occurred during the study period: one from myocardial ischaemia and the second from late-stage bladder cancer. There were no deaths attributable to renal causes.

Renal scarring and mean time to scar development

Time interval between SCI and renal scar development
The patients with static renal scarring were equally distributed between the catheter free and catheterized groups (Table 3). However, all the patients with progressive renal scarring used indwelling catheterization as the main method of bladder drainage, although no significant positive correlation between catheterization and progressive scarring was demonstrated. Of the 5 patients with progressive scarring, no vesicoureteric reflux was demonstrated on videourodynamics.
There was no evidence of either renal calculi or persistent hydronephrosis in any of the renal units with the exception of one patient who had undergone a urinary diversion 18 years after her SCI. This particular patient developed bilateral hydronephrosis and bilateral renal calculi requiring treatment, but no obstruction of her upper tracts on isotope renogram.
Discussion
Renal scarring in patients with SCI is secondary to a multifactorial process. An indwelling catheter is associated with bacteriuria in more than 90% of patients within 4 weeks of its insertion.6 Furthermore, in the SCI population, the presence of an indwelling catheter increases the risk of renal scarring and injury as demonstrated by long-term studies,2, 7 although some studies have not been able to find a correlation between catheterization and renal scarring.8 Vesicoureteric reflux also has a role in the pathogenesis of renal scarring. In children with neurogenic dysfunctional bladders, the risk of renal scarring has been found to be greater in those with reflux and asymptomatic bacteriuria than in those with bacteriuria alone.9 Vesicoureteric reflux in the SCI population is low however.10 A further factor associated with renal scar formation is the presence of neurogenic bladder dysfunction. Urodynamic studies have found that the presence of phasic detrusor contractions is associated with upper tract dilatation.11 Such high-pressure phasic contractions occur even in the presence of an indwelling catheter.3
In the paediatric population with renal scars associated with reflux, the incidence of new renal scars diminishes with age. However, irrespective of age, after the appearance of the initial renal scar, the development of further new renal scars is limited.12, 13 The International Reflux Study in Children reported that in the two arms of the study examining new and progressive scar formation in surgically and medically managed reflux in 321 children over a 5 year period, new scars developed in only 10% of children with pre-existing renal scars.13 Longer term studies have followed the progress of renal scars detected in children into adulthood. In one particular cohort, no new renal scars after puberty were reported in 226 adults who had vesicoureteric reflux as children.14 This has led to the proposition that maximal renal injury in children with reflux occurs with the first episode of upper tract infection.15 Few studies have examined the nature of renal scarring in SCI patients. In our study, only 15.6% of patient who developed renal scars demonstrated further progression of the scarring process. This seems to be in concordance with the findings in the paediatric population with reflux and renal scars. Also of note is the finding that although the use or nonuse of indwelling catheterization was evenly distributed in the group of patients with stable renal scars, all those with progressive renal scarring used indwelling catheters as their method of urinary drainage and none demonstrated reflux on their urodynamic studies. This did not reach statistical significance possibly because of the low number of patients in this group.
Conclusions
Renal scarring in a patient with SCI can occur many years after the injury to the spine, but when it does occur it is unlikely to be a progressive process. The vast majority of scars occur as a single event. However, when there is progression of the scarring process, there is a possibility that it may be associated with long-term catherization. Therefore, until further data become available, it may be more appropriate to target closer radiological surveillance of the upper urinary tracts to those patients with a renal scar who have an indwelling catheter.
References
Dietrick RB, Russi S . Tabulation and review of autopsy findings in fifty five paraplegics. JAMA 1958; 166: 41–46.
Chao R, Clowers D, May M . Fate of upper urinary tracts in patients with indwelling catheters after spinal cord injury. Urology 1993; 42: 259–269.
Jamil F, Williamson M, Ahmed YS, Harrison SCW . Natural-fill urodynamics in chronically catheterised patients with spinal-cord injury. Br J Urol 1999; 83: 396–399.
Roebuck DJ, Howard RG, Metreweli C . How sensitive is ultrasound in the detection of renal scars? Br J Radiol 1999; 72: 345–348.
Brandt TD, Neiman HL, Calenoff L, Greenberg M, Kaplan PE, Nanninga J . Ultrasound evaluation of the urinary system in spinal-cord-injury patients. Radiology 1981; 141: 473–477.
Warren JW . Catheter associated urinary tract infections. Inf Dis Clin Am 1987; 1: 823–853.
Larsen LD, Chamberlin DA, Khonsari F, Ahlering TE . Retrospective analysis of urologic complications in male patients with spinal cord injury managed with and without indwelling urinary catheters. Urology 1997; 50: 418–422.
Dewire DM, Owens RS, Anderson GA, Gotlieb MS, Lepor H . A comparison of the urological complications associated with long-term management of quadriplegics with and without chronic indwelling urinary catheters. J Urol 1992; 147: 1069–1072.
Ottolini MC, Shaer CM, Rushton HG, Majd M, Gonzales EC, Patel KM . Relationship of asymptomatic bacteriuria and renal scarring in children with neuropathic bladders who are practicing clean intermittent catheterisation. J Pediatr 1995; 127: 368–372.
Staskin D . Hydronephrosis after spinal cord injury. Urol Clin Am 1991; 18: 309–316.
Webb R, Griffiths CJ, Ramsden PD, Neal DE . Ambulatory monitoring of bladder pressure in low compliance neurogenic bladder dysfunction. J Urol 1992; 148: 1477–1481.
Shimada K, Matsui T, Ogino T, Ikoma F . New development and progression of renal scarring in children with primary vesicoureteral reflux. Int Urol Nephrol 1989; 21: 153–158.
Obling H et al. Renal scars and parenchymal thinning in children with vesicoureteral reflux: a 5-year report of the International Reflux Study in Children (European branch). J Urol 1992; 148: 1653–1656.
Smellie JM, Hodson CJ, Edwards D . Clinical and radiological features of urinary tract infection in childhood. BMJ 1964; 2: 1222.
Thomas DFM . Vesicoureteric reflux. In: Thomas DFM, Rickwood AMK, Duffy PG (eds). Essentials of Paediatric Urology. Martin Dunitz: London 2002, pp 45–55.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Edhem, I., Harrison, S. Renal scarring in spinal cord injury: a progressive process?. Spinal Cord 44, 170–173 (2006). https://doi.org/10.1038/sj.sc.3101831
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101831
